Klima-, Energi- og Bygningsudvalget 2013-14
KEB Alm.del Bilag 157
Offentligt
Noise from wind turbines and risk of cardiovascular diseaseThe number and size of wind turbines has increased markedly during the last decades. Although research hasconsistently found that traffic noise increases the risk for cardiovascular disease (1-4), potential effects of wind turbinenoise on risk for cardiovascular disease are virtually unexplored.
The aimof this project is to investigate if exposure to wind turbine noise is associated with an increased risk forcardiovascular disease using unique Danish registers. We will investigate if:acute exposure to wind turbine noise triggers myocardial infarction and strokelong-term exposure to wind turbine noise increases the risk of cardiovascular disease
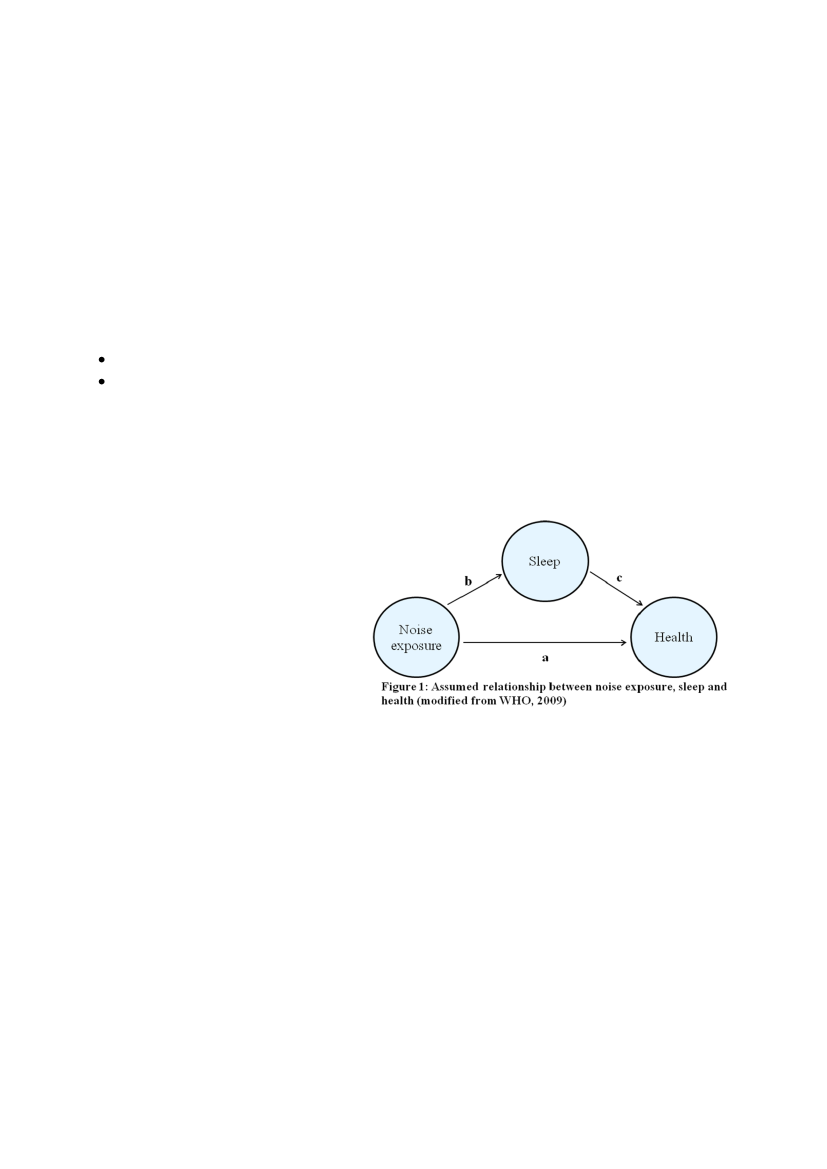
BACKGROUNDHearing is a permanent process essential for human survival and communication. However, the human organism is notable to shut off noise and therefore noise can have a number of unwanted effects, such as reduction of fidelity ofcommunication, interference with cognitive processes and disturbance of sleep.Figure 1 shows two pathways through whichnoise exposure can affect human health: directly(a) and indirectly via sleep disturbance (b + c) (5).Noise acts as a stressor and, according to thegeneral stress model, provokes a typical stressresponse, including hyperactivity of thesympathetic autonomic nervous system andactivation of the hypothalamus–pituitary– adrenalaxis, resulting in vasoconstriction, increased blood pressure, increased heart rate and high levels of the glucocorticoidcortisol (6, 7). Also, acute stress has been found to affect the immune system with increased levels of circulatinginflammatory factors such as IL-6 and IL-1β (8).Exposure to noise during night-time is thought particularly hazardous (5). Studies have shown that noise at night causesa full range of sleep disturbance from minor unconscious autonomic perturbations, such as sleep stage changes andbody movements, to full awakening (9-11). Sleep disturbance has been associated with changes in physiologicalparameters, such as metabolic and endocrine function (12, 13) and altered immune defense, such as increased levels ofimmunoglobulins (14, 15).Longer term exposure to noise from road traffic and airports has consistently been found to increase the risk ofcardiovascular disease: hypertension, myocardial infarction (MI) and stroke (1-4). However, noise immission from windturbines and traffic are different, which highlights the need for research of potential cardiovascular health effects of windturbine noise. Firstly, wind turbine noise levels are generally low compared to traffic noise levels in urban settings. InDenmark wind turbines emits max. 44 dB whereas for road traffic noise approximately one third of all Danish dwellingare exposed to more than 58 dB (Lden). Also, as the sound power level from a wind turbine depends on the wind velocity,1
