Sundheds- og Forebyggelsesudvalget 2012-13
SUU Alm.del Bilag 321
Offentligt
Mad, ilt, motion ogmentalfunktion • Næring ogenergi mod ADHDUmahro CadoganAdjungeret professor, Nutrition and FunctionalMedicine, University of Western States
1
2
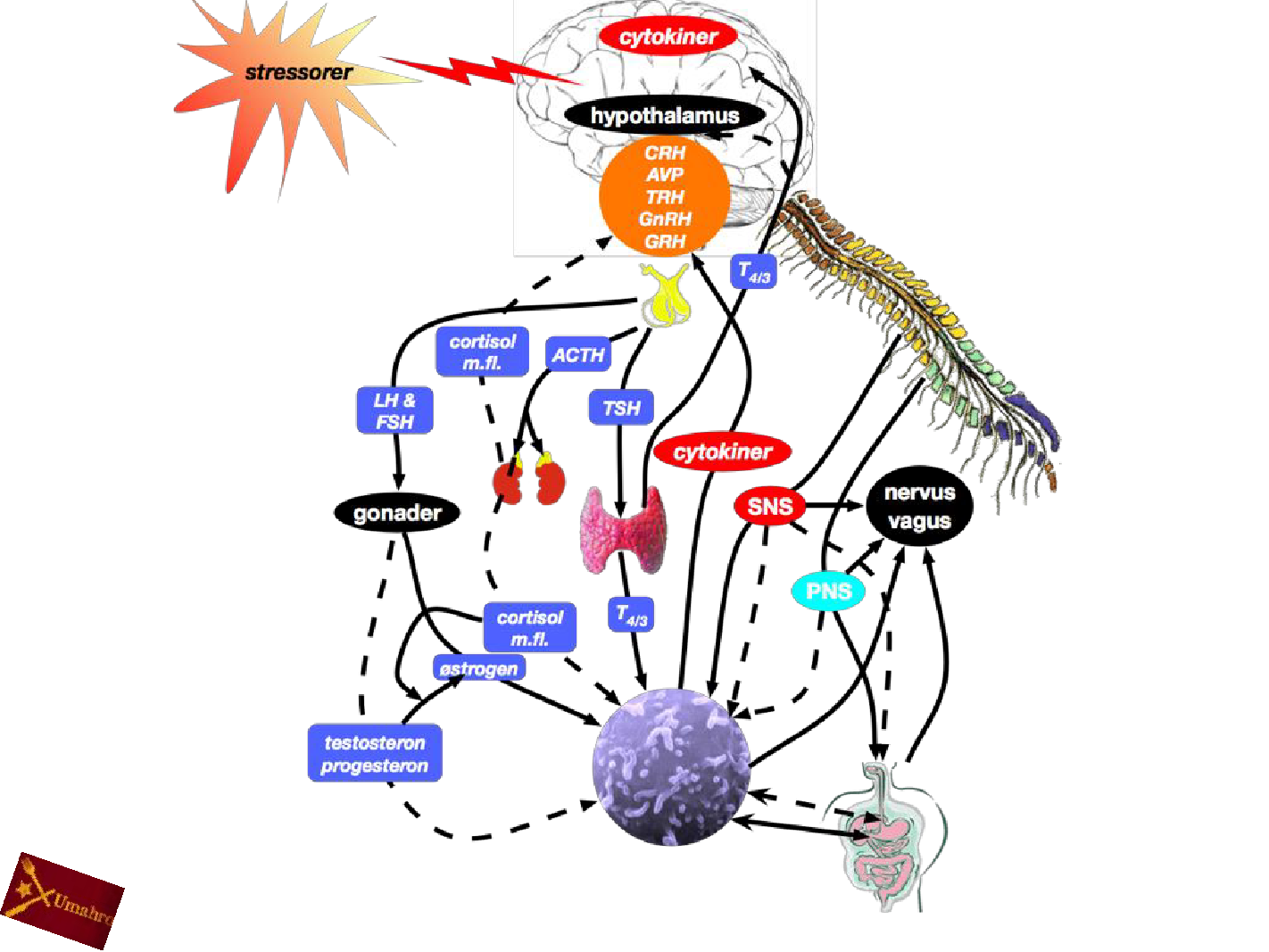
Basalt om hjernen60% fedt i tørvægt70% vand20-25% af ilt og blodsukkerDen skal have nok luft og konstant jævntblodsukkerDen skal være ordentligt hydreretDen er også meget krævende hvad