Socialudvalget 2012-13
SOU Alm.del Bilag 333
Offentligt



a: Health care challenges
Despite a rise in obesity and lifestyle diseases because of a more westernized lifestyle,adult obesity in Japan is still low compared to other OECD countries.1Age-adjustedmortality and infant mortality has decreased, while life expectancy has improved.2The most immediate challenge to the Japanese health care system of is the multipleeffects of demographic change.Japan is a rapidly aging society with a total fertility rate of 1,39 and a life expectancyof 83,9 years.3As a result Japan experienced negative population growth in the late2000’s,4and now 24,1% of the total population are aged 65 or older.5Thesedemographic trends are expected to continue an the Japanese government estimates apopulation decline to 97 million by 2050, of which 38,8 % will be over 65 years old.6This means that a shrinking working population will have to take care of anincreasing population of elderly. A smaller workforce will put the Japanese economyunder pressure,7 8at a time where spending on health care and welfare are expected torise. On top of this, there will also be a shortage of workers to provide care for theelderly.Traditionally the older generations have been living with their family and receivedcare from their children, especially the daughters or daughters-in-law.9Home-basedcare is still the norm, with 83% of the 5,06 million people certified as requiring long-term care lived at home in 2010.10Of the total population over 65, 41% still live withtheir family, and 20% of the primary carers of frail elderly are daughters-in-laws.11The carers (both formal and informal) are overwhelmingly female and 50% of themare over 60 years old.12As immigration control is strict, it is hard to import foreign labour to the welfaresector. Furthermore public opinion is divided on foreign workers in welfare, withmany preferring raising the age of retirement, mobilization of female workers andhigher efficiency achieved through use of welfare technology.13 14Mariko Nishikitani, Shinobu Tsurugano, Mariko Inoue, Eiji Yano (2012). Effect of unequalemployment status on workers’ health: Results from a Japanese national survey, Social Science &Medicine 75 (2012), p 4392http://www.oecd.org/els/health-systems/BriefingNoteJAPAN2012.pdf3CIA world fact book https://www.cia.gov/library/publications/the-world-factbook/geos/ja.html4The Organisation for Economic Co-operation and Development (OECD) http://www.oecd-ilibrary.org/economics/country-statistical-profile-japan_20752288-table-jpn5http://www.stat.go.jp/data/jinsui/2012np/index.htm6Ministry of Internal Affairs and Communicationhttp://www.stat.go.jp/english/data/handbook/c02cont.htm7Eberstadt, Nicholas (2010).8Hewitt, Paul S. (2002).9Tamiya Nanako et al (2011). Population ageing and wellbeing: lessons from Japan’slong-term care insurance policy, in www.thelancet.com, Vol 378 September 24, 2011, p 118710http://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/dl/ri_130311-01.pdf11Tamiya Nanako et al (2011). Population ageing and wellbeing: lessons from Japan’slong-term care insurance policy, in www.thelancet.com, Vol 378 September 24, 2011, pp 1183-4, 118712http://www.mhlw.go.jp/english/topics/elderly/care/2.html13Coulmas 200714Morgan 200111
The Japanese society needs systems thatEnable people over 65 to remain active in the workforceRelieve burdens of formal and informal carersSupport care at home - assistive livingSupport people suffering from geriatric diseases, such as dementia(Supporting childcare, edutainment)
2
b: Health care investment focus