the immission levels vary irregularly (16), whereas traffic noise usually are more constant and predictable. In a recentstudy, Janssen et al. found that wind turbine noise induced a higher proportion of annoyed residents than traffic noisedoes at comparable sound levels (16). Also, annoyance due to wind turbine noise was found at lower noise levels thantraffic noise. However, the study also showed that annoyance was lower among residents who received economicalbenefit from wind turbines (16).Wind turbine noise has been suggested to be associated with sleep disturbances, stress and general health, althoughresults are inconsistent (17-22). All these studies are cross-sectional and uses self-reported data on sleep, stress andhealth. Also, they are generally based on a small number of exposed persons. Some of these studies indicate thatassociations between wind turbine noise and sleep, stress and health are present only among annoyed people whereasthere seems to be no relationship between modeled/measured wind turbine noise and sleep disturbances, stress andhealth among people that report not be annoyed by noise from a nearby wind turbine(s) (18, 21). One study hasinvestigated associations between modeled wind turbine noise and self-reported cardiovascular disease and they foundno associations (19). However, the study was cross-sectional, based on self-reported cardiovascular disease, thenumber of persons with as well as the type of cardiovascular disease was not reported and results only adjusted for ageand sex, and therefore this hypothesis should be evaluated in a larger, more solid design, ideally a prospective studywhich is considered the best design for studying health effects of long-term exposure.Acute effects of noise on cardiovascular events are virtually unexplored, although noise-induced risk factors includingincreased blood pressure and inflammation are believed to be important in the trigger of a stroke and a MI (23, 24). Alarge day-to-day variation in noise exposure is needed to investigate acute effects. In contrast to traffic noise, windturbines noise is associated with considerable day-to-day variation, providing a unique opportunity to investigate whethernoise exposure trigger a cardiovascular eventimmediately after exposure.In Denmark we have unique opportunities to investigatewhether wind turbine noise affects the risk ofcardiovascular disease because Denmark has been apioneer in setting up wind turbines and therefore we canfollow the health effects of wind turbines over many years(Figure 2), and secondly because Denmark has uniquenational registers that enables us to trace the addressesof all Danish citizens since 1971 and all hospitaladmissions for cardiovascular disease since 1977.