angårvitaminer, mineraler, sporstoffer og fedtHos voksne udgør hjernen mindre end 2% afkropsvægten…men den bruger store mængder afden ilt vi indånder og store mængder af blodsukkeret
3
Hjernens behov
4
5
6
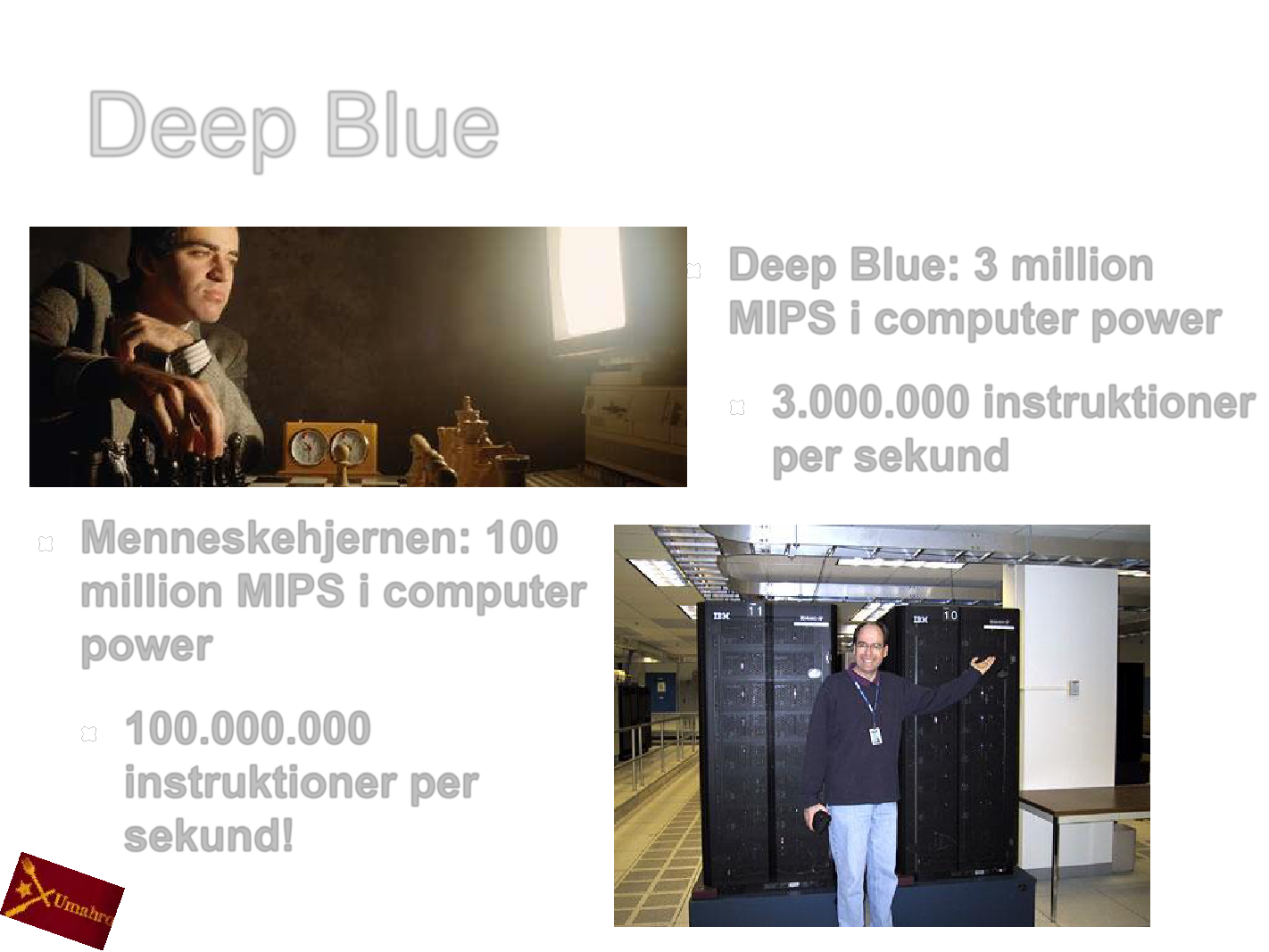
Deep BlueDeep Blue: 3 millionMIPS i computer power3.000.000 instruktionerper sekundMenneskehjernen: 100million MIPS i computerpower100.000.000instruktioner persekund!7
8
9
10
11
Neuroplasticitet
12
Hjernen er “formbar”
13
14
Blinde kan se med tungen!
