Udenrigsudvalget 2011-12
URU Alm.del Bilag 132
Offentligt
THE STATE OF THE WORLD’S CHILDREN2012
Children inan Urban World
EM28BAFebr RGua Ory ED2012
EM28BAFebr RGua Ory ED2012
THE STATE OF THEWORLD’S CHILDREN2012
EM28BAFebr RGua Ory ED2012
� United Nations Children’s Fund (UNICEF)February 2012
Permission is required to reproduce any part of thispublication. Permission will be freely granted toeducational or non-profit organizations. Others willberequested to pay a small fee. Please contact:Division of Communication, UNICEF3 United Nations Plaza, New York, NY 10017, USATel: +1 (212) 326-7434Email: [email protected]
This report and additional online content are availableat <www.unicef.org/sowc2012>.PerspectiveandFocusOnessays represent the personal views of theauthorsand do not necessarily reflect the position ofthe UnitedNations Children’s Fund.For corrigenda subsequent to printing,please see <www.unicef.org/sowc2012>.
For latest data, please visit <www.childinfo.org>.ISBN: 978-92-806-4597-2eISBN: 978-92-806-4603-0United Nations publication sales no.: E.12.XX.1
EM28BAFebr RGua Ory ED2012Photographs
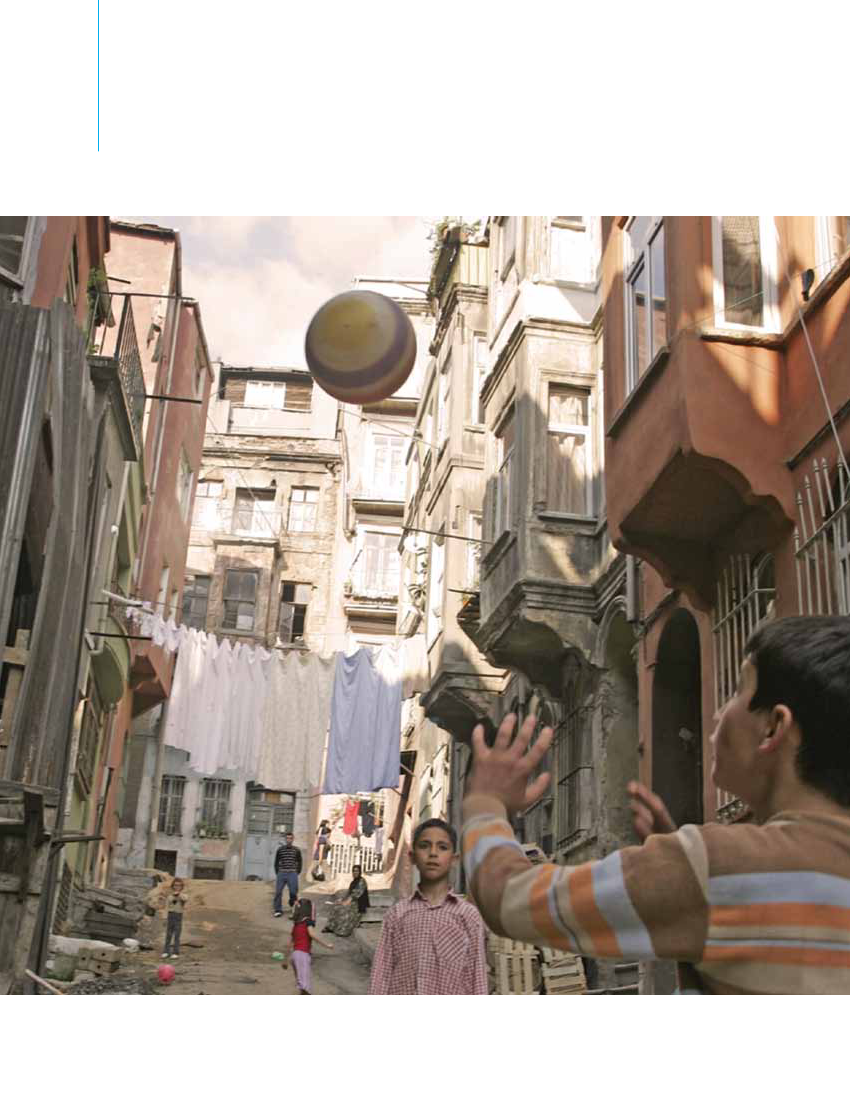
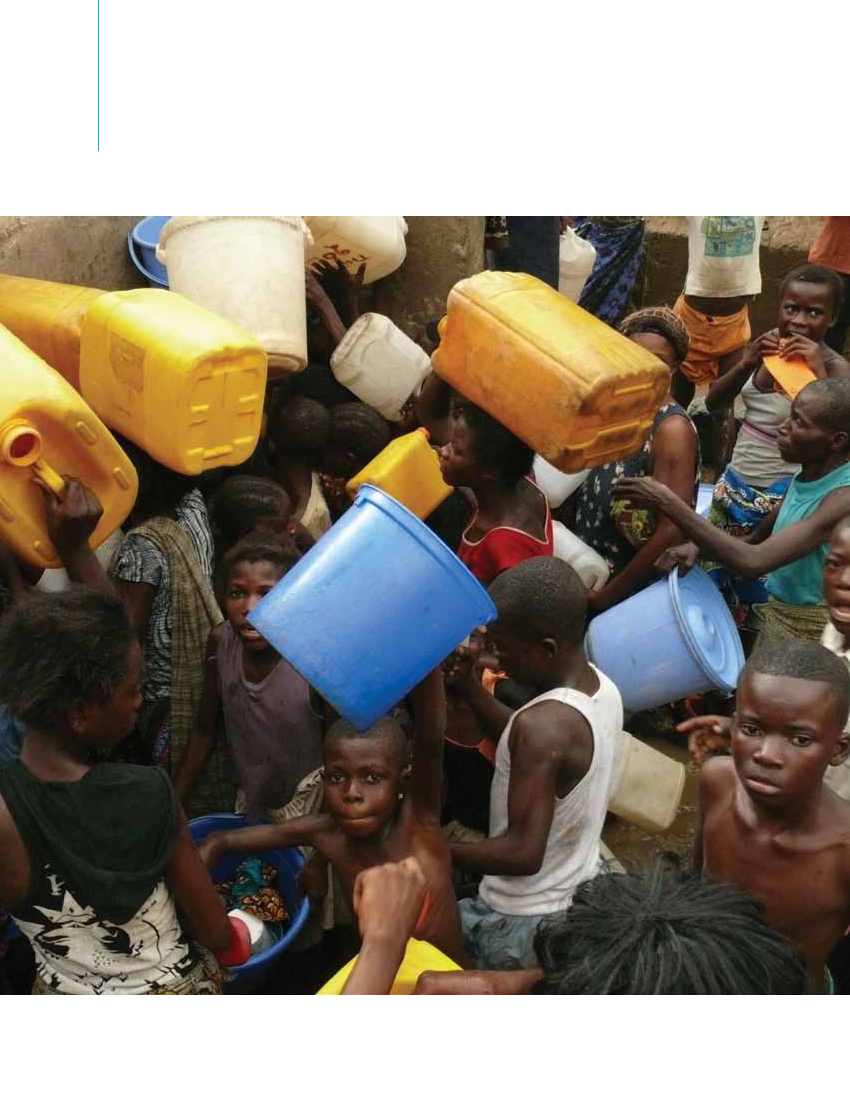
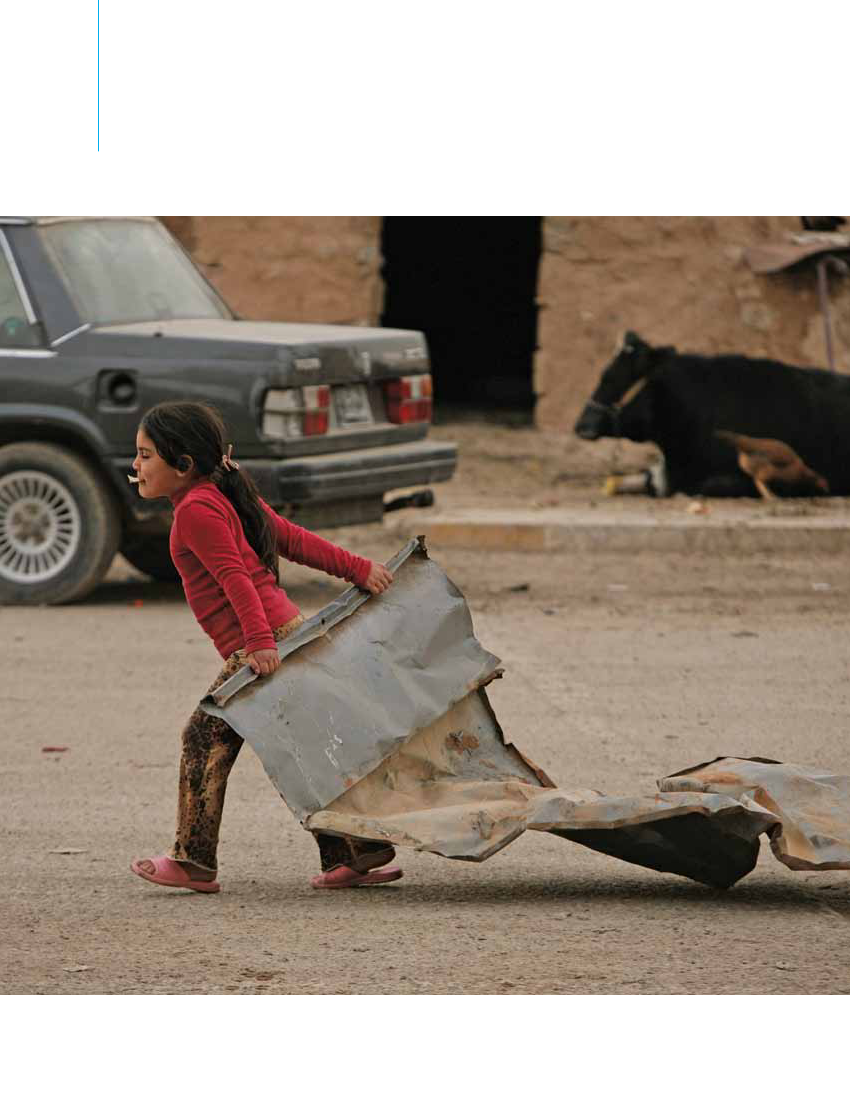
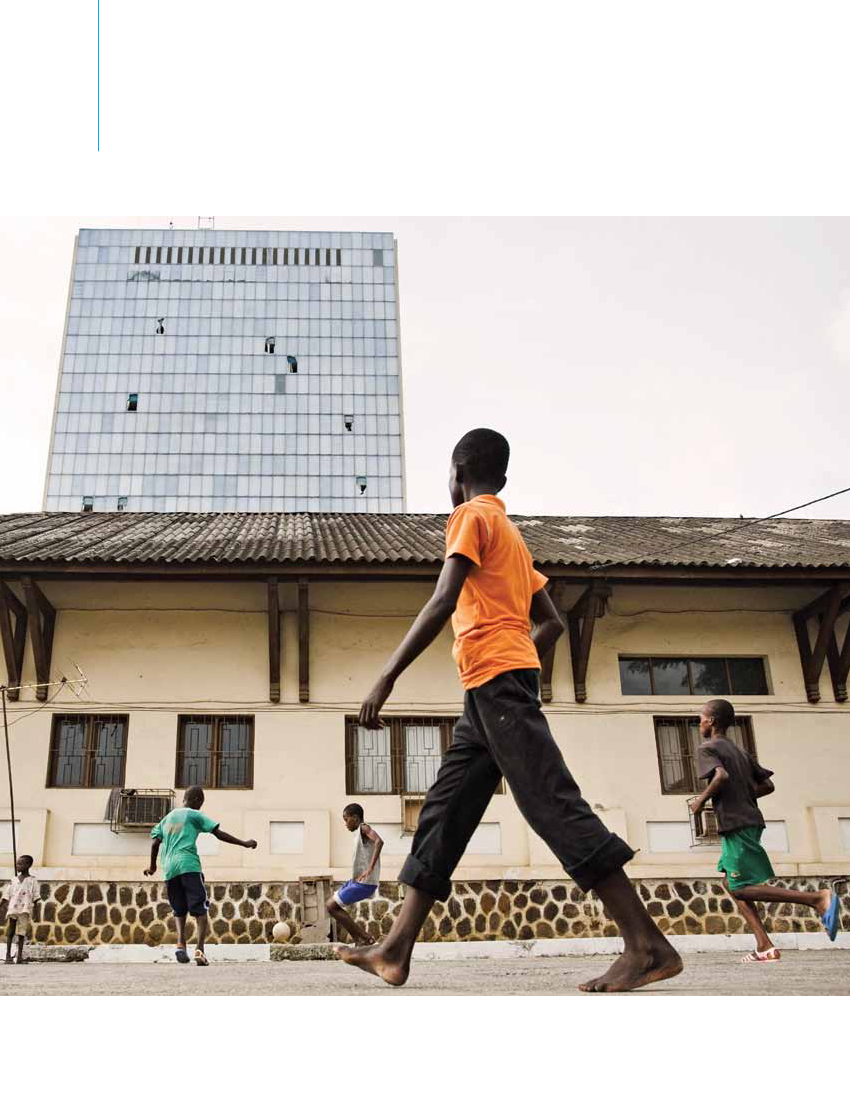
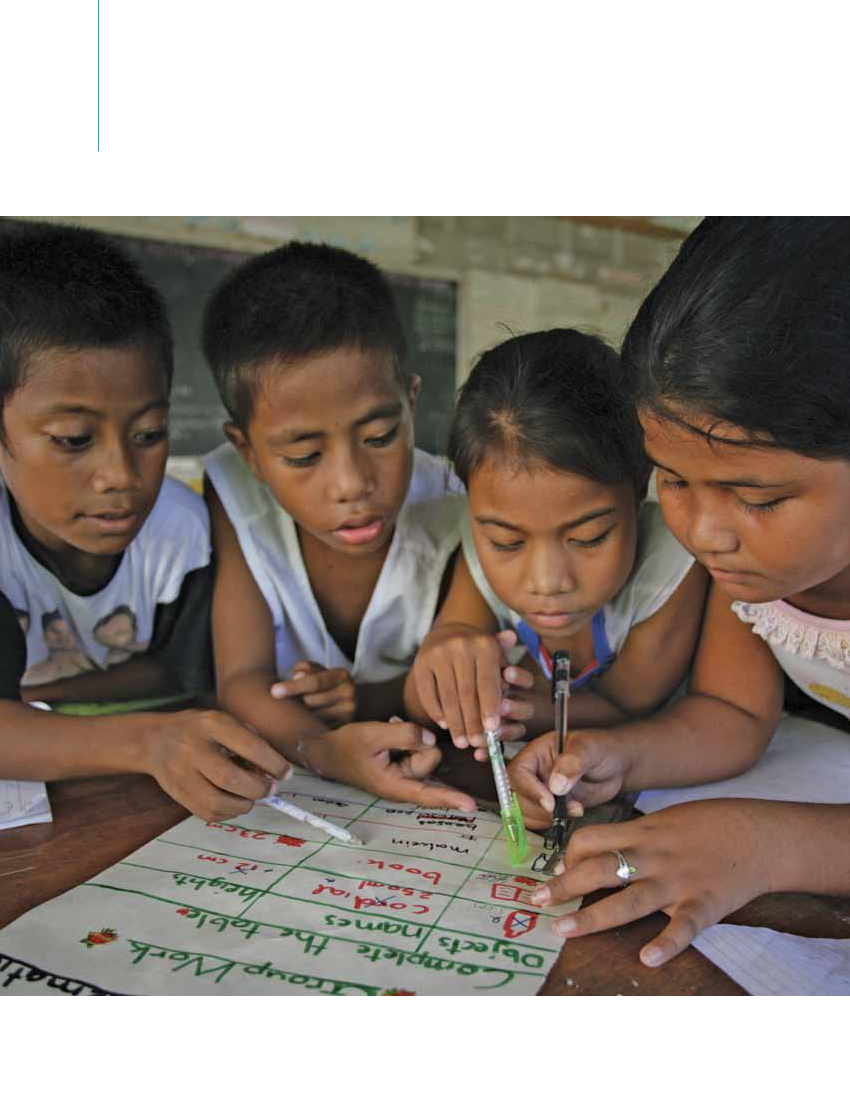
CoverChildren dance in an informal settlement ona hillsidein Caracas, Bolivarian Republicof Venezuela (2007).� Jonas Bendiksen/Magnum PhotosChapter 1, page xChildren play in Tarlabasi, a neighbourhood thatis home to many migrants in Istanbul, Turkey.� UNICEF/NYHQ2005-1185/Roger LeMoyneChapter 2, page 12Queuing for water at Camp Luka, a slum on theoutskirts of Kinshasa, Democratic Republic ofthe Congo.� UNICEF/NYHQ2008-1027/Christine NesbittChapter 3, page 34A girl in Kirkuk, Iraq, drags scrap metal that herfamily will use to reinforce their home – a smallspace with curtains for walls on the top floor ofa former football stadium.� UNICEF/NYHQ2007-2316/Michael KamberChapter 4, page 48Boys play football in the courtyard of the CentreSauvetage BICE, which offers residential andfamily services for vulnerable children in Abidjan,Côte d’Ivoire.� UNICEF/NYHQ2011-0549/Olivier AsselinChapter 5, page 66Girls and boys work on a group project in a primaryschool in Tarawa, Kiribati.� UNICEF/NYHQ2006-2457/Giacomo Pirozzi
ACkNOWLEDGEMENTSThis report is the fruit of collaboration among many individuals and institutions. The editorial and research team thanks allwho gave so generously of their expertise and energy, in particular:Sheridan Bartlett (City University of New York); Jean Christophe Fotso (APHRC); Nancy Guerra (University of California);Eva Jesperson (UNDP); JacobKumaresan (WHO Urban HEART); Gora Mboup (UN-Habitat); Sheela Patel (SDI);Mary Racelis (Ateneo de Manila University); Eliana Riggio; David Satterthwaite (IIED); Ita Sheehy (UNHCR);Nicola Shepherd (UNDESA); Mats Utas (Swedish Academy of Letters); and Malak Zaalouk (American University of Cairo),for serving on the External Advisory Board.Sheridan Bartlett; Roger Hart and Pamela Wridt (City University of New York); Carolyn Stephens (London School ofHygiene and Tropical Medicine and National University of Tucuman, Argentina); and Laura Tedesco (Universidad Autonomade Madrid), for authoring background papers.Fred Arnold (ICF Macro); Ricky Burdett (London School of Economics and Political Science); Elise Caves and Cristina Diez(ATD Fourth World Movement); Michael Cohen (New School); Malgorzata Danilczuk-Danilewicz; Celine d’Cruz (SDI);Robert Downs (Columbia University); SaraElder (ILO); Kimberly Gamble-Payne; Patrick Gerland (UNDESA); FriedrichHuebler (UNESCO); Richard Kollodge (UNFPA); MaristelaMonteiro (PAHO); Anushay Said (World Bank Institute);Helen Shaw (South East Public Health Observatory); MarkSommers (Tufts University); Tim Stonor (Space Syntax Ltd.);Emi Suzuki (World Bank); Laura Turquet (UN-Women); HenrikUrdal (Harvard Kennedy School); and Hania Zlotnik(UNDESA), for providing information and advice.Special thanks to Sheridan Bartlett, Gora Mboup and Amit Prasad (WHO) for their generosity of intellect and spirit.UNICEF country and regional offices and headquarters divisions contributed to this report by submitting findings andphotographs, taking part in formal reviews or commenting on drafts. Many field offices and UNICEF national committeesarranged to translate or adapt the report for local use.Programme, policy, communication and research advice and support were provided by Geeta Rao Gupta,Deputy ExecutiveDirector;Rima Salah,Deputy Executive Director;Gordon Alexander,Director,Office of Research; NicholasAlipui,Director,Programme Division; Louis-Georges Arsenault,Director,Office of Emergency Programmes; Colin Kirk,Director,Evaluation Office; Khaled Mansour,Director,Division of Communication; Richard Morgan,Director,Division of Policyand Practice; LisaAdelson-Bhalla; Christine De Agostini; Stephen Antonelli; Maritza Ascencios; LakshmiNarasimhan Balaji;GerritBeger; Wivina Belmonte; Rosangela Berman-Bieler; Aparna Bhasin; Nancy Binkin; Susan Bissell; ClarissaBrocklehurst;MarissaBuckanoff; Sally Burnheim; Jingqing Chai; Kerry Constabile; HowardDale; Tobias Dierks; KathrynDonovan;PaulEdwards; Solrun Engilbertsdottir; Rina Gill; Bjorn Gillsater; Dora Giusti; JudyGrayson; AttilaHancioglu;Peter Harvey; Saad Houry; Priscillia Kounkou Hoveyda; Robert Jenkins; Malene Jensen; TheresaKilbane; JimmyKolker;JuneKunugi; Boris De Luca; Susanne Mikhail Eldhagen; Sam Mort; Isabel Ortiz; Shannon O’Shea; Kent Page;NicholasRees; MariaRubi; Rhea Saab; Urmila Sarkar; Teghvir Singh Sethi; Fran Silverberg; Peter Smerdon; Antony Spalton;Manuela Stanculescu; David Stewart; Jordan Tamagni; Susu Thatun; Renee Van de Weerdt; and NataliaElenaWinder-Rossi.Special thanks to Catherine Langevin-Falcon,Chief,Publications Section, who oversaw the editing and production of thestatistical tables and provided essential expertise, guidance and continuity amid changes in personnel.Finally, a particular debt of gratitude is owed to David Anthony,Chief,Policy Advocacy, and editor of this report for the pastseveneditions, for his vision, support and encouragement.