The Japanese state have a history of investing in research and development of robottechnology, for example The Humanoid Project initiated in 1998 by the Ministry ofEconomy, Trade and Industry (METI).In 2007 the Shinzo Abe administration publishedInnovation 25,a vision of howinnovation in robotics, and especially household-robotics, would help reverse thedeclining birth-rate and help sustain the needs of the rising population of elderly.15The main actors on the welfare policy field is the Ministry of Health, Labour andWelfare (MHLW), METI and the semi-government organisation NEDO (the NewEnergy and Industrial Technology Development Organisation), with the latter twomost active in supporting and funding R&D. Lastly the Ministry of Land,Infrastructure, Transport and Tourism involved in cooperation with MHLW toconstruct housing for elderly.16In November 2012 METI and MHLW published a report on what they see as the fourkey areas of welfare and nursing robots:1. Robots/technology that relieve or assist carers when lifting and moving.2. Robots/technology that enable to move more freely, or help users transportitems.3. Robots/technology processing excretion4. Protective robots/technology aimed at users suffering from dementia.METI further pledges to work with NEDO and related organisations and corporationsto implementation of robot technology that meets the needs of the users and carers.17To support the 4 areas above, METI started a new program in March 2013 for“Promotion of Implementation and Development of Nursing Robots”, with a budgetof �3.26 billion (190 million DKKR) for the fiscal year of 2013. The program willsupport private companies in research and development and implementation of robottechnology that meets the needs of elderly people or carers, while working with theMinistry of Health, Labour and Welfare to create an environment for actual testingwere the nursing is provided.18Corporations and organisations based in Japan will beable to apply for up to �7 billion (4 million DKKR).191516
http://www.kantei.go.jp/jp/innovation/index.htmlhttp://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/dl/ri_130311-01.pdf17http://www.mhlw.go.jp/stf/houdou/2r9852000002p8sl.html18http://www.meti.go.jp/main/yosangaisan/fy2013/pdf/07.pdf19http://www.meti.go.jp/information/publicoffer/kobo/downloadfiles/k130325002_01.pdf
3
c: Health care structure
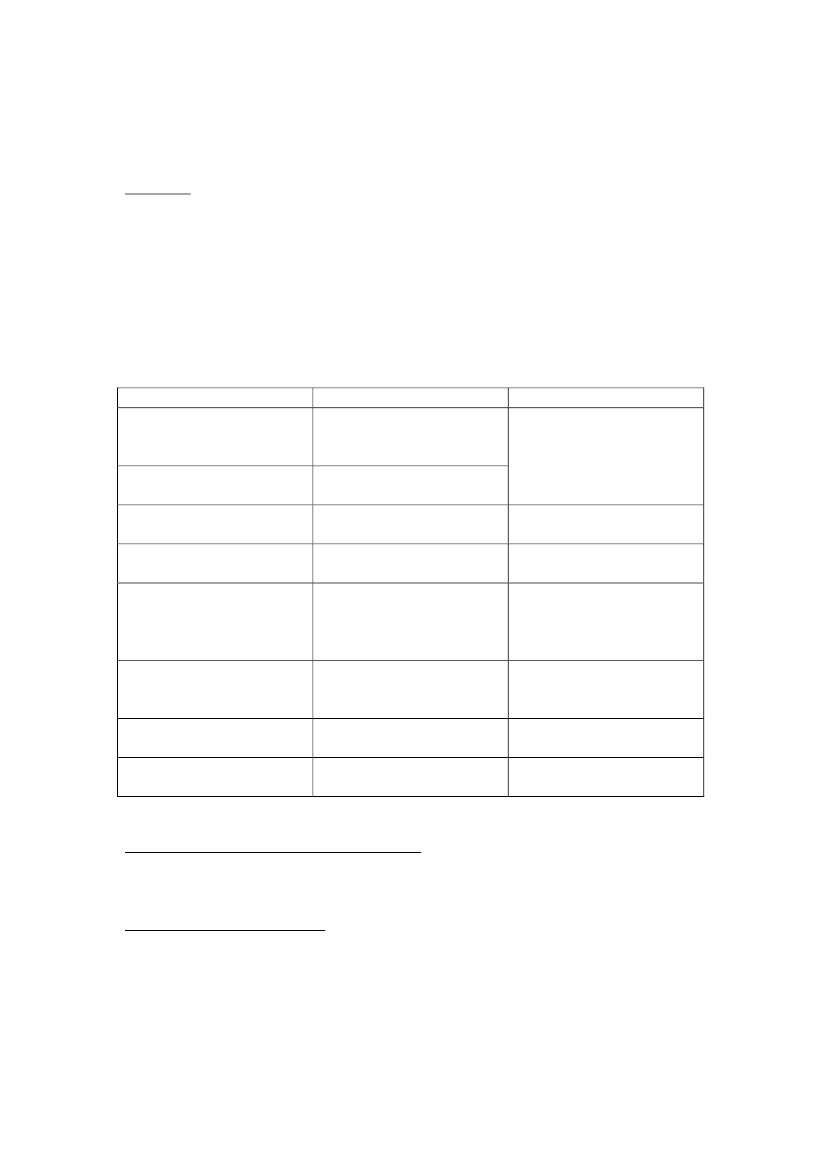
Japan has universal health care coverage through mandatory insurances.OverviewA 2011 survey shows that Japan has 8605 hospitals and 99.547 medical clinics.17,8% of the hospitals are national or public, 70,7% are driven by privateorganisations, 1,4% by organisations affiliated with the social insurance system and10% by others. 4,3% of the medical clinics are national or public, 83,4% are driven byprivate organisations, 0,6% by organisations affiliated with the social insurancesystem and 11,7% by others.20In 2010 Japan had 2,2 practicing physicians per 1000population, which is less than the OECD average of 3,1.21Investor-owned for-profithospitals are prohibited in Japan.22There are several types of housing and institutions for the elderly:23TypeRun byNumberIntensive care facilitiesLocal governments;6.213 (2010)special welfarecorporationsLong-term rehabilitationLocal governments;medical corporationsSanitary wards at hospitals Local governments;1.990 (2010)medical corporationsFee-based homeNo restriction (mainly5.232 (2010), 7,563business corporations)(2012)Moderate-fee home forLocal governments; social 2.114 (2010)low income elderlywelfare corporations;corporation approved byprefectural governmentsCare facility forLocal governments; social 978 (2010)environmentally andwelfare corporations;economically deprivedDementia group homesNo restriction (mainlyN/Abusiness corporations)Elderly housing with care No restriction (mainlyN/Abusiness corporations)Health Care – the National Health InsuranceVirtually all Japanese are covered through around 3500 health care plans according toplace of residence or place of work.24Citizens pay a premium according to theiremployment status and income. Municipalities act as insurers and administrators.2021
http://www.mhlw.go.jp/toukei/saikin/hw/iryosd/11/dl/1-1.pdfhttp://www.oecd.org/els/health-systems/BriefingNoteJAPAN2012.pdf
222324
http://content.healthaffairs.org/content/10/3/87.full.pdf p 89