15
Forskningsresultater
16
Influences of micronutrient and omega-3 fatty acidsupplementation on cognition, learning, and behavior:methodological considerations and implications for childrenand adolescents in developed societies
Forskning antyder at børn i industrisamfundscorer højere på tests af ikke-verbal intelligensog har forbedret adfærd, efter de har fåetThe strongest effects were observed in trials that lasted over 3 months and invitamin-of children with low socioeconomic status, symptoms of attentionsubgroupsog mineraltilskud med eller udendeficit hyperactivity disorder, and/or learning disabilities.omega-3 fedtsyrer (fiskeolie), sammenlignetFuture studies should focus on children and adolescents who have a lowmed dem der fårare likelyitoforsøg der varede i meresocioeconomic status orsetbe sufferingStørst effekt blevplacebo…nutritional deficiencies todetermine the impact of vitamin and mineral supplements with or without n-3end 3supplementation on theirundergrupper af børnThesePUFAmåneder og icognitive and behavioral functioning.medstudies should ideally include blood sample analyses to help determine iflav socio-økonomisk status, tegn på ADHDnutritional status influences the response to supplementation and whetherchanges inindlæringsproblemer…blood status account for effects on cognition and behavior.og/ellerFrensham LJ, Bryan J, Parletta N. (2012)Nutr Rev.70(10): 594-610
Existing evidence suggests that children and adolescents in developed countriesmay perform better on tests of nonverbal intelligence and on behavioralmeasures after receiving vitamin and mineral supplements with or without n-3PUFA supplementation compared with those receiving placebo, regardless ofage and supplementation formula.
17
18
KUNylig gennemgang af forskningen i sammenhængenmellem kost og ADHDPositive trendsEliminationsdiætSund madOmega-3 fedtsyrerZink og jern ved mangel/utilstrækkelighedScanBrit også omtalt19
Omega-3 Fatty Acid Supplementation for theTreatment of Children With Attention-Deficit/Hyperactivity Disorder Symptomatology:Systematichave demonstrated differences in omega-3 fatty acid composition in plasma andSeveral studiesReview and Meta-Analysisin erythrocyte membranes in patients with attention-deficit/hyperactivity disorder (ADHD)compared with unaffected controls. Omega-3 fatty acids have anti-inflammatory properties andcan alter central nervous system cell membrane fluidity and phospholipid composition. Cellmembrane fluidity can alter serotonin and dopamine neurotransmission. The goal of this meta-analysis was to examine the efficacy of omega-3 fatty acid supplementation in children withADHD.Ten trials involving 699 children were included in this meta-analysis. Omega-3 fatty acidsupplementation demonstrated a small but significant effect in improving ADHD symptoms.Eicosapentaenoic acid dose within supplements was significantly correlated with supplementefficacy. No evidence of publication bias or heterogeneity between trials was found.Conclusion: Omega-3 fatty acid supplementation, particularly with higher doses ofeicosapentaenoic acid, was modestly effective in the treatment of ADHD. The relative efficacy ofomega-3 fatty acid supplementation was modest compared with currently availablepharmacotherapies for ADHD such as psychostimulants, atomoxetine, or α2 agonists. However,given its relatively benign side-effect profile and evidence of modest efficacy, it may bereasonable to use omega-3 fatty supplementation to augment traditional pharmacologicinterventions or for families who decline other psychopharmacologic options.Bloch MH, Qawasmi A (2011)Journal of the American Academy of Child & AdolescentPsychiatry16 August EPub ahead of print20
The ScanBrit randomised, controlled, single-blindstudy of a gluten- and casein-free dietaryintervention for children with autism spectrumdisordersThere is increasing interest in the use of gluten- and casein-free diets for children with autism spectrum disorders (ASDs).We report results from a two-stage, 24-month, randomised, controlled trial incorporating an adaptive 'catch-up' designand interim analysis.Stage 1 of the trial saw 72 Danish children (aged 4 years to 10 years 11 months) assigned to diet (A) or non-diet (B)groups by stratified randomisation. Autism Diagnostic Observation Schedule (ADOS) and the Gilliam Autism Rating Scale(GARS) were used to assess core autism behaviours, Vineland Adaptive Behaviour Scales (VABS) to ascertaindevelopmental level, and Attention-Deficit Hyperactivity Disorder - IV scale (ADHD-IV) to determine inattention andhyperactivity.Participants were tested at baseline, 8, and 12 months. Based on per protocol repeated measures analysis, data for 26diet children and 29 controls were available at 12 months. At this point, there was a significant improvement to mean dietgroup scores (time*treatment interaction) on sub-domains of ADOS, GARS and ADHD-IV measures.