REPORT TEAM
EDITORIAL AND RESEARCHAbid Aslam, Julia Szczuka,EditorsNikola Balvin, Sue Le-Ba, Meedan Mekonnen,Research officersChris Brazier,WriterMarc Chalamet,French editorCarlos Perellon,Spanish editorHirut Gebre-Egziabher,Lead,Yasmine Hage, Lisa Kenney,AnneYtreland, Jin Zhang,Research assistantsCharlotte Maitre,Lead,Anna Grojec,Carol Holmes,Copy editorsCeline Little, Dean Malabanan, Anne Santiago,Judith Yemane,Editorial and administrative supportPRODUCTION AND DISTRIBUTIONJaclyn Tierney,Chief,Print and Translation Section;Germain Ake; Fanuel Endalew; JorgePeralta-Rodriguez;Elias Salem; Nogel S. Viyar; Edward Ying Jr.
EM28BAFebr RGua Ory ED2012
STATISTICAL TABLESTessa Wardlaw,Associate Director,Statistics andMonitoring Section, Division of Policy and Practice;PriscillaAkwara; David Brown; Danielle Burke;XiaodongCai; ClaudiaCappa; Liliana Carvajal; ArchanaDwivedi; AnneGenereux; ElizabethHorn-Phatanothai;ClaesJohansson; RouslanKarimov; Mengjia Liang;RolfLuyendijk; NyeinNyeinLwin; Colleen Murray;HollyNewby; KhinWityeeOo; Nicole Petrowski;ChihoSuzuki; Danzhen YouONLINE PRODUCTION AND IMAGESStephen Cassidy,Chief,Internet, Broadcast andImage Section; Matthew Cortellesi; Susan Markisz;KeithMusselman; Ellen Tolmie; Tanya TurkovichDesign by Green Communication Design inc.Printed by Brodock Press, Inc.
Acknowledgements
iii
ACTION
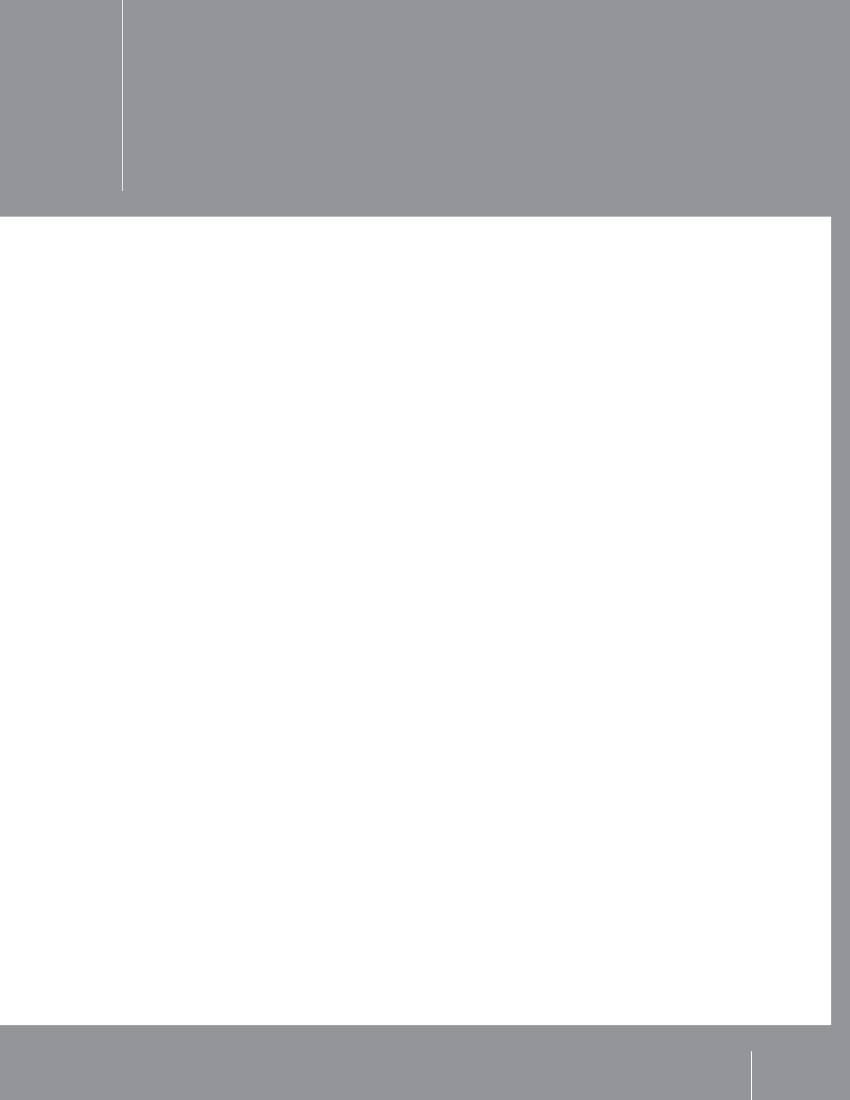
PUTTING CHILDREN FIRST IN AN URBAN WORLDThe experience of childhood is increasingly urban. Over half the world’s people – including more than abillion children – now live in cities and towns. Many children enjoy the advantages of urban life, includingaccess to educational, medical and recreational facilities. Too many, however, are denied such essentials aselectricity, clean water and health care – even though they may live close to these services. Too many areforced into dangerous and exploitative work instead of being able to attend school. And too many face aconstant threat of eviction, even though they live under the most challenging conditions – in ramshackledwellings and overcrowded settlements that are acutely vulnerable to disease and disaster.The hardships endured by children in poor communities are often concealed – and thus perpetuated – by thestatistical averages on which decisions about resource allocation are based. Because averages lump every-one together, the poverty of some is obscured by the wealth of others. One consequence of this is thatchildren already deprived remain excluded from essential services.Increasing numbers of children are growing up in urban areas. They must be afforded the amenities andopportunities they need to realize their rights and potential. Urgent action must be taken to:• Better understand the scale and nature of poverty and exclusion affecting children in urban areas.• Identify and remove the barriers to inclusion.
• Ensure that urban planning, infrastructure development, service delivery and broader efforts to reduce poverty and inequality meet the particular needs and priorities of children.• Promote partnership between all levels of government and the urban poor – especially children and young people.• Pool the resources and energies of international, national, municipal and community actors in support of efforts to ensure that marginalized and impoverished children enjoy their full rights.These actions are not goals but means to an end: fairer, more nurturing cities and societies for all people –starting with children.
iv
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
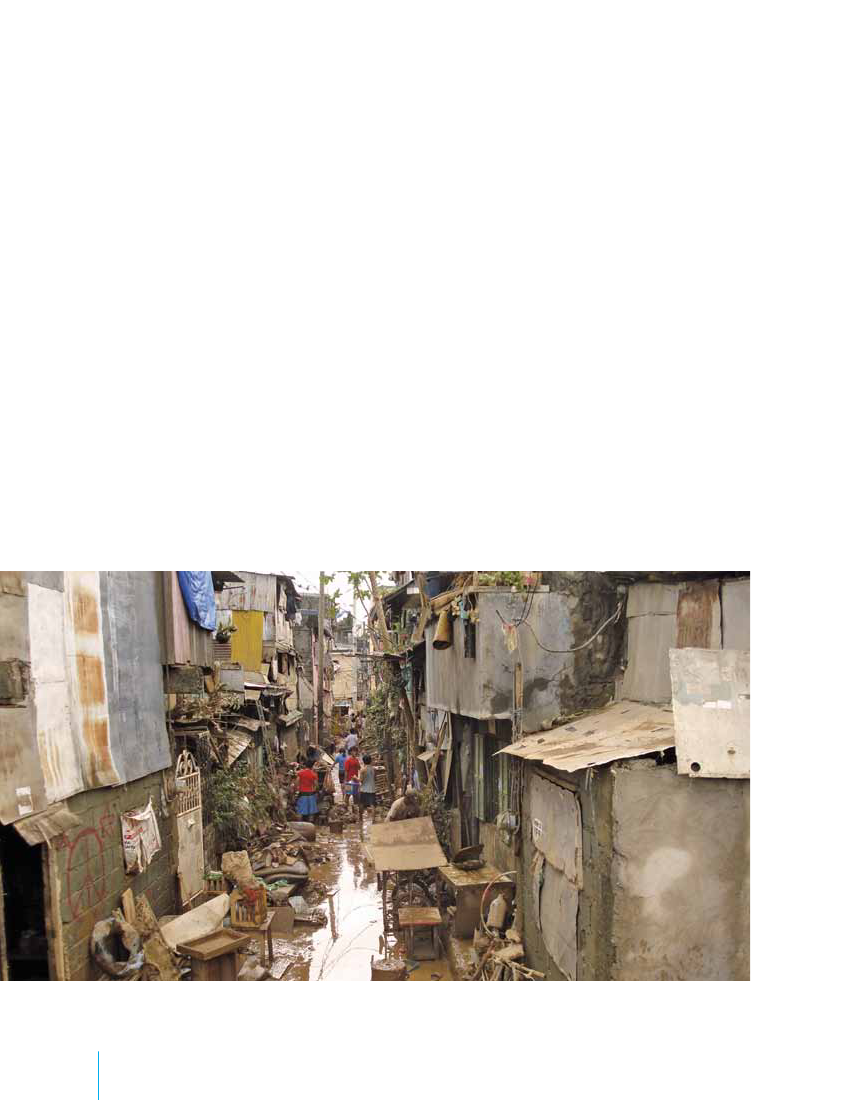
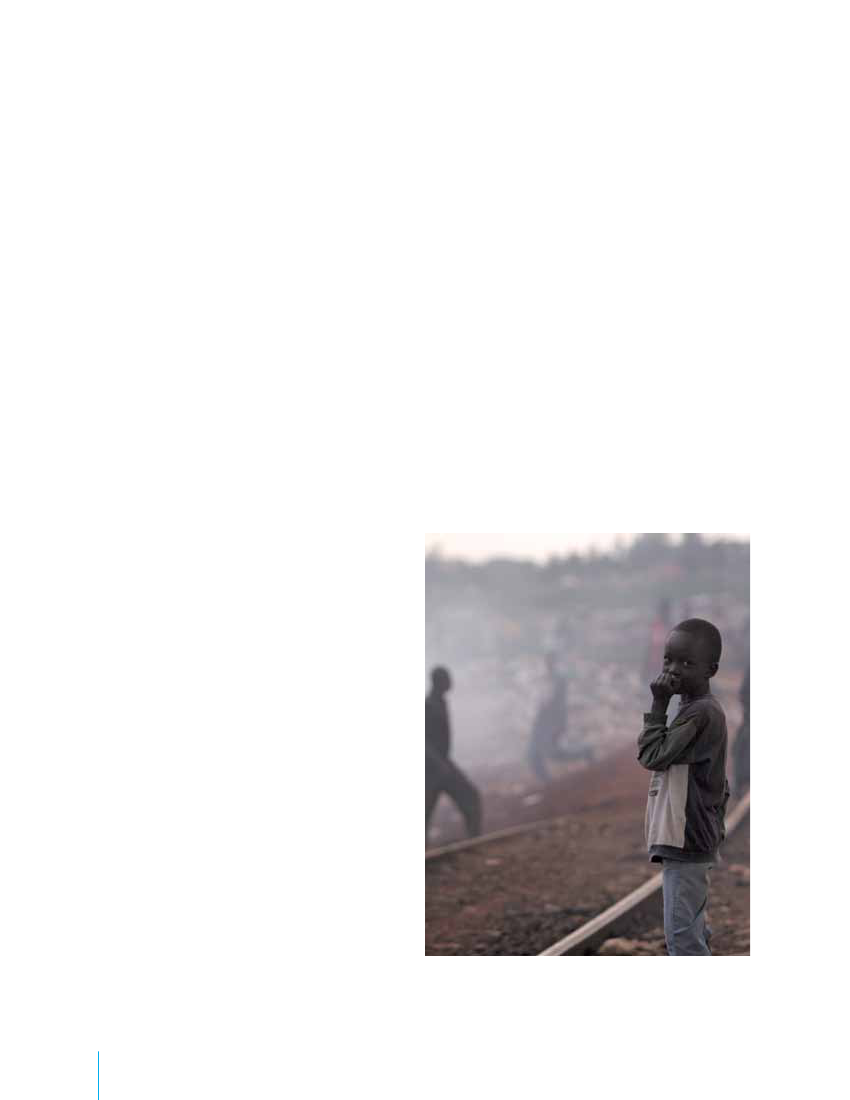
FOREWORDWhen many of us think of the world’s poorest children, the image that comes readily to mind is that of achild going hungry in a remote rural community in sub-Saharan Africa – as so many are today.But asThe State of the World’s Children 2012shows with clarity and urgency, millions of children in citiesand towns all over the world are also at risk of being left behind.In fact, hundreds of millions of children today live in urban slums, many without access to basic services.They are vulnerable to dangers ranging from violence and exploitation to the injuries, illnesses and deaththat result from living in crowded settlements atop hazardous rubbish dumps or alongside railroad tracks.And their situations – and needs – are often represented by aggregate figures that show urban children to bebetter off than their rural counterparts, obscuring the disparities that exist among the children of the cities.This report adds to the growing body of evidence and analysis, from UNICEF and our partners, that scar-city and dispossession afflict the poorest and most marginalized children and families disproportionately.It shows that this is so in urban centres just as in the remote rural places we commonly associate withdeprivation and vulnerability.The data are startling. By 2050, 70 per cent of all people will live in urban areas. Already, 1 in 3 urbandwellers lives in slum conditions; in Africa, the proportion is a staggering 6 in 10. The impact on childrenliving in such conditions is significant. From Ghana and Kenya to Bangladesh and India, children livingin slums are among the least likely to attend school. And disparities in nutrition separating rich and poorchildren within the cities and towns of sub-Saharan Africa are often greater than those between urban andrural children.Every disadvantaged child bears witness to a moral offense: the failure to secure her or his rights to survive,thrive and participate in society. And every excluded child represents a missed opportunity – because when soci-ety fails to extend to urban children the services and protection that would enable them to develop as productiveand creative individuals, it loses the social, cultural and economic contributions they could have made.We must do more to reach all children in need, wherever they live, wherever they are excluded and leftbehind. Some might ask whether we can afford to do this, especially at a time of austerity in nationalbudgets and reduced aid allocations. But if we overcome the barriers that have kept these children fromthe services that they need and that are theirs by right, then millions more will grow up healthy, attendschool and live more productive lives.Can we afford not to do this?Anthony LakeExecutive Director, UNICEFForewordv
EM28BAFebr RGua Ory ED2012
AN URBAN WORLDThis graphic depicts countries and territories with urbanpopulations exceeding 100,000. Circles are scaled inproportion to urban population size. Where space allows,numbers within circles show urban population (in millions)and urban percentage of the country’spopulation.NorwaySweden7.9FinlandEstoniaIcelandNetherlands13.883%Belgium10.497%
Denmark
LatviaLithuania
Canada27.481%
Ireland
UnitedKingdom49.480%
Germany60.874%
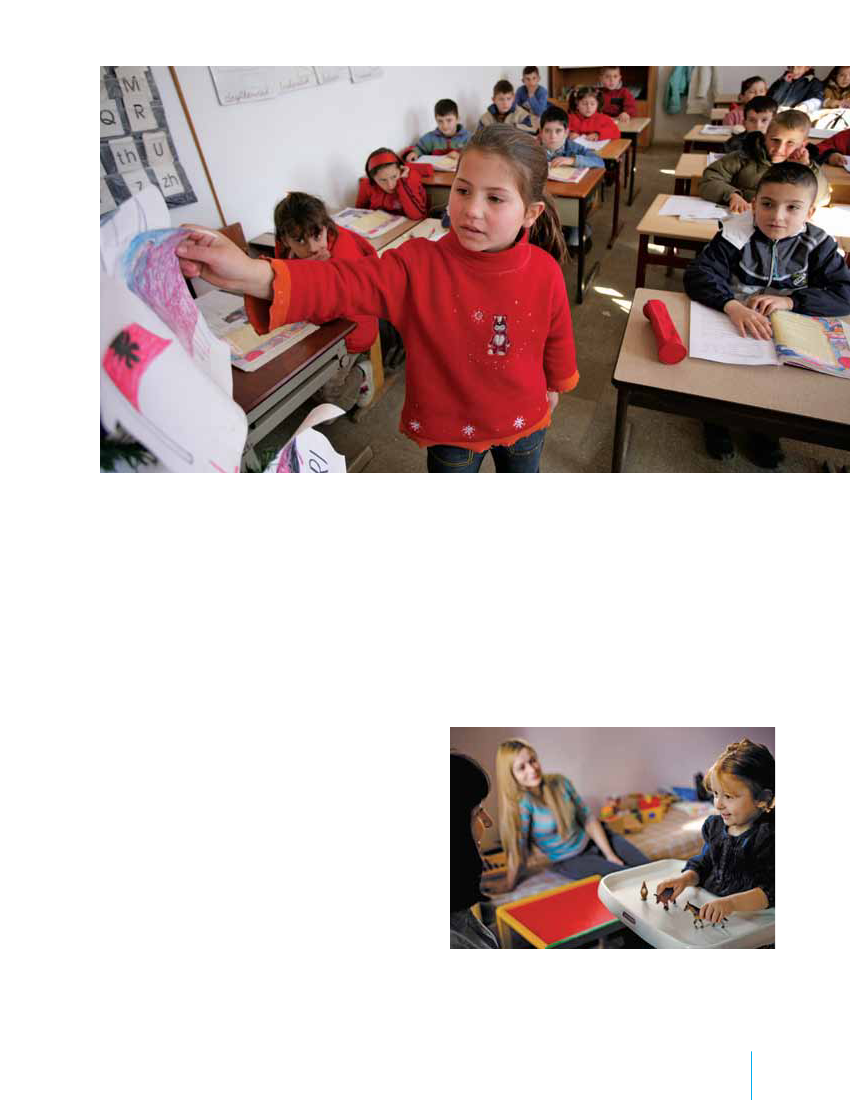
Poland23.361%CzechRepublicSlovakia7.7
Belarus7.2
EM28BAFebr RGua Ory ED2012Spain35.777%Italy41.468%AlbaniaMaltaPortugalBahamas
United Statesof America255.482%Mexico88.378%Cuba8.5
France53.585%
Luxembourg
Ukraine31.369%
AustriaHungaryRomania Republic ofSwitzerlandMoldova12.3Slovenia57%Croatia SerbiaBulgariaBosnia andHerzegovina The formerYugoslavMontenegroRepublic ofMacedonia
GreeceCyprus
Turkey50.770%LebanonSyrian ArabRepublic11.456%Jordan
GeorgiaAzerbaijanArmenia
Morocco18.658%
Algeria23.666%
Tunisia7.1
OccupiedPalestinian Territory
Iraq21.066%Kuwait
Libya
Mauritania
Niger
Chad
Egypt35.243%Sudan17.540%
Israel
Guatemala BelizeHaiti Dominican7.1RepublicHondurasJamaicaEl SalvadorNicaraguaCosta RicaPanama
Cape Verde
Senegal
Mali
Saudi ArabiaUnited Arab22.5Emirates82%EritreaYemen Oman7.6
BahrainQatar
Gambia
Guinea-Bissau
BurkinaFasoGhana12.651%
Nigeria78.950%
Colombia34.875%Ecuador9.7
Venezuela(BolivarianRepublic of)27.193%
BarbadosTrinidad and TobagoGuyanaSuriname
Guinea
Sierra Leone
CôteLiberia d’Ivoire10.051%
CentralAfricanRepublic
DjiboutiEthiopiaSomalia13.817%Kenya9.0
Togo Benin
Cameroon11.458%
UgandaRwanda
Peru22.477%
Bolivia(PlurinationalState of)Paraguay
Brazil168.787%
Equatorial GuineaGabonSao Tome and Principe