Figure 2Growth in number of wind turbines in Denmark (modifiedfrom energinet.dk)
METHODSExposure assessmentThe Danish Energy Agency and Energinet.dk have established a register of all Danish wind turbines. This register isupdated monthly, and contains information on all wind turbines back to 1980 including the exact location of each windturbine (geographical coordinate), date of grid connection, cancelation date for decommissioned turbines, manufacture,type, hub height and diameter of rotor blades. The registry contains data for approximately 5,000 wind turbines inoperation and 2,500 cancelled wind turbines.2
There is a clear association between wind velocity and the noise emitted from a wind turbine which is characteristic andavailable for each type of wind turbine (25). We will use these data to develop a model for noise immission from all typesof wind turbines at all wind velocities. Based on these modeled noise levels for each turbine we will identify all dwellingswithin the immission area of wind turbine noise using geographical information system (GIS), and the noise level at eachdwelling will then be calculated using the distance between the wind turbine and the dwelling. It will in many cases benecessary to calculate the noise contributions from several wind turbines, which will then be summed for each dwelling.Nord2000 is a highly accurate method for calculation of noise, verified by controlled measurements includingmeasurements of wind turbine noise (26). As calculations with Nord2000 are very time consuming and costly, we will usea simplified version of the method described in details in “Vindmøllebekendtgørelsen” from the Danish EPA (27). Weconsider this method to be well fitted for the considerable number of calculations needed for this project. In addition, wewill correct all modeled values for the attenuation that occurs when sound propagates in headwind (see appendix 1).Simulated wind speed and direction time series at each wind turbine location in Denmark back to 1980 will be producedbased on the mesoscale wind analysis method developed by DTU Wind Energy and used in many studies (28-30).These data will be provided at a spatial resolution of approximately 5 km and downscaled to each required location at a1-hour or 3-hour resolution and at different levels, including 10 m above ground and hub height. The wind analysismethod makes use of the advanced Weather Research and Forecasting (WRF) model (31) and a dynamic downscalingatmospheric reanalysis technique (32).Sub-study 1: Day-to-day variation in wind turbine noise and risk for cardiovascular diseasePrevious studies on traffic noise and risk of cardiovascular disease have focused on long-term noise exposure. Onereason is that there is little day-to-day variation in exposure to traffic noise. In contrast, exposure to noise from windturbines is associated with considerable day-to-day variation, which gives us a unique opportunity to investigate whethernoise exposure can lead to MI or stroke immediately after exposure.Study population and designBased on modeled noise immission from all types of wind turbines (see exposure section) we will identify all residentialaddresses within the immission area using GIS and the official Danish address database (Den OffentligeInformationsserver (OIS),www.ois.dk).Subsequently, we will identify all persons who have lived at those addresses inthe period 1980-2012 by linking the addresses with the Danish civil registration system, thereby retrieving their uniquepersonal identification number (33). We will include all persons above 25 years of age at start of exposure (set up of newturbine or moving into a noise immission area) who were exposed to noise from wind turbines in more than one year inthe period from 1980 to 2012. We estimate that this will sum up to approximately 10,000–15,000 persons. This estimateis based on the following: 1) 7,500 wind turbines in Denmark (total of turbines in operation and cancelled), 2) for mostsingle wind turbines there will be one dwelling just below the noise limit value, as this determines the dimensions of theturbine and the required distance to dwellings, 3) for smaller groups of wind turbines (typically 3-5) we estimate that 2-3dwellings will be exposed just below the noise limit value, 4) for large wind farms with up to 100 turbines we estimate that3-10 dwellings will be exposed just below the noise limit value, and 5) for both single and multiple wind turbine areas weexpect that in many cases there will also be dwellings within the immission area but at lower exposure than the limitvalue.We will identify the persons among this exposed population that have been hospitalized at least once with stroke and/orMI during the maximum of 32 years we follow them. We estimate that this will sum up to approximately 2,000 relevant3