Surpassing of predefined statistical thresholds as evidence of improvement in group A at 12 months sanctioned the re-assignment of group B participants to active dietary treatment. Stage 2 data for 18 group A and 17 group B participantswere available at 24 months. Multiple scenario analysis based on inter- and intra-group comparisons showed someevidence of sustained clinical group improvements although possibly indicative of a plateau effect for intervention.Our results suggest that dietary intervention may positively affect developmental outcome for some children diagnosedwith ASD. In the absence of a placebo condition to the current investigation, we are, however, unable to disqualifypotential effects derived from intervention outside of dietary changes.Whiteley P, Haracopos D, Knivsberg AM, Reichelt KL, Parlar S, Jacobsen J, Seim A, Pedersen L, Schondel M, ShattockP. (2010)Nutr Neurosci.13(2): 87-100.
21
Alterations of the intestinal barrier in patientswith autism spectrum disorders and in theirfirst-degree relativesOBJECTIVES: Intestinal permeability (IPT) was investigated in patients with autism as well as in theirfirst-degree relatives to investigate leaky gut hypothesis. Faecal calprotectin (FC) was also measuredin patients with autism, either with or without gastrointestinal symptoms, and in their first-degreerelatives.PATIENTS AND METHODS: IPT results, assessed by means of the lactulose/mannitol test, werecompared with adult and child controls and with FC values.RESULTS: A high percentage of abnormal IPT values were found among patients with autism(36.7%) and their relatives (21.2%) compared with normal subjects (4.8%). Patients with autism on areported gluten-casein-free diet had significantly lower IPT values compared with those who were onan unrestricted diet and controls. Gastrointestinal symptoms were present in 46.7% of children withautism: constipation (45.5%), diarrhoea (34.1%), and others (alternating diarrhoea/constipation,abdominal pain, etc: 15.9%). FC was elevated in 24.4% of patients with autism and in 11.6% of theirrelatives; it was not, however, correlated with abnormal IPT values.CONCLUSIONS: The results obtained support the leaky gut hypothesis and indicate that measuringIPT could help to identify a subgroup of patients with autism who could benefit from a gluten-free diet.The IPT alterations found in first-degree relatives suggest the presence of an intestinal (tight-junctionlinked) hereditary factor in the families of subjects with autism.de Magistris L, Familiari V, Pascotto A, Sapone A, Frolli A, Iardino P, Carteni M, De Rosa M,Francavilla R, Riegler G, Militerni R, Bravaccio C. (2010) J Pediatr Gastroenterol Nutr. 2010Oct;51(4):418-24.