http://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/dl/ri_130311-01.pdfFuture of Japan’s system of good health at low cost withequity: beyond universal coverageKenji Shibuya, Hideki Hashimoto, Naoki Ikegami, Akihiro Nishi, Tetsuya Tanimoto, Hiroaki Miyata,Keizo Takemi, Michael R Reich, www.thelancet.com Vol 378 October 1, 2011, p. 1266
4
Nationally the financing of health expenses are distributed in the following way:municipalities and prefectures 12,2%, state 25,9%, 20,1% by employers, 28,3% byinsurance premiums and 12,7% by patient co-payment.25Depending on familyincome and age he insured has to pay 20% or 30% of the medical fee, while the rest iscovered by the government.26Care for the elderlyThe Japanese state has supported older citizens for a long time. In the sixties it begansmall scale public funding for nursing homes and home-care, and in the 70’s itabolished medical co-payment for people 65, which resulted in a rise of socialadmissions, without much medical justification, into hospitals. Around 500.000elderly still live in special wards in hospitals. In 1989 the government initiated theGold Plan, with the goal of doubling institutional beds and tripling care services forolder people over 10 years. The Gold Plan struggled with administration problems,regional and local quality differences, and increasing spending.In 2000 it was replaced by a the public mandatory long-term care insurance (LTCI),which is financed 50% by taxes and 50% by premiums paid by Japanese aged 40 orolder. The LTCI is managed by the municipalities. Premiums are adjusted accordingto income.Japanese aged 65 years and older, or aged 40–64 years and suffering from geriatricdiseases, are entitled to LTCI services. Clients are categorized into one of sevengroups according to the level of their care needs. Each group sets a ceiling amount ofservices that can be purchased as benefits per month ranging from �53.200 (3.800DKKR) to �383.400 (27.383 DKKR). Clients pay a co-payment of around 10%.27 28LTCI covers institutional services, include nursing homes, homes with more medicalservice, chronic-care hospitals, out of home services such as day care centres,rehabilitation and short-stay respite care, and care at home such as home help services,at home nursing, bathing, remodelling, and rental of assistive devices.29A care manager draws a plan for the care. Care managers are required to take atraining corse and an exam. They are employed by a specialized agency or a serviceprovider. Their main tasks are to coordinate with different service providers, manageservice provision and reimbursement, and help recipients make decisions.30Clientschoose freely between providers.31Providers include local governments, semi-publicwelfare corporations, non-profit organisations, hospitals, and for-profit companies(for-profit companies are not allowed in institutional care). All providers are licensedand supervised by the local government. Service fees are set by the national
2526
http://www.mhlw.go.jp/seisakunitsuite/bunya/kenkou_iryou/iryouhoken/iryouhoken01/index.htmlhttp://www.its-kenpo.or.jp/html_main/h_b.html27Ministry of Health, Labour and Welfare http://www.mhlw.go.jp/english/topics/elderly/care/28Tamiya Nanako et al (2011). Population ageing and wellbeing: lessons from Japan’s long-term careinsurance policy, in www.thelancet.com Vol 378 September 24, 2011, pp. 1185 & 119029Ministry of Health, Labour and Welfare http://www.mhlw.go.jp/english/topics/elderly/care/2.html30Tamiya Nanako et al (2011). Population ageing and wellbeing: lessons from Japan’s long-term careinsurance policy, in www.thelancet.com Vol 378 September 24, 2011, p 118531Ishiguro Nobu (2012). ”Er valgfrihed altid ønskelig?”, Gerontologi Årgang 28, December 12, nr. 04,s. 16-17
5
government and revised every 3 years.32Once assessed as eligible, the client selects a care manager who draws up a care plan,setting the weekly schedule of care services.