hospitalizations during the study period based on information on number of yearly events of the two diseases(www.hjerteforeningen.dk). We use stroke and MI as endpoints as we have previously found road traffic noise toincrease the risk for these diseases (3, 4). Information on hospitalization for stroke (International Classification ofDisease (ICD) 10: I61, I63 and I64) and MI (ICD10: I21.0-I21.9) in the period 1980-2012 for all exposed persons will thenbe collected from the Danish National Patient Registry (34), and information on death will be collected from the Danishregister of causes of death (35) using the personal identification number. For all exposed cases with MI/stroke we willcalculate equivalent continuous A-weighted wind turbine sound pressure level (LAeq) at their residence for the each day(Ld; 07:00–19:00 h), evening (Le; 19:00–22:00 h) and night (Ln; 22:00–07:00 h) as described in the exposure section. Thelow time resolution enables us to investigate health effects of wind turbine noise at different times of the day, which is ofgreat interest as one hypothesis is that exposure during night is particular hazardous (5).We will use a case-crossover design, where we estimate the relationship between day-to-day variability in wind turbinenoise at each address and day-to-day variation in hospitalizations for cardiovascular disease (stroke and MI) amongpeople exposed to wind turbines noise. In a case-crossover study the noise exposure of a case person on the day ofhospitalization (and a few days before) is compared with noise exposure during a control period. The advantage of thedesign is that each person is their own control and differences in socio-economic status and lifestyle factors areaccounted for via the study design.Daily variations in air pollution and outdoor temperature could potentially confound the results. The majority of all Danishwind turbines are placed in rural settings where air pollution levels are mainly determined by the regional backgroundcontribution. Department of Environmental Science at Aarhus University has historical daily measurements on regionalair pollution background levels as well as temperature which will be included in this study.Statistical analysesWe will estimate risk using conditional logistic regression and compare the noise exposure on the day a person ishospitalized with stroke/MI (lag 0) with the noise level on the same weekday within the same month (3 control days), withadjustment for regional background air pollution and temperature. In addition, we will analyze various other time-windows of wind turbine noise: on the previous day and up to 4 days (lag 4) before stroke/MI hospitalization and theaccumulated exposure over 5 days (lag 0 – 4) as well as exposure at daytime (07:00–19:00 h), evening (19:00–22:00 h)and night (22:00–07:00 h).
Sub-study 2: Long-term exposure to wind turbine noise and risk for cardiovascular diseaseWe will use the unique Danish registers on wind turbines, residential addresses, health and socioeconomic status toconduct the first prospective study ever on effect of long-term exposure of noise from wind turbines on risk forcardiovascular disease.Study population and designThe study population will consist of the 10,000-15,000 people (above 25 years of age) in Denmark who lived in dwellingswithin a noise immission area of one or more wind turbines in 1980-2012 (described in sub-study 1) as well asadditionally 30,000 unexposed persons living just outside the noise immission areas of wind turbines, giving us a totalstudy population of 40,000-45,000 persons.