Burundi
United Republicof TanzaniaDemocraticCongo11.8Republic26%of the Congo23.235%MalawiComoros
Angola11.259%BotswanaNamibia
MauritiusMozambiqueZambia9.0MadagascarZimbabweSwaziland
Chile15.289%
Uruguay
SouthAfrica30.962%
Lesotho
Argentina37.392%
Source:United Nations, Department of Economic and Social Affairs (UNDESA), Population Division special updated estimates of urban population as of October 2011, consistent withWorld Population Prospects: The 2010 revisionandWorld Urbanization Prospects: The 2009 revision.Graphic presentation of data based onThe Guardian,27 July 2007.This map is stylized and based on an approximate scale. It does not reflect a position by UNICEF on the legal status of any country or territory or the delimitation of any frontiers.
vi
THE STATE OF THE WORLD’S CHILDREN 2012
Above 75% urbanBetween 50% and 75% urbanBetween 25% and 50% urbanMongolia
RussianFederation104.673%
Below 25% urban
ChinaUrban population in millions
Kazakhstan9.4
629.847%
KyrgyzstanUzbekistan10.036%TajikistanTurkmenistan
Democratic People’sRepublic of Korea14.760%
Afghanistan7.1
Iran(IslamicRepublic of)52.371%
Pakistan62.336%
India367.530%Maldives
EM28BAFebr RGua Ory ED2012Percentage urbanNepalBhutan
Republicof Korea40.083%
Japan84.6
Canton67%14.5
Bangladesh41.728%
Lao People’sDemocraticRepublicMyanmar16.134%
Viet Nam26.730%
Thailand23.534%
Cambodia
Philippines45.649%
Malaysia20.572%
Brunei Darussalam
Sri Lanka
Singapore
Timor-Leste
Indonesia106.244%
Papua New GuineaSolomon Islands
Australia19.889%New Zealand
Fiji
Notes:Because of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011,data for the Sudan and South Sudan as separate States are not yet available. Data presented are for the Sudan pre-cession.Data for China do not include Hong Kong and Macao, Special Administrative Regions of China. Hong Kong became a Special Administrative Region (SAR) of China as of 1 July 1997;Macao became a SAR of China as of 20 December 1999.Data for France do not include French Guiana, Guadeloupe, Martinique, Mayotte and Reunion.Data for the Netherlands do not include the Netherlands Antilles.Data for the United States of America do not include Puerto Rico and United States Virgin Islands.
An urban world
vii
CONTENTSACkNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iiiACTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ivFOREWORDAnthony Lake, Executive Director, UNICEF . . . . . . . . . . . . . . .vCHAPTER 1Children in an increasingly urban world . . . . . . . . . . . . . . . . .1An urban future . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2Poverty and exclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Meeting the challenges of an urban future . . . . . . . . . . . . . . .8CHAPTER 2Children’s rights in urban settings . . . . . . . . . . . . . . . . . . . . .13An environment for fulfilling children’s rights . . . . . . . . . . .14CHAPTER 4Towards cities fit for children . . . . . . . . . . . . . . . . . . . . . . . . .49Policy and collaboration . . . . . . . . . . . . . . . . . . . . . . . . . . . . .49Participatory urban planning and management . . . . . . . . . .50Child-Friendly Cities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .55Non-discrimination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .55Nutrition and hunger . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .55Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .57HIV and AIDS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .57Water, sanitation and hygiene . . . . . . . . . . . . . . . . . . . . . . . .58Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .58Child protection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .60Housing and infrastructure . . . . . . . . . . . . . . . . . . . . . . . . . . .60Urban planning for children’s safety . . . . . . . . . . . . . . . . . . .61Safe cities for girls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .61Safe spaces for play . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .62Social capital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .62Cultural inclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .62Culture and arts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .63Technology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .63CHAPTER 5Uniting for children in an urban world . . . . . . . . . . . . . . . . .67Understand urban poverty and exclusion . . . . . . . . . . . . . . .68Remove the barriers to inclusion . . . . . . . . . . . . . . . . . . . . . .70Put children first . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .73Promote partnership with the urban poor . . . . . . . . . . . . . . 74Work together to achieve results for children . . . . . . . . . . . . 74Towards fairer cities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .75
Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14Child survival . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14Immunization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Maternal and newborn health . . . . . . . . . . . . . . . . . . . . . . . .18Breastfeeding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18Nutrition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19Respiratory illness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22Road traffic injuries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22HIV and AIDS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22Mental health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24Water, sanitation and hygiene . . . . . . . . . . . . . . . . . . . . . . . .25Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28Early childhood development . . . . . . . . . . . . . . . . . . . . . . . . .28Primary education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29Protection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31Child trafficking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31Child labour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32Children living and working on the streets . . . . . . . . . . . . . .32CHAPTER 3Urban challenges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .35Migrant children . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .35Economic shocks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .40Violence and crime . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .42Disaster risk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .45
viii
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012PANELS
Social determinants of urban health . . . . . . . . . . . . . . . . . . . .4Slums: The five deprivations . . . . . . . . . . . . . . . . . . . . . . . . . . .5Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10The Convention on the Rights of the Child . . . . . . . . . . . . . .16The Millennium Development Goals . . . . . . . . . . . . . . . . . . .33Agents, not victims . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38Armed conflict and children in urban areas . . . . . . . . . . . . .42
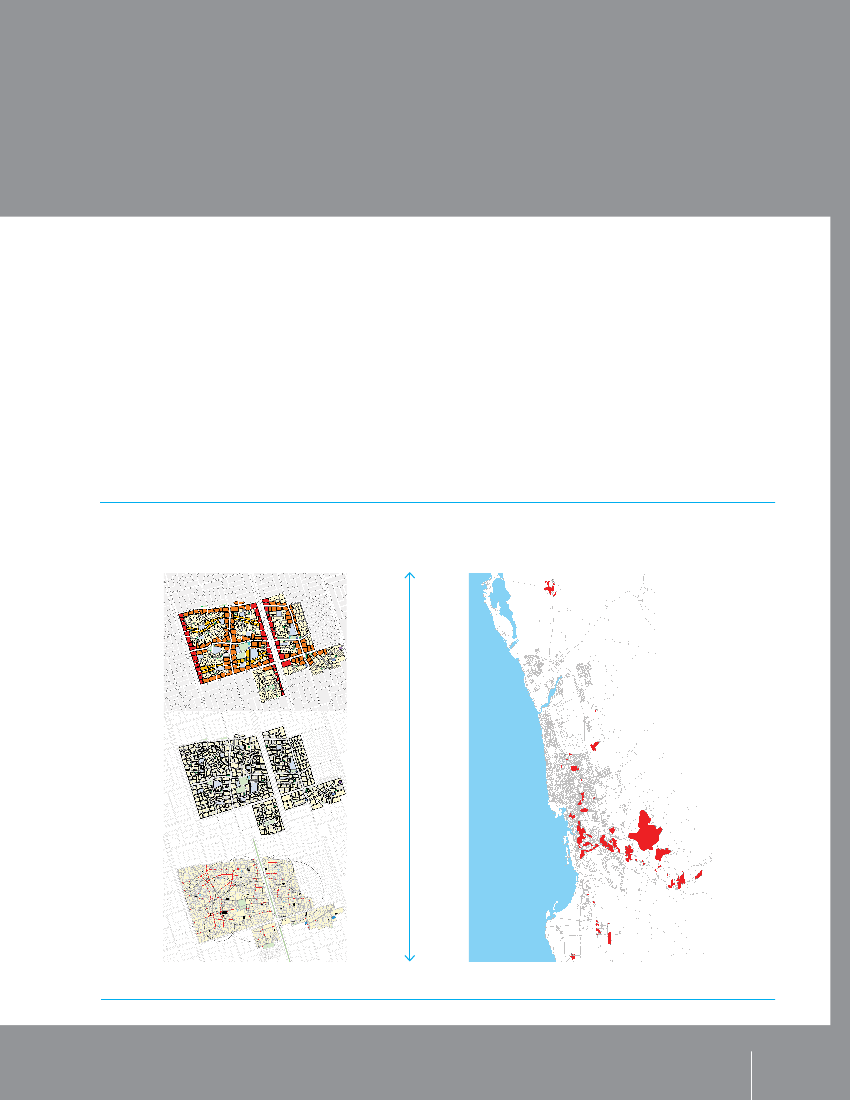
FOCUS ONUrban disparities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6Maternal and child health services for the urban poor:A case study from Nairobi, kenya . . . . . . . . . . . . . . . . . . . . .20Mapping urban disparities to secure child rights . . . . . . . . .26Helpful strategies in urban emergencies . . . . . . . . . . . . . . . .39Women, children, disaster and resilience . . . . . . . . . . . . . . .41Urban HEART: Measuring andresponding to health inequity . . . . . . . . . . . . . . . . . . . . . . . .52The Child-Friendly Cities Initiative:Fifteen years of trailblazing work . . . . . . . . . . . . . . . . . . . . . .56Upgrading informal settlements in Jeddah . . . . . . . . . . . . .64The paucity of intra-urban data . . . . . . . . . . . . . . . . . . . . . . .69PERSPECTIVE
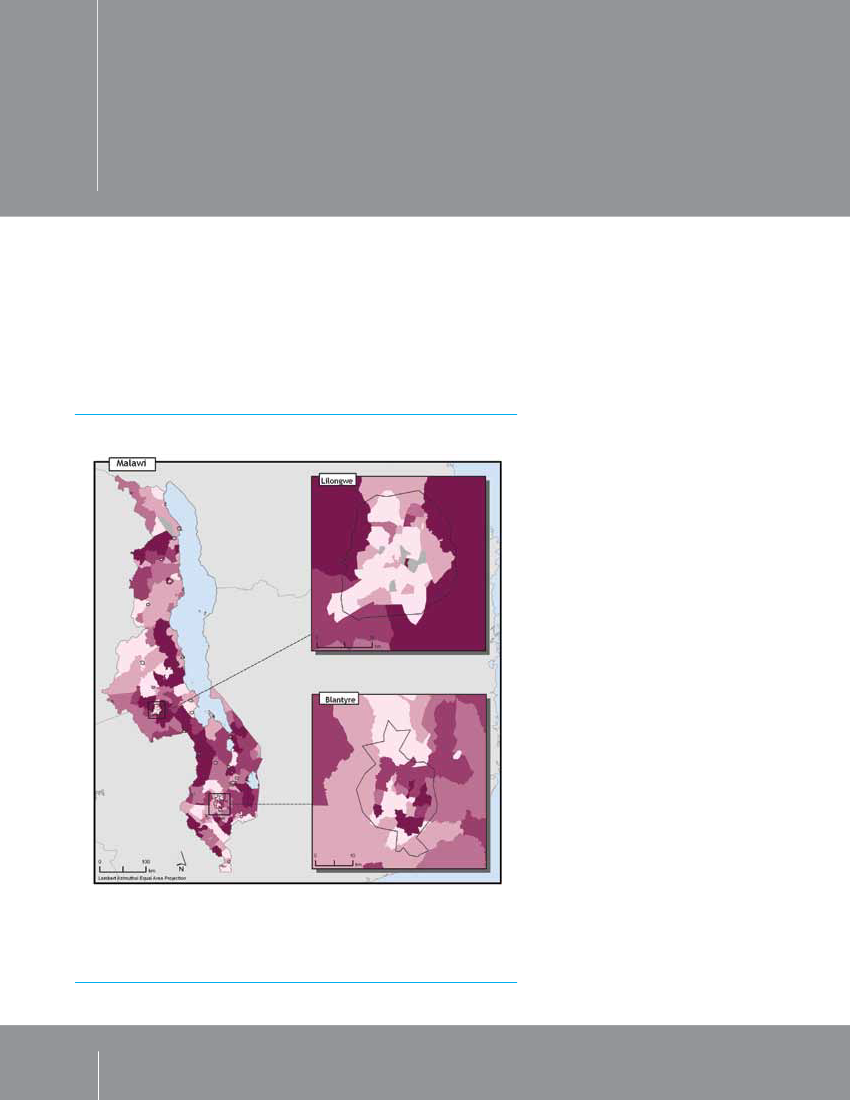
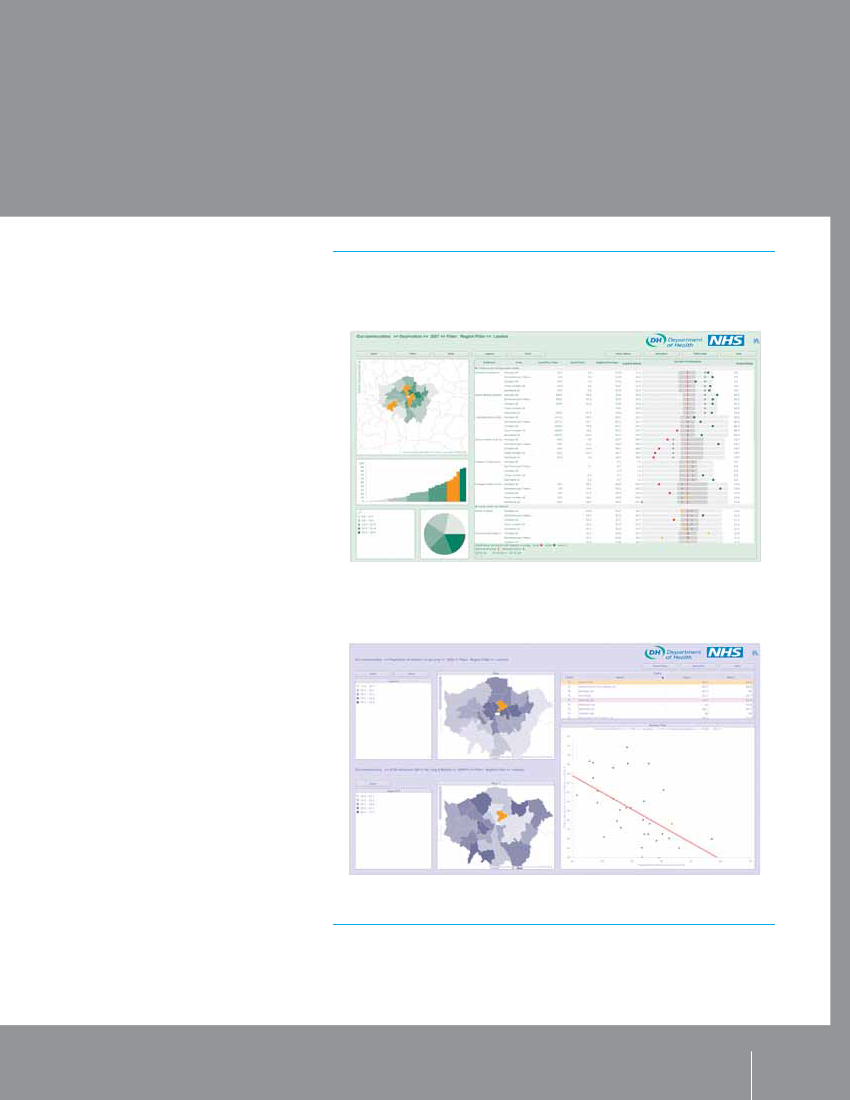
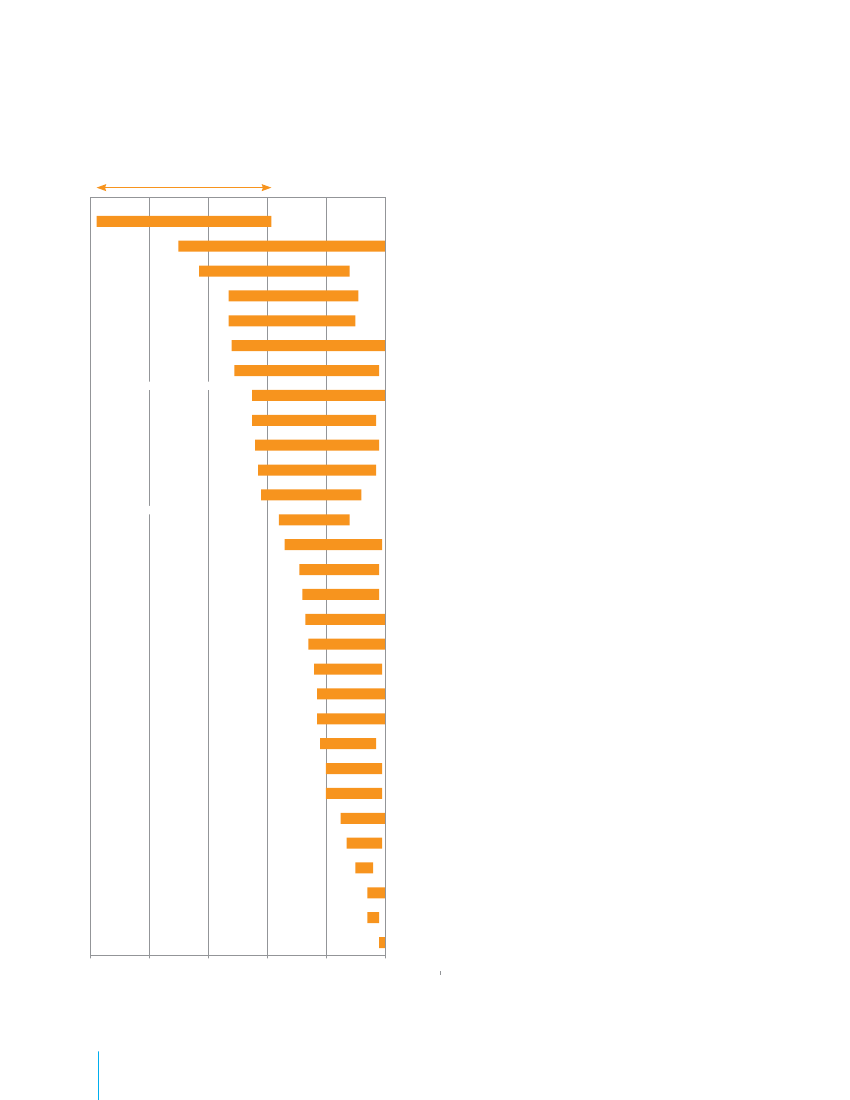
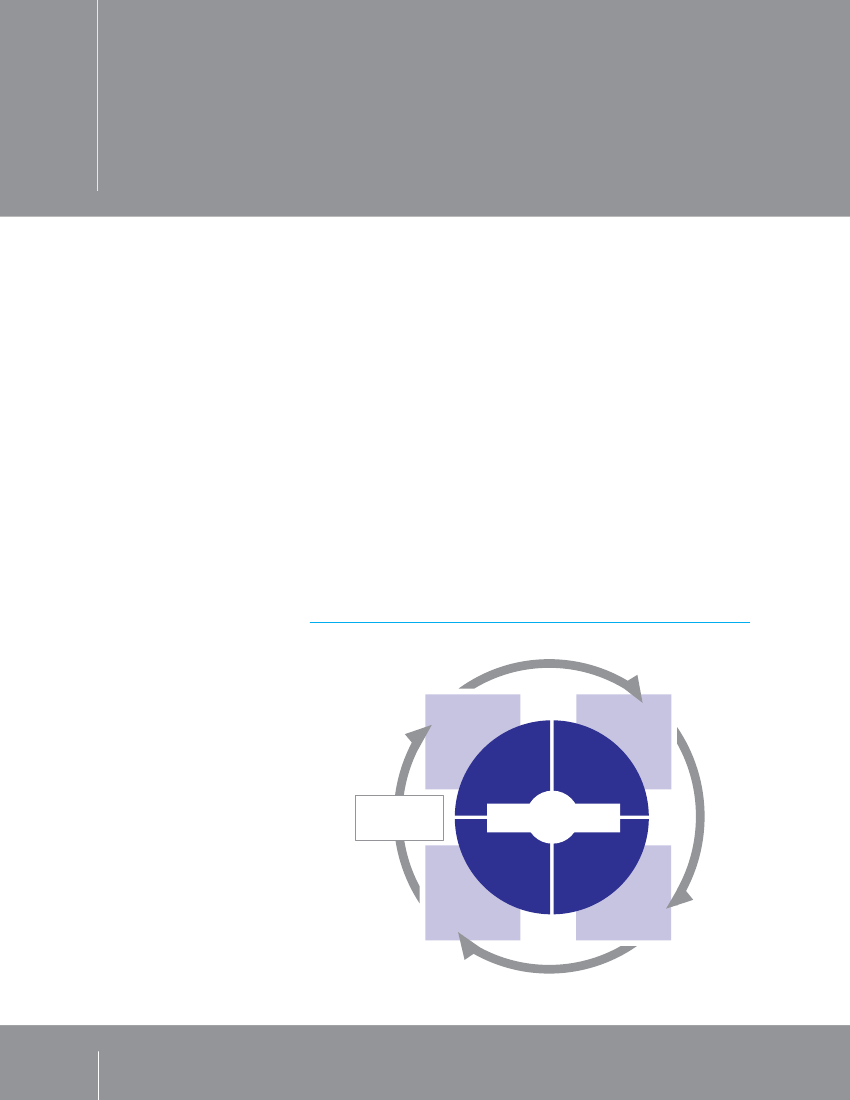
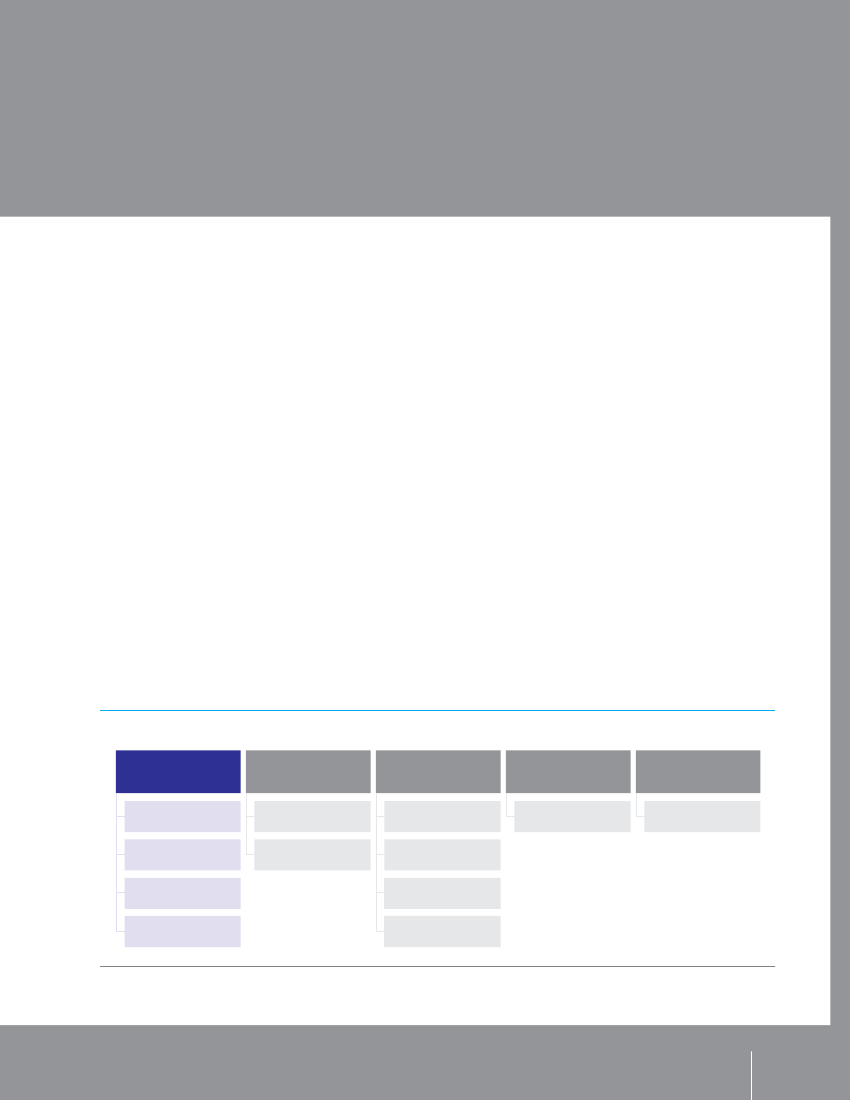