22
Effects of a restricted elimination diet on the behaviour ofchildren with attention-deficit hyperactivity disorder (INCAstudy): a randomised controlled trialThe effects of a restricted elimination diet in children with attention-deficit hyperactivity disorder (ADHD) havemainly been investigated in selected subgroups of patients. We aimed to investigate whether there is aconnection between diet and behaviour in an unselected group of children.The Impact of Nutrition on Children with ADHD (INCA) study was a randomised controlled trial that consisted ofan open-label phase with masked measurements followed by a double-blind crossover phase.…In the open-labelphase (first phase), children aged 4—8 years who were diagnosed with ADHD were randomly assigned to 5weeks of a restricted elimination diet (diet group) or to instructions for a healthy diet (control group). Thereafter,the clinical responders (those with an improvement of at least 40% on the ADHD rating scale [ARS]) from the dietgroup proceeded with a 4-week double-blind crossover food challenge phase (second phase). During the firstphase, only the assessing paediatrician was masked to group allocation. During the second phase (challengephase), all persons involved were masked to challenge allocation. Primary endpoints were the change in ARSscore between baseline and the end of the first phase (masked paediatrician) and between the end of the firstphase and the second phase (double-blind), and the abbreviated Conners' scale (ACS) score (unmasked)between the same timepoints. The primary analyses were intention to treat for the first phase and per protocol forthe second phase.100 children were enrolled and randomly assigned to the control group (n=50) or the diet group (n=50). Betweenbaseline and the end of the first phase, the difference between the diet group and the control group in the meanARS total score was 23¶7 (95% CI 18¶6—28¶8; p<0¶0001) according to the masked ratings. The differencebetween groups in the mean ACS score between the same timepoints was 11¶8 (95% CI 9¶2—14¶5; p<0¶0001).The ARS total score increased in clinical responders after the challenge by 20¶8 (95% CI 14¶3—27¶3; p<0¶0001)and the ACS score increased by 11¶6 (7¶7—15¶4; p<0¶0001). In the challenge phase, after challenges…relapseof ADHD symptoms occurred in 19 of 30 (63%) children…. There were no harms or adverse events reported…A strictly supervised restricted elimination diet is a valuable instrument to assess whether ADHD is induced byfood.Lidy M Peiser et al.The Lancet,Volume 377, Issue 9764, Pages 494 - 503, 5 February 201123
Effects of a few food diet inattention deficitadisorderof hyperactiveSeventyeight children, referred to diet clinic becausebehaviour, were placed on a 'fewfoods' elimination diet. Fifty nineimproved in behaviour during this open trial. For 19 of these children it waspossible to disguise foods or additives, or both, that reliably provokedbehavioural problems by mixing them with other tolerated foods and to testtheir effect in a placebo-controlled double blind challenge protocol. Theresults of a crossover trial on these 19 children showed a significant effectfor the provoking foods to worsen ratings of behaviour and to impairpsychological test performance. This study shows that observations ofchange in behaviour associated with diet made by parents and otherpeople with a role in the child's care can be reproduced using double-blindmethodology and objective assessments.Clinicians should give weight to the accounts of parents and
consider this treatment in selected children with a suggestive
medical history.
CM Carter et al.Archives of Disease in Childhood1993; 69: 564-56824
The Role of Histamine Degradation GenePolymorphisms in Moderating the Effects of FoodAdditives on Children's ADHD SymptomsFood additives can exacerbate ADHD symptoms and cause non-immunoglobulin E-dependent histamine release…However, children vary in the extent to which their ADHDsymptoms are exacerbated by the ingestion of food additives. The authors hypothesized thatgenetic polymorphisms affecting histamine degradation would explain the diversity ofresponses to additives. METHOD: In a double-blind, placebo-controlled crossover trial,challenges involving two food color additive and sodium benzoate (preservative) mixtures ina fruit drink were administered to a general community sample of 3-year-old children(N=153) and 8/9-year-old children (N=144). An aggregate ADHD symptom measure (basedon teacher and parent blind ratings of behavior, blind direct observation of behavior in theclassroom, and—for 8/9-year-old children only—a computerized measure of attention) wasthe main outcome variable. RESULTS: The adverse effect of food additives on ADHDsymptoms was moderated by histamine degradation gene polymorphisms HNMT T939C andHNMT Thr105Ile in 3- and 8/9-year-old children and by a DAT1 polymorphism (short versuslong) in 8/9-year-old children only…CONCLUSIONS: Histamine may mediate the effects offood additives on ADHD symptoms, and variations in genes influencing the action ofhistamine may explain the inconsistency between previous studies. Genes influencing arange of neurotransmitter systems and their interplay with environmental factors, such asdiet, need to be examined to understand genetic influences on ADHD symptoms.