4
We will identify all dwellings with exposure to wind turbinenoise as described in sub-study 1. We will then identifyunexposed persons using GIS and the official Danish addressdatabase (OIS) to identify dwellings within an area ofapproximately three times the distance from the wind turbineas for the exposed dwellings (Figure 3).We will then identify all persons (above 25 years of age) whohave lived in dwellings within the outer geographical circle(Figure 3) in the period between 1980 and 2012 by linking theaddresses with the Danish civil registration system, therebyFigure 3Identification of the unexposed population.retrieving their unique personal identification number (33).Similarly to the exposed population, we will only include persons who have lived at least one year at these addresses.By chosing this strategy for selection of an unexposed population, we will identify a population that are more similar tothe exposed population than if we had chosen a random sample of 30,000 Danes.We will determine the mobility of both the exposed and the unexposed population and based on this set up a strategy forhandling moving out of the geographical areas, e.g. if the mobility is low we will exclude all cohort members who livedless than 80 % of the follow-up time in residences within the included geographical areas.Information on hospitalization for cardiovascular disease (ICD10: I00-I99) in the period from 1977 to 2012 for these40,000-45,000 persons will subsequently be found by linking their personal identification number to the Danish NationalPatient Registry (34). Furthermore, information on death will be collected from the Danish register of causes of death(35). We will exclude all participants hospitalized with cardiovascular disease before moving into dwellings within thegeographical circles used in this study. We estimate that approximately 9,000 persons will be hospitalized with incidentcardiovascular disease during the study period based on information on number of yearly incident cardiovascular events(www.hjerteforeningen.dk). We will generate sub-groups of cardiovascular diseases to be used in the statisticalanalyses: MI (ICD10: I21.0-I21.9; approximately 1,500 cases), atrial fibrillation and flutter (ICD10: I48; approximately3,000 cases), heart failure (ICD10: I50; approximately 1,000 cases) and stroke (ICD10: I61, I63 and I64; approximately2,000 cases).We will use the wind turbine noise exposure data modeled for sub-study 1, and calculate 1- and 5-years averages foreach person (see statistical section). We will investigate effects of whole day exposure as well as for nighttime exposure.To be able to adjust all statistical analyses for socioeconomic status we will link the personal identification number of allpopulation members to Statistic Denmark (36) to collect information on level of education, individual and householdincome, affiliation to the work market and cohabiting status.Exposure to road traffic noise and/or air pollution could potentially confound the results. We have previously developed aGIS road network with traffic data for the period 1960–2005 (37). We will use this database together with the geocode ofall dwellings in the study to derive three variables indicating the amount of traffic near each dwelling: distance to a roadwith a traffic density > 10,000 vehicle/day (major road), and two variables summarizing the total amount of kilometersdriven by vehicles within 200 m and 500 m, respectively, of the residence each day as the product of street length andtraffic density added up for all street lines within a 200/500 m circle around the address.
5
Statistical analysesStatistical analyses will be based on a Cox proportional hazards model with age as the underlying time, which ensurescomparison of individuals of the same age (38). We will use left truncation at age of enrolment into the population(January 1st 1985 (to allow for calculation of 5 year exposure preceding event), moving into an area close to a windturbine (figure 3) or setting up of new wind turbine), so that people will be considered at risk from enrolment into thecohort, and end of follow-up at the age at diagnosis of a cardiovascular disease (event), death or December 31th 2012,whichever came first.Exposure to wind turbine noise will be modeled as time-weighted averages the preceding 1- and 5-years at a given age.These exposures (1- and 5-years) will be entered as time-dependent variables into the statistical risk model, thus foreach incident cardiovascular event recalculating exposure for all population members at exactly the same age as thecase and at risk at the time of the hospitalization for cardiovascular disease. Time-weighted averages will be calculatedbased on 1) whole day exposure and 2) only nighttime exposure.Estimates will be calculated crude and adjusted for a priori defined potential confounders: sex, level of education,calendar year, individual and household income, affiliation to the work market and cohabiting status. We will also adjustfor distance to major road and traffic load within 200 m and 500 m of the residence as proxies for air pollution and roadtraffic noise.We have calculated the power of this study based on a population of 40,000 where one third of the population isexposed. We have a statistical power of >90 % to detect associations of 1.10, 1.15 and 1.20 for all cardiovasculardiseases (9,000 cases), atrial fibrillation and flutter (3,000 cases) and MI (1,500 cases), respectively. Proc power, SASversion 9.2, was used for these calculations.