1 .5 Half of the world’s urban population lives in citiesof fewer than 500,000 inhabitants . . . . . . . . . . . . . . . . . 112 .1 Wealth increases the odds of survival for childrenunder the age of 5 in urban areas . . . . . . . . . . . . . . . . . .182 .2 Children of the urban poor are more likelyto be undernourished . . . . . . . . . . . . . . . . . . . . . . . . . . . .192 .3 Stunting prevalence among children under3 years old in urban kenya . . . . . . . . . . . . . . . . . . . . . . . .212 .4 HIV is more common in urban areas andmore prevalent among females . . . . . . . . . . . . . . . . . . . .222 .5 In urban areas, access to improvedwater and sanitation is not keeping pacewith population growth . . . . . . . . . . . . . . . . . . . . . . . . . .242 .6 Mapping poverty in Lilongwe and Blantyre, Malawi . . .262 .7 Tracking health outcomesin London, United kingdom . . . . . . . . . . . . . . . . . . . . . . .272 .8 Urban income disparities also mean unequalaccess to water . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .282 .9 School attendance is lower in slums . . . . . . . . . . . . . . .304 .1 Urban HEART planning and implementation cycle . . . .524 .2 Twelve core indicators . . . . . . . . . . . . . . . . . . . . . . . . . . .534 .3 Design scenarios for an informal settlement . . . . . . . . .65REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .76STATISTICAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .81
Her Majesty Queen Rania Al Abdullah of JordanOut of sight, out of reach . . . . . . . . . . . . . . . . . . . . . . . . . . . .15Amitabh BachchanReaching every child: Wiping out polio in Mumbai . . . . . . .23Eugen CraiA world apart: The isolation of Roma children . . . . . . . . . . .37ATD Fourth World Movement Youth Group, New York CitySpeaking for ourselves . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .43Tuiloma Neroni SladePacific challenges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .46José Clodoveu de Arruda Coelho NetoBuilding children’s lives to build a city . . . . . . . . . . . . . . . . . .51Ricky MartinTrafficked children in our cities:Protecting the exploited in the Americas . . . . . . . . . . . . . . . .54Celine d’Cruz and Sheela PatelHome-grown solutions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .72FIGURES
An urban world . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vi1 .1 Almost half of the world’s children live in urban areas . . . .21 .2 Urban population growth is greater in lessdeveloped regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31 .3 Educational attainment can be mostunequal in urban areas . . . . . . . . . . . . . . . . . . . . . . . . . . . .61 .4 Urban populations are growing fastest inAsia and Africa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
EM28BAFebr RGua Ory ED2012Table 7 .
Under-five mortality rankings . . . . . . . . . . . . . . . . . . . . . . . . .87Table 1 . Basic indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . .88Table 2 . Nutrition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .92Table 3 . Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .96Table 4 . HIV/AIDS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100Table 5 . Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104Table 6 . Demographic indicators . . . . . . . . . . . . . . . . . . . . 108Economic indicators . . . . . . . . . . . . . . . . . . . . . . . 112Table 8 . Women . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 116Table 9 . Child protection . . . . . . . . . . . . . . . . . . . . . . . . . . .120Table 10 . The rate of progress . . . . . . . . . . . . . . . . . . . . . . .125Table 11 . Adolescents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .130Table 12 . Equity – Residence . . . . . . . . . . . . . . . . . . . . . . . .134Table 13 . Equity – Household wealth . . . . . . . . . . . . . . . . . .138ABBREVIATIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .142
Contents
ix
CHAPTER
1
EM28BAFebr RGua Ory ED2012� UNICEF/NYHQ2005-1185/Roger LeMoyne
The day is coming when the majority of the world’schildren will grow up in cities and towns. Already, halfof all people live in urban areas. By mid-century, overtwo thirds of the global population will call these placeshome. This report focuses on the children – more thanone billion and counting – who live in urban settingsaround the world.
Urban areas offer great potential to secure children’srights and accelerate progress towards the MillenniumDevelopment Goals (MDGs). Cities attract and gener-ate wealth, jobs and investment, and are thereforeassociated with economic development. The moreurban a country, the more likely it is to have higherincomes and stronger institutions.1Children in urbanareas are often better off than their rural counter-parts thanks to higher standards of health, protection,education and sanitation. But urban advances have
EM28BAFebr RGua Ory ED2012
Children inan increasinglyurban worldbeen uneven, and millions of children in marginalizedurban settings confront daily challenges and depriva-tions of their rights.Traditionally, when children’s well-being is assessed, acomparison is drawn between the indicators for chil-dren in rural areas and those in urban settings. Asexpected, urban results tend to be better, whether interms of the proportion of children reaching their firstor fifth birthday, going to school or gaining access toimproved sanitation. But these comparisons rest onaggregate figures in which the hardships endured bypoorer urban children are obscured by the wealth ofcommunities elsewhere in the city.Where detailed urban data are available, they revealwide disparities in children’s rates of survival, nutritionalstatus and education resulting from unequal access to
Children in an increasingly urban world
1
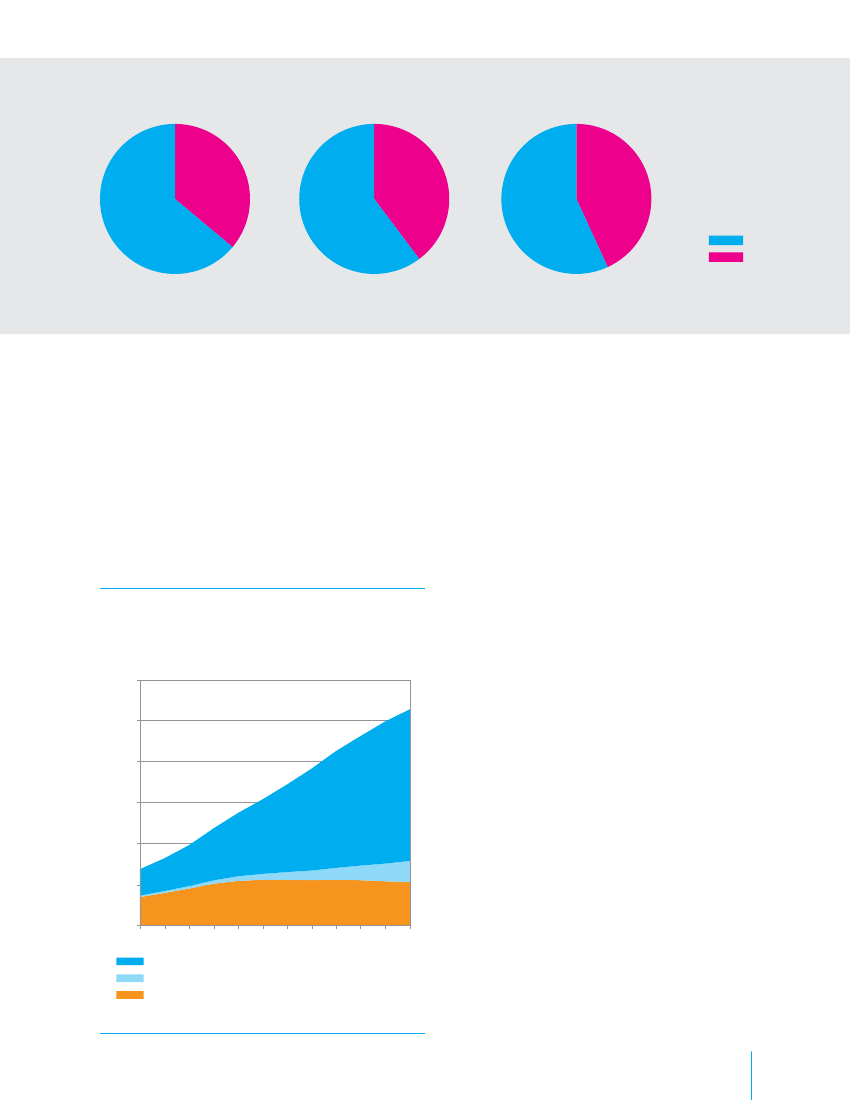
Figure 1 .1 . Almost half of the world’s children live in urban areasWorld population (0–19 years old)
27%
30%
33%
1955
1965
1975
This report focuses mainly on those children in urbansettings all over the world who face a particularlycomplex set of challenges to their development and thefulfilment of their rights. Following an overview of theworld’s urban landscape, Chapter 2 looks at the statusof children in urban settings through the lens of inter-national human rights instruments and developmentgoals. Chapter 3 examines some of the phenomenashaping the lives of children in urban areas, from theirreasons for coming to the city and their experience ofmigration to the challenges posed by economic shocks,violence and acute disaster risk.Clearly, urban life can be harsh. It need not be. Manycities have been able to contain or banish diseases thatwere widespread only a generation ago. Chapter 4 pre-sents examples of efforts to improve the urban realities2THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012An urban future
services. Such disaggregated information is hard to find,however, and for the most part development is pursued,and resources allocated, on the basis of statistical aver-ages. One consequence of this is that children livingin informal settlements and impoverished neighbour-hoods are excluded from essential services and socialprotection to which they have a right. This is happen-ing as population growth puts existing infrastructureand services under strain and urbanization becomesnearly synonymous with slum formation. Accordingto the United Nations Human Settlements Programme(UN-Habitat), one city dweller in three lives in slumconditions, lacking security of tenure in overcrowded,unhygienic places characterized by unemployment,pollution, traffic, crime, a high cost of living, poorservice coverage and competition over resources.
that children confront. These instances show that it ispossible to fulfil commitments to children – but onlyif all children receive due attention and investmentand if the privilege of some is not allowed to obscurethe disadvantages of others. Accordingly, the finalchapter of this report identifies broad policy actions thatshould be included in any strategy to reach excluded chil-dren and foster equity in urban settings riven by disparity.