32
Tamiya Nanako et al (2011). Population ageing and wellbeing: lessons from Japan’s long-term careinsurance policy, in www.thelancet.com Vol 378 September 24, 2011, p 1185
6
d: Health care company structure
Care technology marketAccording to a 2006 survey predicts that the Japanese market for partner robots (termcovering robots for entertainment, surveillance, cleaning, lifestyle support, educationand nursing care) will grow to 18,6 million units or �3,26 billion (187 million DKKR)by 2016.33METI estimates that the market for care alone will be �16,7 billion (970million DKKR) by 2015 and �400 billion (23,25 billion DKKR) by 2035.However, care technology is usually expensive, and therefore only implemented insome care facilities. METI and MWHL are working on expanding on expanding thepublic insurance to cover more welfare robots. The plan is to reimburse 9% of thecost.Because of the high pricing, most technology can also be leased. The walkingassistance suit HAL by Cyberdyne has an initial cost of about �550.000 (32.200DKKR) followed by a monthly fee of about �158.000 (9.250 DKKR) for 5 years.36MySpoon be SECOM will cost �399,000 (23.360 DKKR) to buy or �6.405 (375DKKR) pr. month for 5 years.37CompaniesIt is not easy to give a clear overview of the Japanese companies developing welfaretechnology as many of them also do many other things. The most famous companiesdeveloping partner and care robots, SONY (Aibo, Qrio), Mitsubishi Heavy Industries(Wakamaru), Honda (Asimo, walking assistance) and Toyota (walking assistance),are mainly known for other activities.Some of the smaller companies team up with larger ones to get promotion, e.g. AIST(Paro), Moritoh (Popo) and NWIC (Minelet) have teamed up with housing giantDaiwahouse for promotion and sales. Daiwahouse is also responsible for the sale ofWakamaru by Mitsubishi.38Some of the larger companies also offer care services, build and run care facilities, orsenior housing sell or lease care equipment, and even provide care managementsupport. These include Airwater (bathing system), SECOM (myspoon), Daiwahouse(represents Paro, HAL, POPO and more) and Panasonic.The technology is sold to private buyers and health care facilities. Many companiesask private persons to buy through their care organisation or care manager,39and willonly lease to institutions and organisations.40 413334
http://www.robocasa.com/pdf/press_release.pdfhttp://www.nikkei.com/article/DGXNASFS2901R_Z20C12A7MM8000/35http://www.nikkei.com/article/DGXNASFS2901R_Z20C12A7MM8000/36http://www.cyberdyne.jp/customer/index_3.html#cs0737http://www.secom.co.jp/personal/medical/myspoon.html38http://www.mhi.co.jp/products/detail/wakamaru_basic-package.html39http://www.cyberdyne.jp/robotsuithal/faq.html40http://www.cyberdyne.jp/customer/index_3.html#cs0741http://www.daiwahouse.co.jp/release/20121212093333.html
7
Technology is sold through organisations targeting the health and welfare markets42.They sell or lease a wide variety of equipment for care to institutions or privatecustomers. There are at least 7000 of these companies,43but not all sell products thatfall under the definition of welfare technology. Two examples are YamashitaCorporation44and Frontier,45and also Airwater who runs a chain called AI Land with27 stores.46List of companies:ActiveLink - lifting assistancehttp://psuf.panasonic.co.jp/alc/en/index.htmlAirwater - Bathing Systemhttp://www.awi.co.jp/english/business/medical/service.htmlAIST - Parohttp://www.aist.go.jp/aist_e/latest_research/2004/20041208_2/20041208_2.htmlHonda Motor Co. Ltd - Walking assistancehttp://www.honda.co.jp/robotics/Moritoh Corporation - Lift “popo”http://www.moritoh.co.jp/?page_id=10NWIC - Waste disposal system “Minelet”http://www.minelet.com/Panasonic - Robotic bed turned wheelchairhttp://panasonic.co.jp/ism/robot/robot01.htmlRIKEN – Riba transfer robothttp://rtc.nagoya.riken.jp/SAKAImed - Bathing systemhttp://www.sakaimed.co.jp/index.htmlSales on Demand - Representing iRobot47in Japanhttp://www.salesondemand.co.jp/Sanyo - Electronic bedhttp://www.sanyo-inc.co.jp/kaigo/SECOM co. ltd. - Eating assistant robot Myspoon42
The Japanese term for these businesses isfukushi yougu rentaru/hanbai jigyou()43http://www.mhlw.go.jp/toukei/saikin/hw/kaigo/service11/dl/sankou.pdf4445
http://www.yco.co.jp/service/homecare/service.htmlhttp://www.frontier-ph.com/homecare/kaigo/index.html46http://www.awi.co.jp/business/medical/welfare/tools.html47
iRobots cleaning robots are not particularly associated with care, and are sold in normal chain storesselling electronic equipment, tv’s, cameras etc.