SIGNIFICANCE AND DISSEMINATIONExposure to wind turbine noise is suspected of affecting health and concern for this is increasing among people livingclose to wind turbines. However, very limited scientific data exists on effect of noise from wind turbines and risk forcardiovascular disease or other major diseases. This study will therefore be among the first contributing to answer thequestion of whether noise from wind turbines affects the risk of a major disease and has the potential to contribute inproviding guidance on regulations for human habitation close to wind turbines.Results will be published in international peer-reviewed journals and presented to the general population throughnational media and popular science articles.
FEASIBILITYThe Danish Cancer Society research group members have many years of experience in conducting environmentalepidemiology research, and have during the last years specialized in investigating health effects of noise. We expect noproblems in collecting and generating data and results for this study. Information on all Danish wind turbines is readilyavailable from The Danish Energy Agency and Energinet.dk. We have extensive experience in collecting, managing andanalyzing data from the national registers to be used in this study and expect no difficulties in gaining access to theseregisters or in obtaining permission from the Danish Data Protection Agency. We also have extensive experience in wind6
speed and traffic modelling and the applicant has already been in contact with two acoustical consultant agenciesinterested in modelling the wind turbine noise for the project. Many of the research group members have successfullycollaborated in several projects.
TIMELINESThe project runs for 24 months:Month 1:The Danish Cancer Society and DTU Wind Energy will meet with at least two acoustical consultantagencies to discuss and plan the wind turbine noise modeling. Based on this one consultant will beselected and a contract written and signed.The Danish Cancer Society will apply the Danish Data Protection Agency and national registers (OIS,Statistic Denmark and ‘Statens Serum Institut’) for permissions for use of data for the study.The consultant agency will generate a model for noise immission from all types of wind turbines to beused for identifying the exposed Danish dwellings.DTU Wind Energy will model wind speed and direction time series at each wind turbine location.Based on the modeled noise immission data the Danish Cancer Society will use the Danish addressdatabase (OIS) to identify addresses of all Danish dwellings exposed to wind turbine noise as well asunexposed dwellings for sub-study 2. Subsequently, these addresses will be linked to the Danish civilregistration system, followed by linkage to Danish National Patient Registry, Danish register of causes ofdeath and Statistic Denmark.Based on wind modeling data and addresses of all exposed Danish dwellings the consultant agency willmodel wind turbine noise for all exposed dwellings.Department of Environmental Science, Aarhus University, will generate traffic proxies and obtaininformation on historical background air pollution and temperature measurements.The Danish Cancer Society will conduct the statistical analyses of sub-study 1.The Danish Cancer Society will conduct the statistical analyses of sub-study 2.The Danish Cancer Society will write scientific papers with input from all other research group members.
Month 2-3:Month 2-6:Month 4-5:
Month 7-9:
Month 10-15:Month 16-20:Month 16-24:
THE RESEARCH GROUPThe highly interdisciplinary research team will be headed by the applicant Mette Sørensen. The expertise of the teamincludes noise exposure, wind energy, register-based health research, use of GIS and biostatistics:Mette Sørensen,PhD, senior researcher in the environment and cancer research group at the Danish Cancer Society,has many years of experience in environmental epidemiology. Since 2008 her research has focused on health effects oftraffic noise, which among others have resulted in publications that as the first ever showed exposure to road trafficnoise to be associated with risk for stroke and diabetes (3, 39). In March 2012 she received a 5-year starting grant fromthe European Research Council to investigate health consequences of noise exposure from road traffic (QUIET).7
Ole Raaschou-Nielsen,PhD, head of the environment and cancer research group at the Danish Cancer Society, hasmany years of experience in health effects of traffic pollution, and participates in designing the study, choosingconsultant agency, dialog with consultant agency etc.Rikke Nordsborg,PhD student in the environment and cancer research group at the Danish Cancer Society. Rikkemastered in geography and has extensive experience in the use of GIS. She will be responsible for identification ofdwellings in the vicinity of wind turbines using GIS, and for identifying persons living in the dwellings during the studyperiod and link them to national registry data.Alfredo Peña,PhD, senior scientist at DTU Wind Energy has extensive experience in wind resource assessment, windpower meteorology and meso-scale modeling. He will be responsible for providing the simulated wind speed anddirection time series at the wind turbine locations.All statistical analyses will be conducted by astatistician/epidemiologistwho will be employed at the Danish CancerSociety.Responsible for the modeling of wind turbine noise will be aconsultant agencywith extensive expertise within the areaof wind turbine noise. To ensure the best value for money at least two consultant agencies will be approached.Matthias Ketzel,PhD Senior Scientist, Department of Environmental Science, Aarhus University has extensiveexperience in air pollution modeling and will be responsible for generating traffic proxies and historical backgroundconcentrations of air pollution.