By 2050, 7 in 10 people will live in urban areas. Everyyear, the world’s urban population increases by approx-imately 60 million people. Most of this growth istaking place in low- and middle-income countries. Asiais home to half of the world’s urban population and66 out of the 100 fastest-growing urban areas, 33 ofwhich are in China alone. Cities such as Shenzhen, with a10 per cent rate of annual increase in 2008, are doublingin population every seven years.2Despite a low overallrate of urbanization, Africa has a larger urban populationthan North America or Western Europe, and more than6 in 10 Africans who live in urban areas reside in slums.New urban forms are evolving as cities expand andmerge. Nearly 10 per cent of the urban population isfound in megacities – each with more than 10 millionpeople – which have multiplied across the globe.New York and Tokyo, on the list since 1950, havebeen joined by a further 19, all but 3 of them in Asia,Latin America and Africa. Yet most urban growth istaking place not in megacities but in smaller cities andtowns, home to the majority of urban children andyoung people.3
36%
40%
43%RuralUrban
1985
1995
2005Source:United Nations, Department of Economic and Social Affairs (UNDESA), Population Division.
Migration from the countryside has long driven urbangrowth and remains a major factor in some regions.But the last comprehensive estimate, made in 1998,
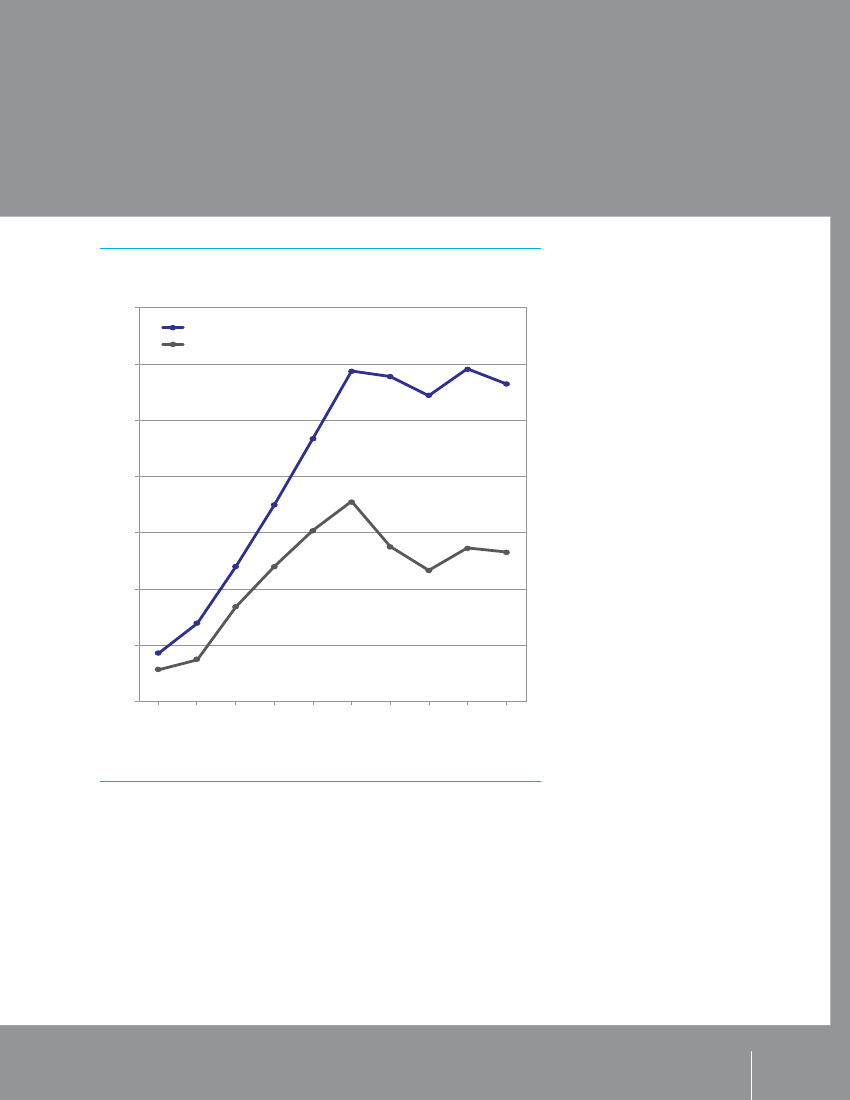
Figure 1 .2 . Urban population growth is greater inless developed regionsWorld urban population (0–19 years old)Millions1,200
1,000
800
600
400
200
0195019551960196519701975198019851990199520002005
Less developed regionsLeast developed countries (a subset of less developed regions)More developed regionsSource:UNDESA, Population Division.
EM28BAFebr RGua Ory ED2012
In contrast to rapid urban growth in the developingworld, more than half of Europe’s cities are expectedto shrink over the next two decades.4The size of theurban population in high-income countries is projectedto remain largely unchanged through 2025, however,with international migrants making up the balance.5
suggests that children born into existing urban popula-tions account for around 60 per cent of urban growth.6
Poverty and exclusionFor billions of people, the urban experience is oneof poverty and exclusion. Yet standard data collec-tion and analysis fail to capture the full extent of bothproblems. Often, studies overlook those residents of acity whose homes and work are unofficial or unreg-istered – precisely those most likely to be poor orsuffer discrimination. Moreover, official definitions ofpoverty seldom take sufficient account of the cost ofnon-food needs. In consequence, poverty thresholdsapplied to urban populations make inadequate allow-ance for the costs of transport, rent, water, sanitation,schooling and health services.7Difficult urban living conditions reflect and are exac-erbated by factors such as illegality, limited voice indecision-making and lack of secure tenure, assetsand legal protection. Exclusion is often reinforced bydiscrimination on the grounds of gender, ethnicity, raceor disability. In addition, cities often expand beyondthe capacity of the authorities to provide the infrastruc-ture and services needed to ensure people’s health andwell-being. A significant proportion of urban popula-tion growth is occurring in the most unplanned anddeprived areas. These factors combine to push essen-tial services beyond the reach of children and familiesliving in poor urban neighbourhoods.Physical proximity to a service does not guaranteeaccess. Indeed, many urban inhabitants live close toChildren in an increasingly urban world3
schools or hospitals but have little chance of using theseservices. Even where guards or fees do not bar entry, poorpeople may lack the sense of entitlement and empower-ment needed to ask for services from institutions perceivedas the domain of those of higher social or economic rank.Inadequate access to safe drinking water and sanita-tion services puts children at increased risk of illness,undernutrition and death. When child health statis-tics are disaggregated, it becomes clear that evenwhere services are nearby, children growing up inpoor urban settings face significant health risks. Insome cases, the risks exceed those prevalent in ruralareas.8Studies demonstrate that in many countries,children living in urban poverty fare as badly as or
worse than children living in rural poverty in terms ofheight-for-weight and under-five mortality.9Children’s health is primarily determined by the socio-economic conditions in which they are born, grow andlive, and these are in turn shaped by the distributionof power and resources. The consequences of havingtoo little of both are most readily evident in infor-mal settlements and slums, where roughly 1.4 billionpeople will live by 2020.10By no means do all of the urban poor live in slums –and by no means is every inhabitant of a slum poor.Nevertheless, slums are an expression of, and a practi-cal response to, deprivation and exclusion.
Social determinants of urban healthStark disparities in health between rich and poor havedrawn attention to the social determinants of health, orthe ways in which people’s health is affected not onlyby the medical care and support systems available toprevent and manage illness, but also by the economic,social and political circumstances in which they are bornand live.
The urban environment is in itself a social determinantof health. Urbanization drove the emergence of publichealth as a discipline because the concentration ofpeople in towns and cities made it easier for communicablediseases to spread – mainly from poorer quarters to wealth-ier ones. An increasingly urban world is also contributing tothe rising incidence of non-communicable diseases, obesity,alcohol and substance abuse, mental illness and injuries.Many poor and marginalized groups live in slums andinformal settlements, where they are subjected to amultitude of health threats. Children from these commu-nities are particularly vulnerable because of the stressesof their living conditions. As the prevalence of physicaland social settings of extreme deprivation increases, sodoes the risk of reversing the overall success of diseaseprevention and control efforts.The urban environment need not harm people’s health.In addition to changes in individual behaviour, broader
Source:World Health Organization; Global Research Network on Urban Health Equity.
4
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
social policy prioritizing adequate housing; water andsanitation; food security; efficient waste managementsystems; and safer places to live, work and play caneffectively reduce health risk factors. Good governancethat enables families from all urban strata to accesshigh-quality services – education, health, public trans-portation and childcare, for example – can play a majorpart in safeguarding the health of children in urbanenvironments.Growing awareness of the potential of societalcircumstances to help or harm individuals’ health hasled to such initiatives as the World Health Organization’sCommission on Social Determinants of Health. Its recom-mendations emphasize that effectively addressing thecauses of poor health in urban areas requires a rangeof solutions, from improving living conditions, throughinvestment in health systems and progressive taxation, toimproved governance, planning and accountability at thelocal, national and international levels. The challengesare greatest in low- and middle-income countries, whererapid urban population growth is seldom accompanied byadequate investment in infrastructure and services. TheCommission has also highlighted the need to address theinequalities that deny power and resources to margin-alized populations, including women, indigenous peopleand ethnic minorities.
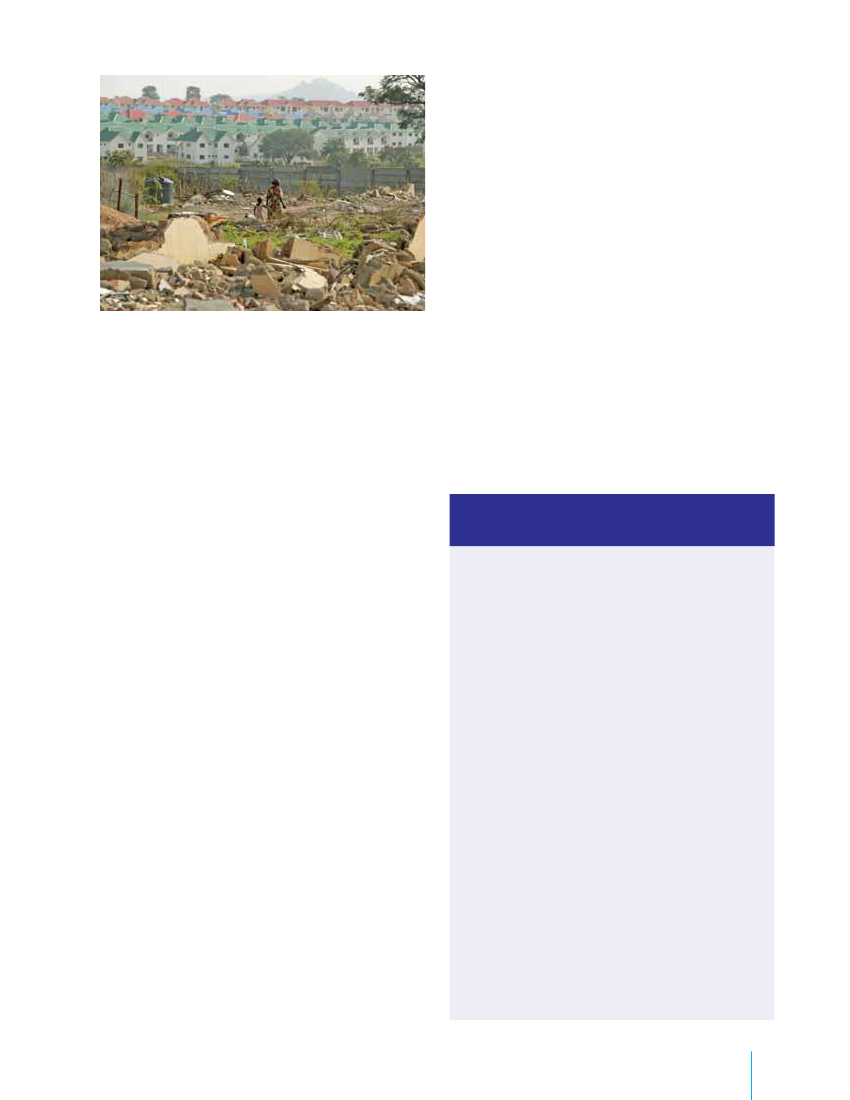
A woman and child walk among the ruins of a low-income neighbourhoodalongside a new residential development in Abuja, Nigeria.
the slum stands in the way of a major redevelopment.They may come without warning, let alone consulta-tion, and very often proceed without compensation orinvolve moving to an unfeasible location. The evictionsthemselves cause major upheaval and can destroy long-established economic and social systems and supportnetworks – the existence of which should come as nosurprise if one ponders what it takes to survive andadvance in such challenging settings. Even those whoare not actually evicted can suffer significant stress andinsecurity from the threat of removal. Moreover, theconstant displacement and abuse of marginalized popu-lations can further hinder access to essential services.Despite their many deprivations, slum residentsprovide at least one essential service to the very soci-eties from which they are marginalized–labour. Someof it is formal and some undocumented, but almostall is low-paid – for example, as factory hands, shopassistants, street vendors and domestic workers.
� UNICEF/NYHQ2006-2606/Michael Kamber
Illegal dwellings are poor in quality, relatively cheap –though they will often still consume about a quarter ofhousehold income – and notorious for the many hazardsthey pose to health. Overcrowding and unsanitary condi-tions facilitate the transmission of disease – includingpneumonia and diarrhoea, the two leading killers of chil-dren younger than 5 worldwide. Outbreaks of measles,tuberculosis and other vaccine-preventable diseasesare also more frequent in these areas, where popula-tion density is high and immunization levels are low.In addition to other perils, slum inhabitants frequentlyface the threat of eviction and maltreatment, not just bylandlords but also from municipal authorities intent on‘cleaning up’ the area. Evictions may take place becauseof a wish to encourage tourism, because the countryis hosting a major sporting event or simply because
EM28BAFebr RGua Ory ED2012
Impoverished people, denied proper housing and securityof tenure by inequitable economic and social policies andregulations governing land use and management, resortto renting or erecting illegal and often ramshackle dwell-ings. These typically include tenements (houses that havebeen subdivided), boarding houses, squatter settlements(vacant plots or buildings occupied by people who donot own, rent or have permission to use them) and ille-gal subdivisions (in which a house or hut is built in thebackyard of another, for example). Squatter settlementsbecame common in rapidly growing cities, particularlyfrom the 1950s onward, because inexpensive housingwas in short supply. Where informal settlements wereestablished on vacant land, people were able to buildtheir own homes.