8
http://www.secom.co.jp/home/TMSUK - Hospital care equipment, surveillance robothttp://www.tmsuk.co.jp/english/robots.htmlToyotahttp://www2.toyota.co.jp/en/news/11/11/1101.htmlToshibaCleaning robotshttp://www.toshiba.co.jp/living/lineup/cleaners/0163_k2_pic_01.html
9
e: Health care product approvals and acceptance
Certification of products in Japan falls into two categories: mandatory technicalstandards and non-mandatory voluntary standards.48Japanese Industrial Standards Mark (JIS) is a voluntary standard but it is used widely.Electrical appliances imported to Japan are subject to the Electrical Appliance andMaterial Safety Law and are required to get the Product Safety Electric Appliance andMaterials Mark (PSE).49Testing and certification in connection to JIS and PSE is carried out by government-approved third-body certifying organizations.There are a variety of organizations offering guidance, testing and certifications, e.g.:JET (Japan Electrical Safety & Environment Technology Laboratories)http://www.jet.or.jp/JQA (Japan Quality Assurance Organization)http://www.jqa.jp/english/index.htmlTÜV SÜD Grouphttp://www.tuv-sud.jp/english/eec/japanese_market.htmlUL Japanhttp://www.ul.com/japan/eng/pages/aboutus/Many of the certifying organizations also have their own voluntary quality orcostumer safety marks.There are also moves to bring Japanese standards into harmony with internationalstandards, and certification organizations usually offer to certify using ISO(International Organization for Standardizations) or IEC (InternationalElectrotechnical Commission) standards as well as Japanese ones.New standards for welfare technologyPart of METI’s “Promotion of Implementation and Development of Nursing Robots”is to develop assessment and standardization methods for safety and functions.METI proposes to base the safety standard on the ISO safety requirements for non-medical care robots ISO / DIS 13482, and the functional standard on the JIS standardsfor similar technology.50Although ISO / DIS 13482 is still under development,51JQA used this standard tocertify the first personal care robot (HAL by Cyberdyne) in February 2013.52Further informationFor further information on JIS:http://www.jisc.go.jp/eng/jis-mark/pdf/JISpamphlet.pdf4849http://ita.doc.gov/td/standards/Final%20Site/CCG/CCG%20PDFs/Japan.pdfhttp://www.meti.go.jp/english/policy/economy/consumer/pse/index.html50from http://www.meti.go.jp/information/publicoffer/kobo/k130325002.html51http://www.iso.org/iso/home/store/catalogue_tc/catalogue_detail.htm?csnumber=5382052http://www.jqa.jp/service_list/fs/topics/topics_fs_04.html
10
For full list of designated JIS certification bodies:http://www.jsa.or.jp/eng/jiscba/p4.aspFor further information on PSE:http://www.meti.go.jp/english/policy/economy/consumer/pse/index.html
11
KilderEberstadt, Nicholas (2010).* The Demographic Future,Foreign Affairs,Vol. 89Issue 6, Nov/Dec2010, pp 54-64. Hentet 5. april 2012. Link:http://search.ebscohost.com.ep.fjernadgang.kb.dk/login.aspx?direct=true&db=a9h&AN=54624934&site=ehost-liveHewitt, Paul S. (2002). ”Depopulation and ageing in Europe and Japan: Thehazardous transition to a labor shortage economy,”Internationale Politik undGesellschaft,Volume 1 2002, pp. 111-120. Hentet 7. april 2012. Link:http://www.fes.de/ipg/ipg1_2002/ZEITSCHRIFT.HTM
12