8
REFERENCES
1. Babisch W. Transportation noise and cardiovascular risk: updated review and synthesis of epidemiological studiesindicate that the evidence has increased, 2006. Noise Health 8:1-292. Babisch W. Road traffic noise and cardiovascular risk, 2008. Noise.Health 10:27-333. Sorensen M, Hvidberg M, Andersen ZJ, et al. Road traffic noise and stroke: a prospective cohort study, 2011. EurHeart J 32:737-7444. Sorensen M, Andersen ZJ, Nordsborg RB, et al. Road traffic noise and incident myocardial infarction: aprospective cohort study, 2012. PlosONE 7:e392835. World Health Organization Regional Office for Europe. 2009. Night noise guidelines for Europe6. Lusk SL, Gillespie B, Hagerty BM, Ziemba RA. Acute effects of noise on blood pressure and heart rate, 2004.Arch.Environ.Health 59:392-3997. Wagner J, Cik M, Marth E, et al. Feasibility of testing three salivary stress biomarkers in relation to naturalistictraffic noise exposure, 2010. Int.J Hyg.Environ Health 213:153-1558. Steptoe A, Hamer M, Chida Y. The effects of acute psychological stress on circulating inflammatory factors inhumans: a review and meta-analysis, 2007. Brain Behav.Immun. 21:901-9129. Haralabidis AS, Dimakopoulou K, Velonaki V, et al. Can exposure to noise affect the 24 h blood pressure profile?Results from the HYENA study, 2010. J Epidemiol.Community Health10. Griefahn B, Brode P, Marks A, Basner M. Autonomic arousals related to traffic noise during sleep, 2008. Sleep31:569-57711. Miedema HM, Vos H. Associations between self-reported sleep disturbance and environmental noise based onreanalyses of pooled data from 24 studies, 2007. Behav.Sleep Med. 5:1-2012. Ekstedt M, Akerstedt T, Soderstrom M. Microarousals during sleep are associated with increased levels of lipids,cortisol, and blood pressure, 2004. Psychosom.Med. 66:925-93113. Stamatakis KA, Punjabi NM. Effects of sleep fragmentation on glucose metabolism in normal subjects, 2010.Chest 137:95-10114. Wright CE, Erblich J, Valdimarsdottir HB, Bovbjerg DH. Poor sleep the night before an experimental stressorpredicts reduced NK cell mobilization and slowed recovery in healthy women, 2007. Brain Behav.Immun. 21:358-36315. Hui L, Hua F, Diandong H, Hong Y. Effects of sleep and sleep deprivation on immunoglobulins and complement inhumans, 2007. Brain Behav.Immun. 21:308-31016. Janssen SA, Vos H, Eisses AR, Pedersen E. A comparison between exposure-response relationships for windturbine annoyance and annoyance due to other noise sources, 2011. J.Acoust.Soc.Am. 130:3746-375317. Pedersen E, Waye KP. Perception and annoyance due to wind turbine noise--a dose-response relationship, 2004.J.Acoust.Soc.Am. 116:3460-34709