Slums: The five deprivationsThe United Nations Human SettlementsProgramme (UN-Habitat) defines a slum householdas one that lacks one or more of the following:• Access to improved waterAn adequate quantity of water that is afford-able and available without excessive physicaleffort and time• Access to improved sanitationAccess to an excreta disposal system, eitherin the form of a private toilet or a public toiletshared with a reasonable number of people• Security of tenureEvidence or documentation that can be usedas proof of secure tenure status or for protec-tion from forced evictions• Durability of housingPermanent and adequate structure in anon-hazardous location, protecting its inhabit-ants from the extremes of climatic conditionssuch as rain, heat, cold or humidity• Sufficient living areaNot more than three people sharing thesame room
Children in an increasingly urban world
5
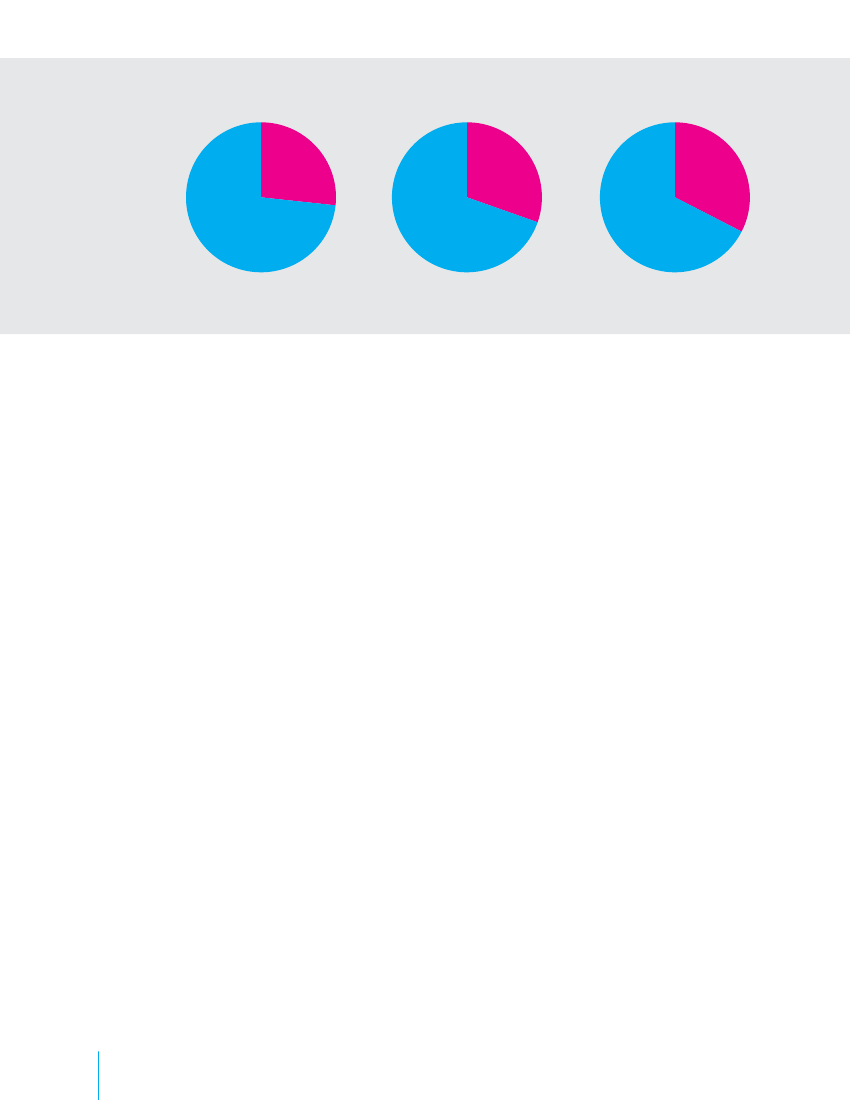
FOCUS ON
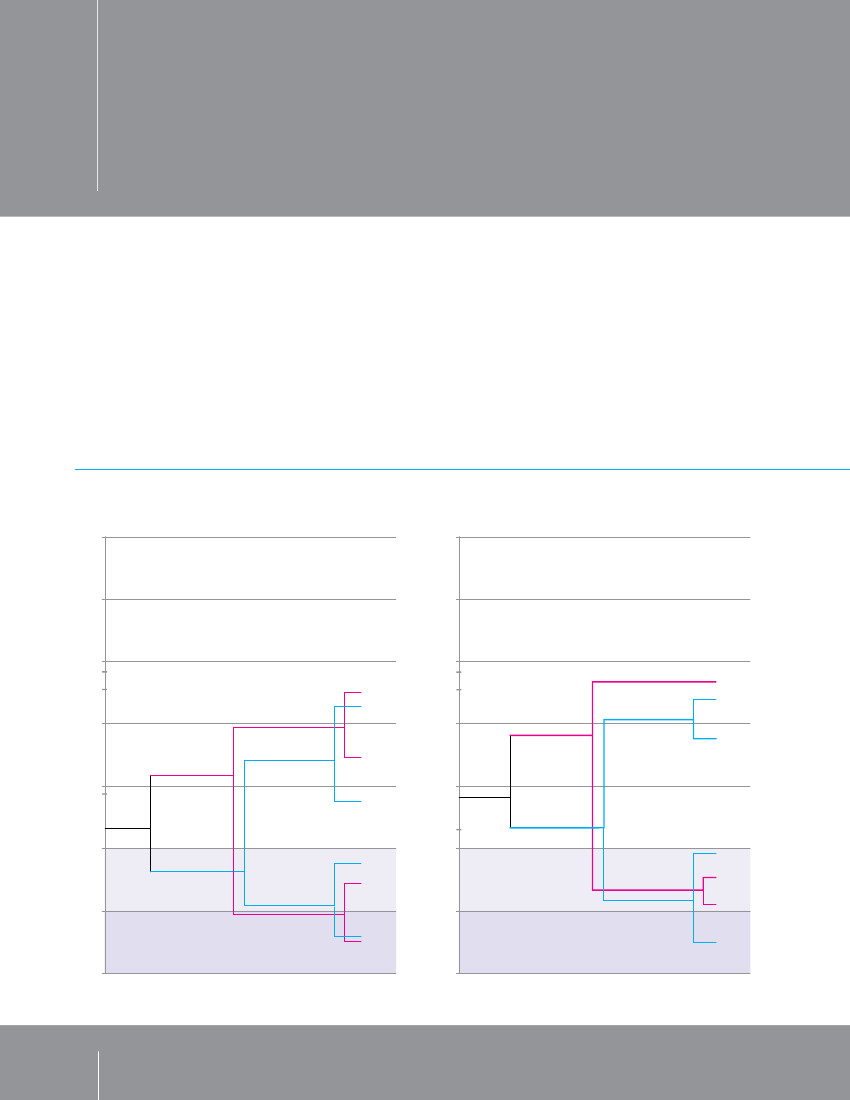
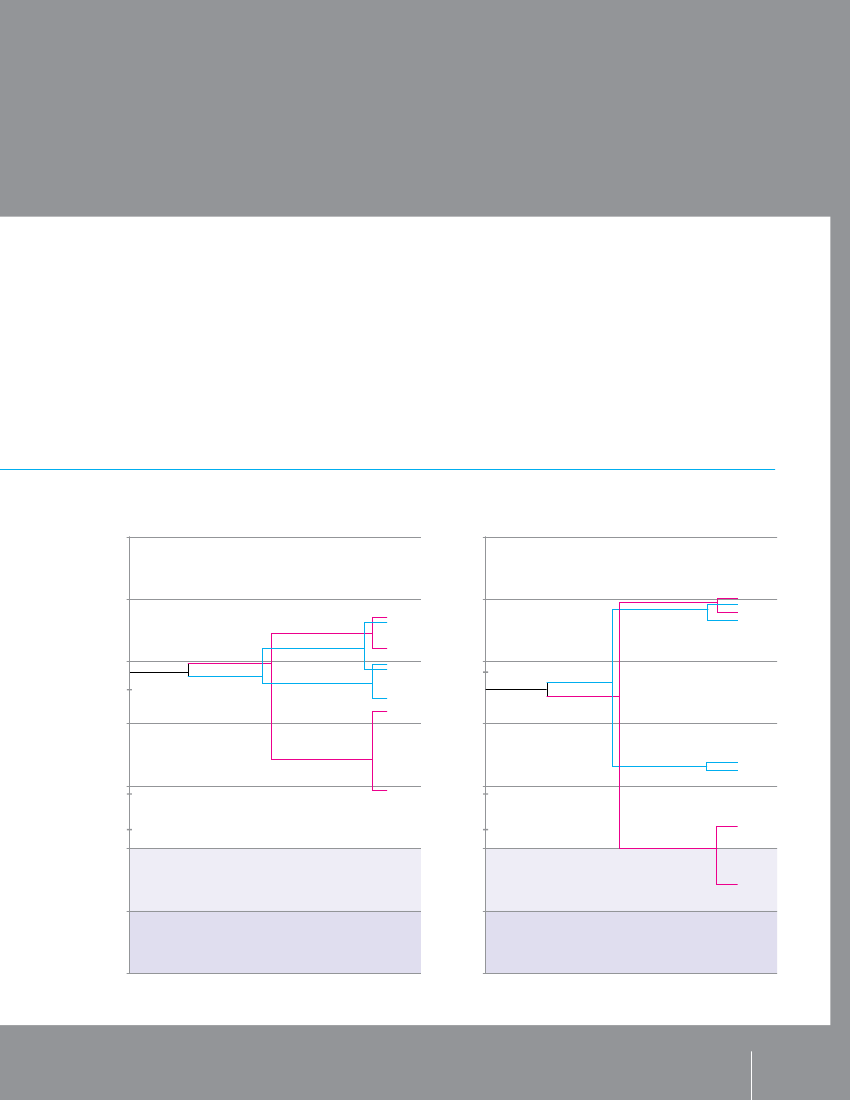
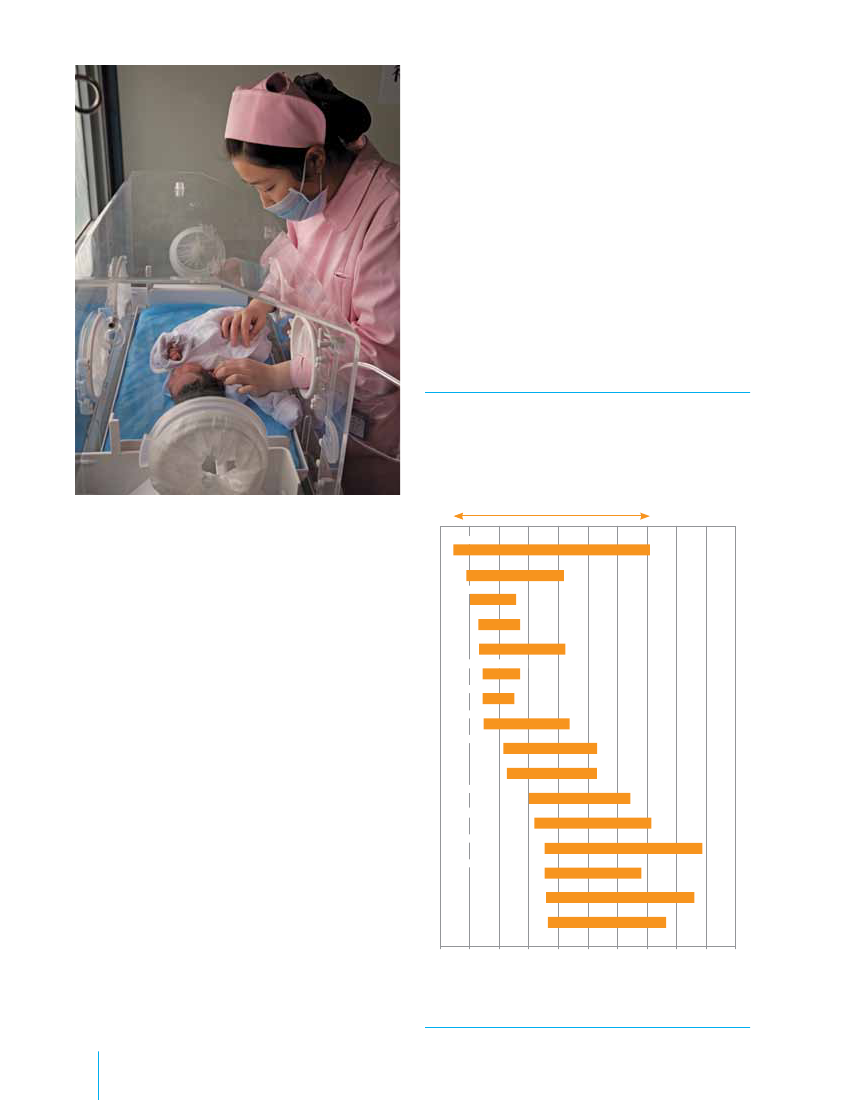
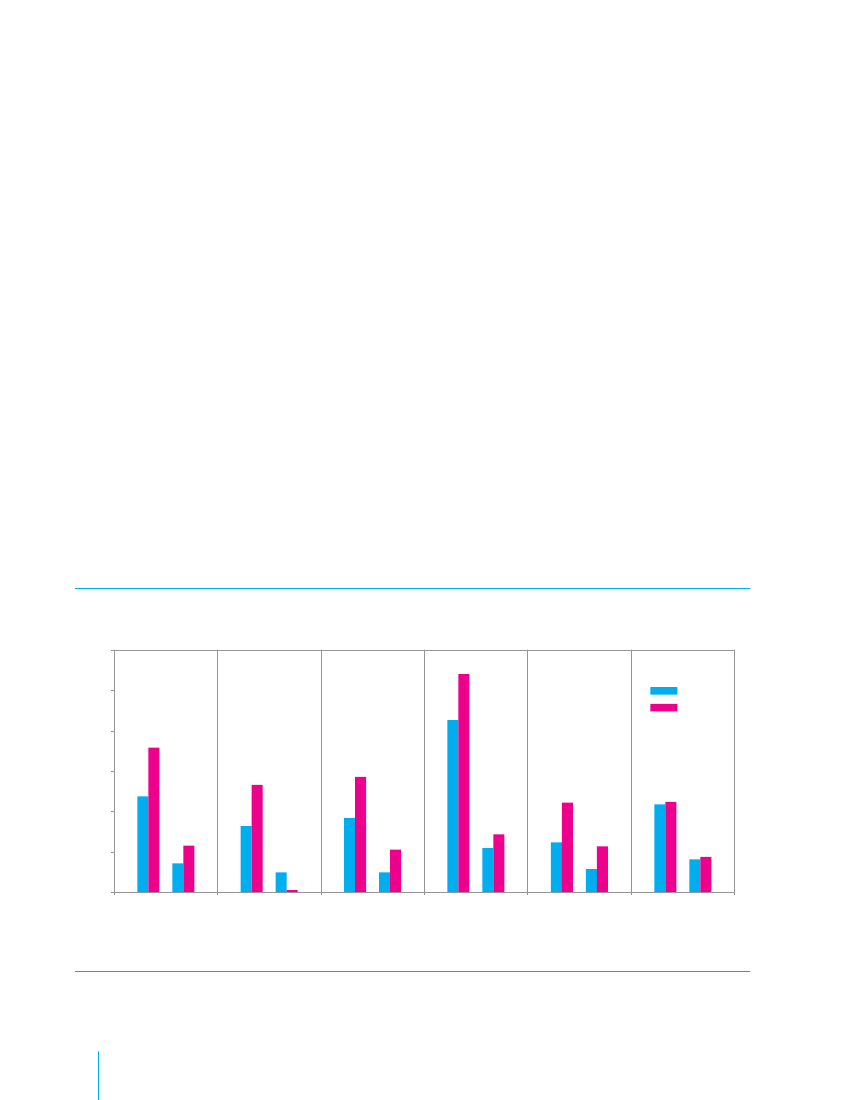
URBAN DISPARITIESnational averages are disaggregated, itbecomes clear that many children living inurban poverty are clearly disadvantagedand excluded from higher educa-tion, health services and other benefitsenjoyed by their affluentpeers.The figures below, called ‘equity trees’,illustrate that, while vast disparities exist inrural areas, poverty also can severely limita child’s education in urban areas – in somecases, more so than in the countryside.In Benin, Pakistan, Tajikistan andVenezuela (Bolivarian Republic of), theeducation gap between the richest 20per cent and the poorest 20percent isgreater in urban than in rural areas. Thegap is widest in Venezuela, where pupilsfrom the richest urban families have, onaverage, almost eight years more school-ing than those from the poorest ones,compared with a gap of 5 years betweenthe wealthy and poor in rural areas. InBenin, Tajikistan and Venezuela, children
On average, children in urban areas aremore likely to survive infancy and earlychildhood, enjoy better health and havemore educational opportunity than theircounterparts in rural areas. This effect isoften referred to as the ‘urban advantage’.Nevertheless, the scale of inequalitywithin urban areas is a matter of greatconcern. Gaps between rich and poor intowns and cities can sometimes equal orexceed those found in rural areas. When
Figure 1 .3 . Educational attainment can be most unequal in urban areasAverage years of schooling among population aged 17–22, by location, wealth and gender14
12
10
TajikistanVenezuela (BolivarianRepublic of)
EM28BAFebr RGua Ory ED2012Benin14
Pakistan
12
10
Tajikistan
urban richest 20%rural richest 20%
Average years of schooling
8
urban richest 20%rural richest 20%
Average years of schooling
malemale
Venezuela (BolivarianRepublic of)
femalemalemale
8
urban
female
urban6
female
PakistanBenin
6
female
Pakistan
Benin4
ruralmale
4
ruralEducation poverty
malemale
urban poorest 20%2Education poverty
malefemale
rural poorest 20%urban poorest 20%femalefemale0
2
rural poorest 20%
femaleExtreme education poverty
0
Extreme education poverty
Source:UNICEF analysis based on UNESCO Deprivation and Marginalization in Education database (2009) using household survey data: Benin (DHS, 2006);Pakistan (DHS, 2007); Tajikistan (MICS, 2005); Venezuela (Bolivarian Republic of) (MICS, 2000).