25
Differences between the gut microflora ofchildren with autistic spectrum disorders andthat of healthy childrenAbstract: Children with autistic spectrum disorders (ASDs) tend to suffer from severegastrointestinal problems. Such symptoms may be due to a disruption of the indigenous gut florapromoting the overgrowth of potentially pathogenic micro-organisms. The faecal flora of patientswith ASDs was studied and compared with those of two control groups (healthy siblings andunrelated healthy children). Faecal bacterial populations were assessed through the use of aculture-independent technique, fluorescence in situ hybridization, using oligonucleotide probestargeting predominant components of the gut flora. The faecal flora of ASD patients contained ahigher incidence of the Clostridium histolyticum group (Clostridium clusters I and II) of bacteriathan that of healthy children. However, the non-autistic sibling group had an intermediate level ofthe C. histolyticum group, which was not significantly different from either of the other subjectgroups. Members of the C. histolyticum group are recognized toxin-producers and may contributetowards gut dysfunction, with their metabolic products also exerting systemic effects. Strategiesto reduce clostridial population levels harboured by ASD patients or to improve their gutmicroflora profile through dietary modulation may help to alleviate gut disorders common in suchpatientsHelena MRT Parracho, Max O Bingham, Glenn R Gibson and Anne L McCartney
26
Gastrointestinal MicrofloraStudiesofin Late-Onsetmay involve abnormalAutismSome cases late-onset (regressive) autismflora because oral vancomycin, which is poorly absorbed, may lead tosignificant improvement in these children. Fecal flora of children withregressive autism was compared with that of control children, andclostridial counts were higher. The number of clostridial species foundin the stools of children with autism was greater than in the stools ofcontrol children. Children with autism had 9 species of Clostridium notfound in controls, whereas controls yielded only 3 species not found inchildren with autism. In all, there were 25 different clostridial speciesfound. In gastric and duodenal specimens, the most striking finding wastotal absence of non—spore-forming anaerobes and microaerophilicbacteria from control children and significant numbers of such bacteriafrom children with autism. These studies demonstrate significantalterations in the upper and lower intestinal flora of children with late-onset autism and may provide insights into the nature of this disorder.Sidney Finegold et. al.27
Desulfovibrio species are potentiallyimportant in regressive autismAutism is a complex disorder with no specific diagnostic test so the disease is defined by its characteristicsincluding cognitive defects, social, communication and behavioral problems, repetitive behaviors, unusualsensitivity to stimuli such as noise, restricted interests, and self stimulation. The incidence of this disease hasincreased remarkably in recent years and was 110/10,000 children (∼1%) in multiple areas of the US in 2007. Thefinancial burden on families and communities is enormous. In terms of predisposing factors, heredity plays a rolein some subjects, but it is clear that environmental factors are also important. Environmental toxins can affect theimmune system adversely. Intestinal bacteria are recognized by a few investigators as potentially important andwe have proposed that certain antimicrobial drugs may be a key factor in modifying the intestinal bacterial floraadversely, selecting out potentially harmful bacteria that are normally suppressed by an intact normal intestinalflora. We had felt that clostridia in the gut might be involved in autism because they are virulent organisms andspore-formers; spores would resist antibacterial agents so that when antibiotics were discontinued the sporeswould germinate and by toxin production or another mechanism lead to autism. However, a recent study of oursemploying the powerful pyrosequencing technique on stools of subjects with regressive autism showed thatDesulfovibrio was more common in autistic subjects than in controls. We subsequently confirmed this with pilotcultural and real-time PCR studies and found siblings of autistic children had counts of Desulfovibrio that wereintermediate, suggesting possible spread of the organism in the family environment. Desulfovibrio is an anaerobicbacillus that does not produce spores but is nevertheless resistant to aerobic and other adverse conditions byother mechanisms and is commonly resistant to certain antimicrobial agents (such as cephalosporins) often usedto treat ear and other infections that are relatively common in childhood. This bacterium also produces importantvirulence factors and its physiology and metabolism position it uniquely to account for much of thepathophysiology seen in autism. If these results on Desulfovibrio are confirmed and extended in other studies,including treatment trials with appropriate agents and careful clinical and laboratory studies, this could lead tomore reliable classification of autism, a diagnostic test and therapy for regressive autism, development of avaccine for prevention and treatment of regressive autism, tailored probiotics/prebiotics, and importantepidemiologic information.Sidney Finegold et al. Med Hypotheses. 2011 Aug;77(2):270-4. Epub 2011 May 17.28