18. Pedersen E, Persson WK. Wind turbine noise, annoyance and self-reported health and well-being in differentliving environments, 2007. Occup.Environ.Med. 64:480-48619. Pedersen E. Health aspects associated with wind turbine noise - Results from three field studies, 2011. NoiseControl Engineering Journal 59:47-5320. Shepherd D, McBride D, Welch D, Dirks KN, Hill EM. Evaluating the impact of wind turbine noise on health-related quality of life, 2011. Noise.Health 13:333-33921. Bakker RH, Pedersen E, van den Berg GP, Stewart RE, Lok W, Bouma J. Impact of wind turbine sound onannoyance, self-reported sleep disturbance and psychological distress, 2012. Sci.Total Environ. 425:42-5122. Nissenbaum MA, Aramini JJ, Hanning CD. Effects of industrial wind turbine noise on sleep and health, 2012.Noise.Health 14:237-24323. McColl BW, Allan SM, Rothwell NJ. Systemic infection, inflammation and acute ischemic stroke, 2009.Neuroscience 158:1049-106124. Biasucci LM, Leo M, De Maria GL. Local and systemic mechanisms of plaque rupture, 2008. Angiology 59:73S-76S25. Søndergaard B, Henningsen P. Generelle data om støjen fra ældre vindmøller, 2011. Miljøstyrelsen MiljøprojektNr. 1398:26. Søndergaard B, Plovsing B, Sørensen T. Validation of the Nord2000 propagation model for use on wind turbinenoise, 2009. PSO-07 F&U project no.7389 Final report:1-5327. Miljøministeriet. Bekendtgørelse om støj fra vindmøller, 2012.https://www.retsinformation.dk/Forms/R0710.aspx?id=13965828. Hahmann AN, Lange J, Pena A, Hasager CB. The NORSEWInD numerical wind atlas for the South Baltic, 2012.DTU Wind Energy.DTU Wind Energy E, no 0011(EN).29. Pena A, Gryning S-E, Hahmann AN. Observations of the atmospheric boundary layer height under marineupstream flow conditions at a coastal site, 2013. J.Geophysical Research 118:1924-194030. Marinelli M, Maule P, Hahmann AN, Isleifsson FR, Nørgård P, Cutululis.N.A. Wind and photovoltaic large scaleregional models for hourly production evaluation, IEEE transaction on sustainable energy, 2013. In preparation31. Skamarock WC, Klemp JB, Dudhia J, et al. A description of the advanced research WRF version 3, 2008.NCAR/TN-475+STR Mesoscale and microscale meteorology division, National Center for Atmospheric Research,Boulder, Colorado, USA, 113pp:32. Hahmann AN, Rostkier-Edelstein D, Warner TT, et al. A reanalysis system for the generation of mesoscaleclimatographies, 2010. J Applied Meteorol Climatol 49:954-97233. Pedersen CB. The Danish Civil Registration System, 2011. Scand.J.Public Health 39:22-2534. Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register, 2011. Scand.J.Public Health 39:30-3335. Helweg-Larsen K. The Danish Register of Causes of Death, 2011. Scand.J.Public Health 39:26-2936. Thygesen LC, Daasnes C, Thaulow I, Bronnum-Hansen H. Introduction to Danish (nationwide) registers on healthand social issues: structure, access, legislation, and archiving, 2011. Scand.J.Public Health 39:12-1610
37. Jensen SS, Hvidberg M, Pedersen J, et al. GIS-based national street and traffic data base 1960-2005 (In Danishwith English summary), 2009. National Environmental Research Institute, Aarhus University, Roskilde NERITechnical Report No. 678:38. Thiebaut AC, Benichou J. Choice of time-scale in Cox's model analysis of epidemiologic cohort data: a simulationstudy, 2004. Stat.Med. 23:3803-382039. Sorensen M, Andersen ZJ, Nordsborg RB, et al. Long-term exposure to road traffic noise and incident diabetes: acohort study, 2013. Environ.Health Perspect. 121:217-222
11