6
THESTATE OF THE WORLD’S CHILDREN 2012STATE OF THE WORLD’S CHILDREN 2012
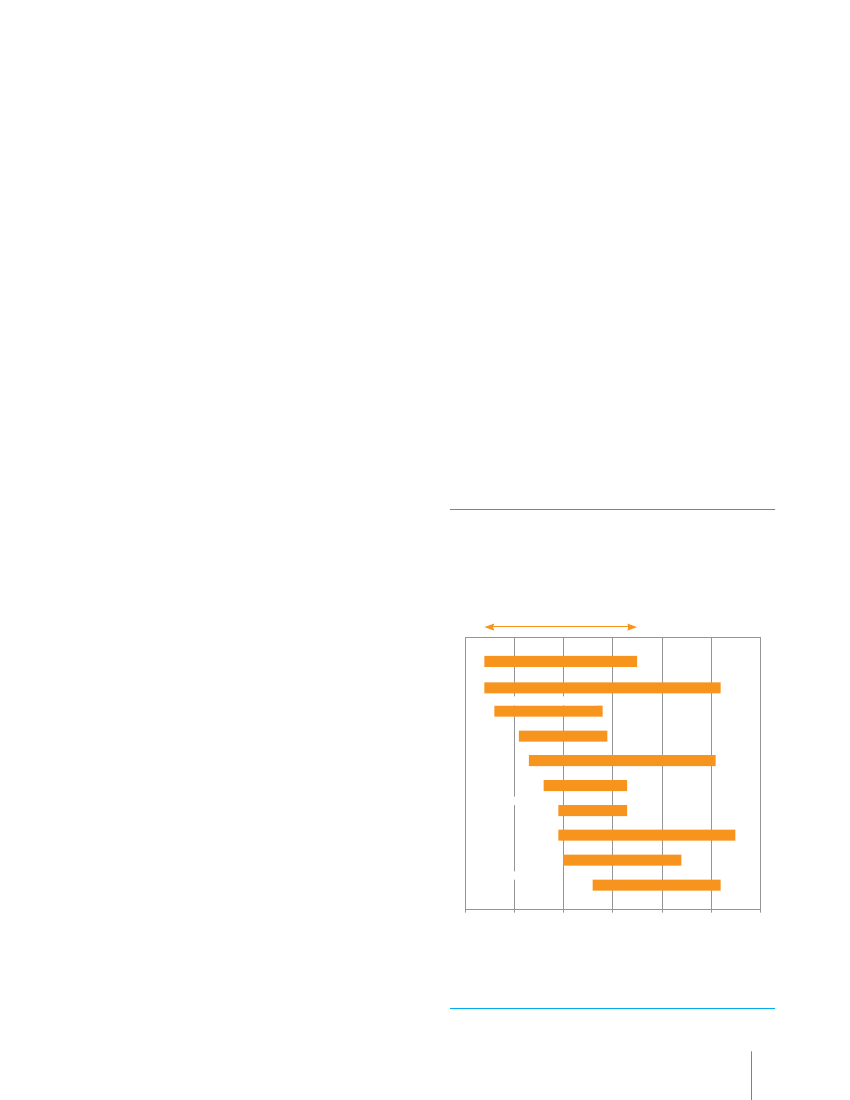
from the poorest urban households arelikely to have fewer years of school-ing not only than children from wealthierurban households but also than theirrural counterparts.Some disparities transcend location.Girls growing up in poor households areat a great disadvantage regardless ofwhether they live in urban or rural areas.In Benin, girls in urban and rural areaswho come from the poorest 20 per cent
of the population receive less than twoyears of schooling, compared with threeto four years for their male counterpartsand about nine years for the richest boysin urban and rural settings. In Pakistan,the difference in educational attain-ment between the poorest boys and girlsis about three years in rural areas andabout one year in urban areas.The gender gap is more pronounced forpoor girls in urban Tajikistan. On average,
14
EM28BAFebr RGua Ory ED2012Tajikistan1412
they receive less than six years of educa-tion, compared with almost nine years forpoor girls in rural areas. Butthe gendergap is reversed in Venezuela, where thepoorest boys in urban areas receive theleast education – less than threeyearsof schooling, compared to four and ahalfyears for the poorest girls in urbansettings and about six and a half years forthe poorest boys and girls in rural areas.
Venezuela (Bolivarian Republic of)
12
urban richest 20%rural richest 20%
urban richest 20%rural richest 20%rural poorest 20%
malemale
femalefemalemalemale
10
Tajikistan
urbanrural
femalemalefemale
10
Average years of schooling
8
Average years of schooling
Venezuela (BolivarianRepublic of)
femalemale
TajikistanVenezuela(BolivarianRepublic of)
ruralurban
8
urban poorest 20%
rural poorest 20%
malefemale
6
PakistanBenin
female
6
PakistanBeninfemale
4
4
urban poorest 20%
male2Education poverty2Education poverty
0
Extreme education poverty
0
Extreme education poverty
Children in an increasingly urban worldChildren in an increasingly
7
Children juggle to make money on the streets of Salvador, capital of the eastern state of Bahia, Brazil.
Meeting the challengesof an urban future
Children and adolescents are, of course, among the mostvulnerable members of any community and will dispro-portionately suffer the negative effects of poverty andinequality. Yet insufficient attention has been given tochildren living in urban poverty. The situation is urgent,and international instruments such as the Conventionon the Rights of the Child and commitments such asthe MDGs can help provide a framework for action.The fast pace of urbanization, particularly in Africa andAsia, reflects a rapidly changing world. Developmentpractitioners realize that standard programmingapproaches, which focus on extending services to morereadily accessible communities, do not always reachpeople whose needs are greatest. Disaggregated datashow that many are being left behind.Cities are not homogeneous. Within them, and partic-ularly within the rapidly growing cities of low- andmiddle-income countries, reside millions of childrenwho face similar, and sometimes worse, exclusion anddeprivation than children living in rural areas.In principle, the deprivations confronting childrenin urban areas are a priority for human rights-based8THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
development programmes. In practice, and particu-larly given the misperception that services are withinreach of all urban residents, lesser investment has oftenbeen devoted to those living in slums and informalurban settlements.For this to change, a focus on equity is needed – one inwhich priority is given to the most disadvantaged chil-dren, wherever they live.The first requirement is toimprove understandingof the scale and nature of urban poverty and exclu-sion affecting children.This will entail not only soundstatistical work – a hallmark of which must be greaterdisaggregation of urban data – but also solid researchand evaluation of interventions intended to advancethe rights of children to survival, health, development,sanitation, education and protection in urban areas.Second, development solutions mustidentify andremove the barriers to inclusionthat prevent marginal-ized children and families from using services, exposethem to violence and exploitation, and bar them fromtaking part in decision-making. Among other neces-sary actions, births must be registered, legal statusconferred and housing tenure made secure.
� UNICEF/NYHQ2006-1335/Claudio Versiani
Fourth, policy and practice mustpromote partner-ship between the urban poor and government at all itslevels.Urban initiatives that foster such participation –and in particular those that involve children and youngpeople – report better results not only for children butalso for their communities.Finally, everyone mustwork together to achieve resultsfor children.International, national, municipal andcommunity actors will need to pool resources andenergies in support of the rights of marginalized andimpoverished children growing up in urban environ-ments. Narrowing the gaps to honour internationalcommitments to all children will require additionalefforts not only in rural areas but also within cities.
Children put their sprawling slum on the map – literally. The data theyhave gathered about Rishi Aurobindo Colony, Kolkata, India, will beuploaded to Google Earth.
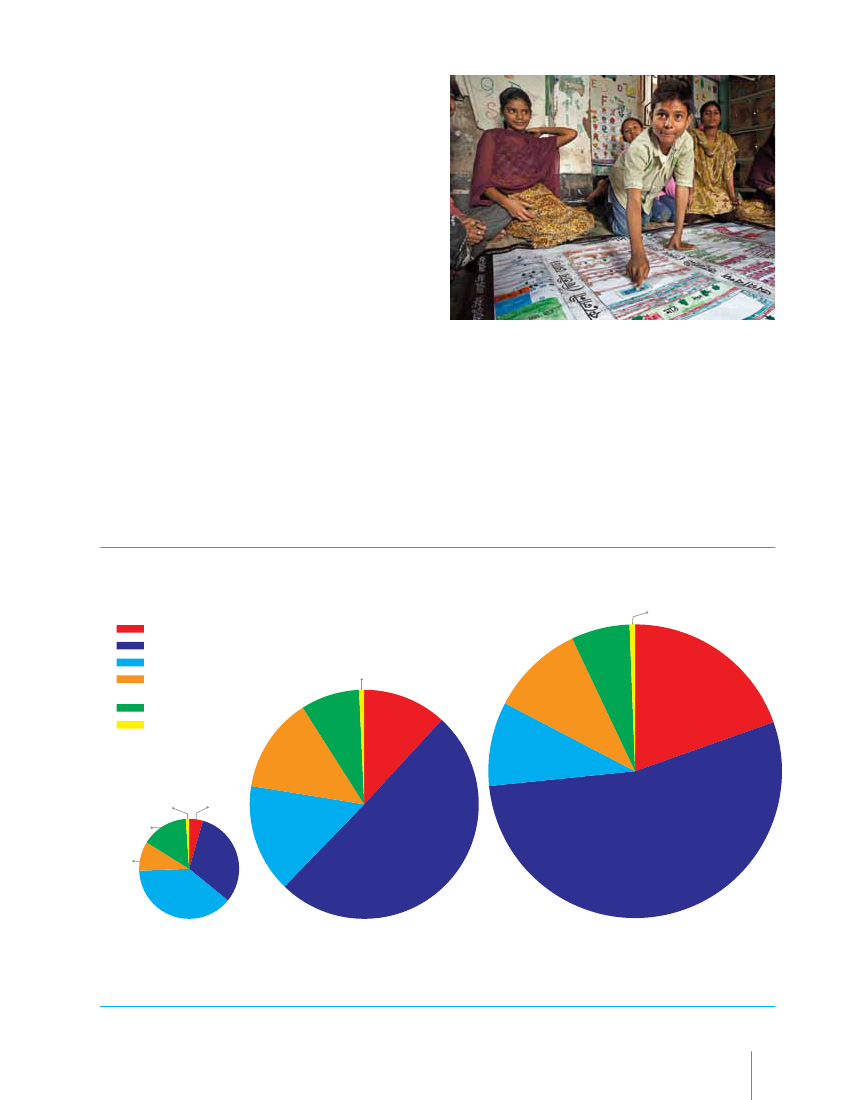
Figure 1 .4 . Urban populations are growing fastest in Asia and AfricaWorld urban population 1950, 2010, 2050 (projected)
EM28BAFebr RGua Ory ED2012
Clearly, children’s rights cannot be fulfilled and protectedunless governments, donors and international organi-zations look behind the broad averages of developmentstatistics and address the urban poverty and inequalitythat characterize the lives of so many children.
1%
AfricaAsiaEurope
Latin Americaand the CaribbeanNorth AmericaPacific
1%
6%
10%
20%
8%
12%
14%1% 5%15%10%38%19500 .7 billionSource:UNDESA, Population Division.
9%
15%31%
50%
54%
20103 .5 billion
2050 (projected)6 .3 billion
Children in an increasingly urban world
9
� UNICEF/INDA2011-00105/Graham Crouch
Third, asharp focus on the particular needs andpriorities of childrenmust be maintained in urban plan-ning, infrastructure development, service delivery andbroader efforts to reduce poverty and disparity. Theinternational Child-Friendly Cities Initiative providesan example of the type of consideration that must begiven children in every facet of urban governance.
URBAN (AREA)The definition of ‘urban’ varies from country to country, and,with periodic reclassification, can also vary within one coun-try over time, making direct comparisons difficult. An urbanarea can be defined by one or more of the following: admin-istrative criteria or political boundaries (e.g., area within thejurisdiction of a municipality or town committee), a thresholdpopulation size (where the minimum for an urban settle-ment is typically in the region of 2,000 people, although thisvaries globally between 200 and 50,000), population density,economic function (e.g., where a significant majority of thepopulation is not primarily engaged in agriculture, or wherethere is surplus employment) or the presence of urban char-acteristics (e.g., paved streets, electric lighting, sewerage).In2010, 3.5 billion people lived in areas classified as urban.
containing the city proper, suburbs and continuouslysettled commuter areas or adjoining territory inhabited aturban levels of residential density.Large urban agglomerations often include several adminis-tratively distinct but functionally linked cities. For example,the urban agglomeration of Tokyo includes the cities ofChiba, Kawasaki, Yokohama and others.METROPOLITAN AREA/REgIONA formal local government area comprising the urbanarea as a whole and its primary commuter areas, typicallyformed around a city with a large concentration of people(i.e., a population of at least100,000).In addition to the city proper, a metropolitan area includes
DEFINITIONS
The (relative or absolute) increase in thenumber of peoplewho live in towns and cities. The pace of urban populationlation and the population gained by urban areas throughrural settlements into cities and towns.URBANIzATION
growth depends on the natural increase of the urban popu-both net rural-urban migration and the reclassification of
The proportion of a country that is urban.RATE OF URBANIzATION
The increase in the proportion of urban population over
time, calculated as the rate of growth of the urban popu-lation minus that of the total population. Positive rates offaster rate than the total population.CITy PROPER
urbanization result when the urban population grows at a
The population living within the administrative boundariesof a city, e.g., Washington, D.C.Because city boundaries do not regularly adapt to accom-modate population increases, the concepts ofurbanagglomerationandmetropolitan areaare often used toimprove the comparability of measurements of city popula-tions across countries and over time.URBAN AggLOMERATIONThe population of a built-up or densely populated areaIn 2009, 21 urban agglomerations qualified as megacities,accounting for 9.4 per cent of the world’s urban popula-tion. In 1975, New York, Tokyo and Mexico City were the onlymegacities. Today, 11 megacities are found in Asia, 4 in LatinAmerica and 2 each in Africa, Europe and North America.Eleven of these megacities are capitals of their countries.MEgACITyAn urban agglomeration with a population of 10 millionor more.
10
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012URBAN SPRAWLPERI-URBAN AREA
URBAN gROWTH
both the surrounding territory with urban levels of residen-tial density and some additional lower-density areas thatare adjacent to and linked to the city (e.g., through frequenttransport, road linkages or commuting facilities). Examples ofmetropolitan areas include Greater London and Metro Manila.
Also ‘horizontal spreading’ or ‘dispersed urbanization’. Theuncontrolled and disproportionate expansion of an urbanarea into the surrounding countryside, forming low-density,poorly planned patterns of development. Common in bothhigh-income and low-income countries, urban sprawl ischaracterized by a scattered population living in separateresidential areas, with long blocks and poor access, oftenoverdependent on motorized transport and missing well-defined hubs of commercial activity.
An area between consolidated urban and rural regions.
Megacities, 2009 (population in millions)1Tokyo, Japan (36.5)2Delhi, India (21.7)3Sao Paulo, Brazil (20.0)4Mumbai, India (19.7)6New York-Newark,United States (19.3)7Shanghai, China (16.3)8Kolkata, India (15.3)9Dhaka, Bangladesh (14.3)10Buenos Aires,Argentina (13.0)11Karachi, Pakistan (12.8)12Los Angeles-Long Beach-Santa Ana,United States (12.7)13Beijing, China (12.2)15Manila, Philippines (11.4)16Osaka-Kobe, Japan (11.3)17Cairo, Egypt (10.9)18Moscow, RussianFederation (10.5)19Paris, France (10.4)20Istanbul, Turkey (10.4)21Lagos, Nigeria (10.2)
spark business and change the nature and function ofindividual towns and cities, promoting regional economicgrowth but also often reinforcing urban primacy andunbalanced regional development.Examples include the industrial corridor developingbetween Mumbai and Delhi in India; the manufacturingand service industry corridor running from Kuala Lumpur,Malaysia, to the port city of Klang; and the regionaleconomic axis forming the greater Ibadan-Lagos-Accraurban corridor in West Africa.CITy-REgIONAn urban development on a massive scale: a major citythat expands beyond administrative boundaries to engulfsmall cities, towns and semi-urban and rural hinterlands,sometimes expanding sufficiently to merge with othercities, forming large conurbations that eventually becomecity-regions.
5Mexico City, Mexico (19.3)14Rio de Janeiro, Brazil (11.8)
Sources:UNDESA, Population Division; UN-Habitat.
METACITy20 million people.
A major conurbation – a megacity of more than
As cities grow and merge, new urban configurations arecity-regions.MEgAREgION
formed. These includemegaregions, urban corridorsand
A rapidly growing urban cluster surrounded by low-density hinterland, formed as a result of expansion,
growth and geographical convergence of more than onemetropolitan area and other agglomerations. Commonin North America and Europe, megaregions are nowexpanding in other parts of the world and are charac-
terized by rapidly growing cities, great concentrationssignificant economic innovation and potential.
of people (including skilled workers), large markets and
Examples include the Hong Kong-Shenzhen-Guangzhoumegaregion (120 million people) in China and the Tokyo-Nagoya-Osaka-Kyoto-Kobe megaregion (predicted toreach 60 million by 2015) in Japan.URBAN CORRIDORA linear ‘ribbon’ system of urban organization: cities ofvarious sizes linked through transportation and economicaxes, often running between major cities. Urban corridors
EM28BAFebr RGua Ory ED2012current population of over 17 million.10 million +
For example, the Cape Town city-region in South Africaextends up to 100 kilometres, including the distancesthat commuters travel every day. The extended Bangkokregion in Thailand is expected to expand another 200 kilo-metres from its centre by 2020, growing far beyond its
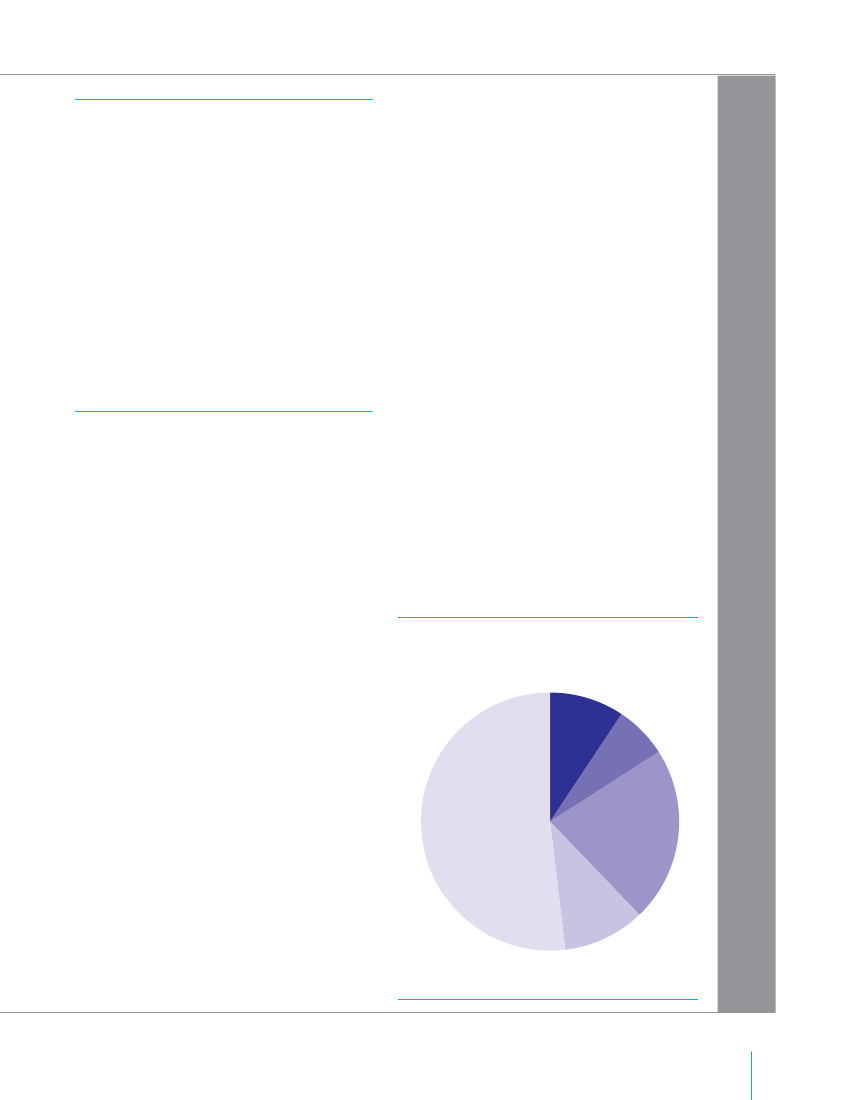
Figure 1 .5 . Half of the world’s urban populationlives in cities of fewer than 500,000 inhabitantsWorld urban population distribution, by city size, 2009
9%
5 to 10million
7%Fewer than500,0001 to 5 million
52%500,000 to1 million
22%
10%
Source:Calculations based on UNDESA,World Urbanization Prospects:The 2009 revision.
Children in an increasingly urban world
11
CHAPTER
2
EM28BAFebr RGua Ory ED2012� UNICEF/NYHQ2008-1027/Christine Nesbitt
Children’s rightsin urban settingsChildren whose needs are greatest are also those whoface the greatest violations of their rights. The mostdeprived and vulnerable are most often excluded fromprogress and most difficult to reach. They requireparticular attention not only in order to secure theirentitlements, but also as a matter of ensuring therealization of everyone’s rights.
Children living in urban poverty have the full rangeof civil, political, social, cultural and economic rightsrecognized by international human rights instruments.The most rapidly and widely ratified of these is theConvention on the Rights of the Child. The rights ofevery child include survival; development to the fullest;protection from abuse, exploitation and discrimina-tion; and full participation in family, cultural and sociallife. The Convention protects these rights by detailingcommitments with respect to health care, education,and legal, civil and social protection.All children’s rights are not realized equally. Overone third of children in urban areas worldwide go
EM28BAFebr RGua Ory ED2012
unregistered at birth – and about half the children inthe urban areas of sub-Saharan Africa and South Asiaare unregistered. This is a violation of Article 7 of theConvention on the Rights of the Child. The invisibil-ity that derives from the lack of a birth certificate or anofficial identity vastly increases children’s vulnerabilityto exploitation of all kinds, from recruitment by armedgroups to being forced into child marriage or hazard-ous work. Without a birth certificate, a child in conflictwith the law may also be treated and punished as anadult by the judicial system.1Even those who avoidthese perils may be unable to access vital services andopportunities – including education.Obviously, registration alone is no guarantee of accessto services or protection from abuse. But the obliga-tions set out by the Convention on the Rights of theChild can be easily disregarded when whole settle-ments can be deemed non-existent and people can,in effect, be stripped of their citizenship for wantof documentation.
Children’s rights in urban settings
13
Inadequate living conditions are among the mostpervasive violations of children’s rights. The lack ofdecent and secure housing and such infrastructure aswater and sanitation systems makes it so much moredifficult for children to survive and thrive. Yet, theattention devoted to improving living conditions hasnot matched the scope and severity of the problem.Evidence suggests that more children want for shelterand sanitation than are deprived of food, educationand health care, and that the poor sanitation, lack ofventilation, overcrowding and inadequate natural lightcommon in the homes of the urban poor are responsi-ble for chronic ailments among their children.2Manychildren and families living in the urban slums of low-income countries are far from realizing the rights to“adequate shelter for all” and “sustainable humansettlements development in an urbanizing world”enshrined in the Istanbul Declaration on HumanSettlements, or Habitat Agenda, of 1996.3Since children have the rights to survival, adequatehealth care and a standard of living that supports theirfull development, they need to benefit from environ-mental conditions that make the fulfilment of theserights possible. There is no effective right to play with-out a safe place to play, no enjoyment of health withina contaminated environment. Support for this perspec-tive is provided by such treaties and declarations asthe International Covenant on Economic, Social andCultural Rights; the Convention on the Eliminationof All Forms of Discrimination against Women; theHabitat Agenda; and Agenda 21, the action planadopted at the 1992 United Nations Conference onEnvironment and Development. The Centre onHousing Rights and Evictions, among others,documents the extensive body of rights relatedto housing and the disproportionate vulnerabil-ity of children to violations of these rights. Inrecent years, practical programming aimed atfulfilling rights has been focused on the pursuit ofthe Millennium Development Goals (MDGs), all ofwhich have relevant implications for children in urbanpoverty. One of the targets of MDG 7 – to ensureenvironmental sustainability – focuses specificallyon improving the lives of at least 100 million of the
A mother holding a one-year-old infant obtains micronutrient powderfrom social workers in Dhaka, Bangladesh. Micronutrient deficienciescan lead to anaemia, birth defects and other disorders.
14
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012HealthChild survival
world’s slum dwellers by 2020. This is only a smallpercentage of those who live in slums worldwide; thetarget does not address the continuing growth in thenumber of new slums and slum dwellers.This chapter looks at the situation of children inurban settings and considers in particular their rightsto health; water, sanitation and hygiene; educationandprotection.
Article 6 of the Convention on the Rights of theChild commits States parties to “ensure to the maxi-mum extent possible the survival and developmentof the child.” Article 24 refers to every child’s right tothe “enjoyment of the highest attainable standard ofhealth and to facilities for the treatment of illness andrehabilitation of health.” The Convention urges Statesparties to “ensure that no child is deprived of his or herright of access to such health care services.”
Nearly 8 million children died in 2010 before reach-ing the age of 5, largely due to pneumonia, diarrhoeaand birth complications. Some studies show thatchildren living in informal urban settlements areparticularly vulnerable.4High urban child mortal-ity rates tend to be seen in places where significantconcentrations of extreme poverty combine withinadequate services, as in slums.
� UNICEF/NYHQ2009-0609/Shehzad Noorani
An environment for fulfillingchild rights
PERSPECTIVE
OUT OF SIGHT,OUT OF REACHby Her Majesty Queen Rania Al Abdullah of Jordan,UNICEF Eminent Advocate
The contrast could not be more ironic.Cities, where children flourish with goodschools and accessible health care, arewhere they also suffer greatly, deniedtheir basic human rights to an educa-tion and a life of opportunity. Side byside, wealth juxtaposed against poverty,nowhere else is the iniquity of inequity asobvious as in a city.
Over the course of a decade, the state ofthe world’s urban children has worsened.The number of people living in slumshas increased by over 60 million. Theseare mothers and fathers, grandmothersand grandfathers, sons and daughters,scratching out a life in shantytowns theworld over. With the direct disadvan-tages of urban poverty – disease, crime,violence – come indirect ones, social and
EM28BAFebr RGua Ory ED2012In the Arab world the facts are clear:More than one third of the urbanpopulation lives in informal settlementsand slums. These environments arehazardous to children; a lack of adequatesanitation and drinkable water poses amajor threat to their well-being. In someless developed Arab countries, over-crowding in makeshift houses furtheraggravates the precarious health condi-tions of these vulnerable families.For Palestinian children, city life can bea grim life. Too often, it represents gunsand checkpoints, fear and insecurity.Yet their greatest hope is their nationalpride: a deep-seated belief in education,which they know is essential for build-ing a life and rebuilding their country. Yet,since 1999, across Occupied PalestinianTerritory, the number of primary-school-aged children who are out of school hasleapt from 4,000 to 110,000, a staggering2,650 per cent increase. In Gaza, amongthe world’s most densely populated areas,access to and quality of education havedeteriorated rapidly. For the sake of thesechildren’s futures and of the all-important
Half the world’s population now lives incities. Throughout history, urban life, soconcentrated with humanity, has beena catalyst for trade, ideas and opportuni-ties, making cities engines of economicgrowth. Today, living in a city is widelyregarded as the best way to find pros-perity and escape poverty. Yet hiddeninside cities, wrapped in a cloak of statis-tics, are millions of children struggling tosurvive. They are neither in rural areas norin truly urban quarters. They live in squa-lor, on land where a city has outpaceditself, expanding in population but notin vital infrastructure or services. Theseare children in slums and deprived neigh-bourhoods, children shouldering the manyburdens of living in that grey area betweencountryside and city, invisible to theauthorities, lost in a hazy world of statisti-cal averages that conceal inequality.
cultural barriers, like gender and ethnic-ity, that deny children from the slumsthe chance to enrol in and completeprimary school. Education is pushed outof reach because there are not enoughpublic schools or the costs are too high.Religious groups, non-governmentalorganizations and entrepreneurs try to fillthe gap but struggle without governmentsupport or regulation. As the best chanceto escape their parents’ destinies eludesthese children, the cycle of destitutionspins on.
search for regional peace, we must setaside our anger and angst and give themthe childhoods they deserve, childhoodswe expect for our own children, filled withhappy memories and equal opportunities.In a few Arab countries, the fates ofdisadvantaged urban children are beingrewritten. In Morocco, the governmentprogramme ‘Cities without Slums’hopes to raise the standards of nearly300,000homes. By engaging banksand housing developers, a ‘triple win’scenario is possible for poor people,the government and the private sector.Jordan, too, is making strides. Amman isone of the region’s leading child-friendlycities, with over 28,000students partici-pating in children’s municipal councils toprioritize their needs, rights and interests.The results have been impressive: parks,libraries, community spaces, educationalsupport for children who dropped out ofschool, campaigns against violence andabuse, and information and communica-tion technology centres for the deaf.Yet for Arab children – forallchildren – tothrive, nations have to work together. Wehave to share resources, adopt and adaptsuccessful initiatives from around theglobe and encourage our private sectorsto engage with disadvantaged families sowe can catch those falling through thecracks. In cities across the world, chil-dren out of reach are too often out ofsight. If we are to raise their hopes andtheir prospects, we have to dig deep intothe data, unroot entrenched prejudicesand give every child an equal chance atlife. Only in this way can we truly advancethe state ofallthe world’s children.
Children’s rights in urban settings
15
The Convention on the Rights of the ChildThe Convention on the Rights of the Child, adopted in 1989,was the first international treaty to state the full range of civil,political, economic, social and cultural rights belonging tochildren. The realities confronting children can be assessedagainst the commitments to which it holds States parties.Legally binding on States parties, the Convention detailsuniversally recognized norms and standards concerning theprotection and promotion of the rights of children – everywhereand at all times. The Convention emphasizes the complementar-ity and interdependence of children’s human rights. Across its54 articles and 2 Optional Protocols, it establishes a new visionof the child – one that combines a right to protection throughthe State, parents and relevant institutions with the recognitionthat the child is a holder of participatory rights and freedoms.All but three of the world’s nations – Somalia, South Sudan andthe United States of America – have ratified the document.This broad adoption demonstrates a common political will toprotect and ensure children’s rights, as well as recognitionthat, in the Convention’s words, “in all countries in the world,there are children living in exceptionally difficult conditions,and that such children need special consideration.”The values of the Convention stem from the 1924 GenevaDeclaration of the Rights of the Child, the 1948 UniversalDeclaration of Human Rights and the 1959 Declaration of theRights of the Child. The Convention applies to every child,defined as every person younger than 18 or the age of major-ity, if this is lower (Article 1). The Convention also requiresthat in all actions concerning children, “the best interests ofthe child shall be a primary consideration,” and that Statesparties “ensure the child such protection and care as isnecessary for his or her well-being” (Article 3).Furthermore, “a mentally or physically disabled child shouldenjoy a full and decent life, in conditions which ensuredignity, promote self-reliance and facilitate the child’s activeparticipation in the community” (Article 23). This extends tothe right to special care, provided free of charge wheneverpossible, and effective access to education, training, healthcare, rehabilitation services, recreation opportunities andpreparation for employment.ParticipationOne of the core principles of the Convention is respect forand consideration of the views of children. The documentrecognizes children’s right to freely express their views in allmatters affecting them and insists that these views be givendue weight in accordance with the age and maturity of thechildren voicing them (Article 12). It further proclaims chil-dren’s right to freedom of all forms of expression (Article 13).Children are entitled to freedom of thought, conscience andreligion (Article 14), to privacy and protection from unlawfulattack or interference (Article 16) and to freedom of associationand peaceful assembly (Article 15).Social protectionThe Convention acknowledges the primary role of parentsor legal guardians in the upbringing and development ofthe child (Article 18) but stresses the obligation of the Stateto support families through “appropriate assistance,” “thedevelopment of institutions, facilities and services for thecare of children” and “all appropriate measures to ensurethat children of working parents have the right to benefit fromchild-care services and facilities for which they are eligible.”Of particular relevance in the urban context is the recognitionof “the right of every child to a standard of living adequatefor the child’s physical, mental, spiritual, moral and socialdevelopment” (Article 27). The responsibility to secure theseconditions lies mainly with parents and guardians, but Statesparties are obliged to assist and “in case of need providematerial assistance and support programmes, particularlywith regard to nutrition, clothing and housing.” Children havethe right to benefit from social security on the basis of theircircumstances (Article 26).Health and environmentStates parties are obliged to “ensure to the maximum extentpossible the survival and development of the child” (Article6). Each child is entitled to the “enjoyment of the highestattainable standard of health and to facilities for the treat-ment of illness and rehabilitation of health” (Article 24). Thisincludes child care; antenatal, postnatal and preventive
Every child has the right to be registered immediately after birthand to have a name, the right to acquire a nationality and topreserve her or his identity and, as far as possible, the right toknow and be cared for by her or his parents (Articles 7 and 8).
Non-discriminationStates parties also take on the responsibility to protect childrenagainst discrimination. The Convention commits them torespecting and ensuring rights “to each child within their juris-diction without discrimination of any kind, irrespective of thechild’s or his or her parent’s or legal guardian’s race, colour, sex,language, religion, political or other opinion, national, ethnic orsocial origin, property, disability, birth or other status” (Article 2).Children belonging to ethnic, religious or linguistic minoritiesand those of indigenous origin have the right to practise theirown culture, religion and language in the community (Article 30).
16
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
care; family planning; and education on child health, nutrition,hygiene, environmental sanitation, accident prevention andthe advantages of breastfeeding. In addition to ensuring provi-sion of primary health care, States parties undertake to combatdisease and malnutrition “through the provision of adequatenutritious foods and clean drinking water, taking into consid-eration the dangers and risks of environmental pollution.”Education, play and leisureThe Convention establishes the right to education on the basisof equal opportunity. It binds States parties to make “availableand accessible to every child” compulsory and free primaryeducation and options for secondary schooling, includingvocational education (Article 28). It also obliges States partiesto “encourage the provision of appropriate and equal oppor-tunities for cultural, artistic, recreational and leisure activity”(Article 31).ProtectionStates parties recognize their obligation to provide for multipleaspects of child protection. They resolve to take all appro-priate legislative, administrative, social and educationalmeasures to protect children from all forms of physical ormental violence, injury or abuse, neglect or negligent treat-ment, maltreatment or exploitation, even while the childrenare under the care of parents, legal guardians or others(Article 19). This protection, along with humanitarian assis-tance, extends to children who are refugees or seekingrefugee status (Article 22).
Under the Convention, States are obliged to protect childrenfrom economic exploitation and any work that may interferewith their education or be harmful to their health or physical,mental, spiritual, moral or social development. Such protec-tions include the establishment and enforcement of minimumage regulations and rules governing the hours and condi-tions of employment (Article 32). National authorities shouldalso take measures to protect children from the illicit use ofnarcotic drugs and psychotropic substances (Article 33) andfrom all forms of exploitation that are harmful to any aspect oftheir welfare (Article 36), such as abduction, sale of or trafficin children (Article 35) and all forms of sexual exploitation andabuse (Article 34).
The Convention’s four core principles – non-discrimination; thebest interests of the child; the right to life, survival and devel-opment; and respect for the views of the child – apply to allactions concerning children. Every decision affecting childrenin the urban sphere should take into account the obligation topromote the harmonious development of every child.
EM28BAFebr RGua Ory ED2012Immunization
Recent research from Nigeria suggests that livingin a socio-economically disadvantaged urban areaincreases the rate of under-five mortality even after thedata have been adjusted for factors such as mother’seducation or income.5In Bangladesh, 2009 householdsurvey data indicate that the under-five mortality ratein slums is 79 per cent higher than the overall urbanrate and 44 per cent higher than the rural rate.6Aroundtwo thirds of the population of Nairobi, Kenya, livesin crowded informal settlements, with an alarmingunder-five mortality rate of 151 per thousand livebirths. Pneumonia and diarrhoeal disease are amongthe leading causes of death.7Poor water supply andsanitation, the use of hazardous cooking fuels in badlyventilated spaces, overcrowding and the need to payfor health services – which effectively puts them out ofreach for the poor – are among the major underlyingcauses of these under-five deaths.8Disparities in childsurvival are also found in high-income countries. Inlarge cities of the United States, income and ethnicityhave been found to significantly affect infant survival.9
Around 2.5 million under-five deaths are avertedannually by immunization against diphtheria, pertus-sis and tetanus (DPT) and measles. Global vaccinationcoverage is improving: 130 countries have been able toadminister all three primary doses of the DPT vaccineto 90 per cent of children younger than 1. Moreneeds to be done however. In 2010, over 19 millionchildren did not get all three primary doses ofDPT vaccination.10Lower levels of immunization contribute to morefrequent outbreaks of vaccine-preventable diseases incommunities that are already vulnerable owing to highpopulation density and a continuous influx of newinfectious agents.Poor service delivery, parents who have low levelsof education, and lack of information about immu-nization are major reasons for low coverage amongchildren in slums as diverse as those of western UttarPradesh, India, and Nairobi, Kenya.
Children’s rights in urban settings
17
� UNICEF/NYHQ2009-0266/Jia Zhao
BreastfeedingBreastfeeding is recommended during the first sixmonths of life as a way to meet infants’ nutritionalrequirements and reduce neonatal mortality byperhaps 20 per cent. There is some evidence that urbanmothers are less likely than rural ones to breastfeed –and more likely to wean their children early if they dobegin. An analysis of Demographic and Health Survey(DHS) data from 35 countries found that the percent-age of children who were breastfed was lower in urbanareas.15Low rates of breastfeeding may be attributedin part to a lack of knowledge about the importanceof the practice and to the reality that poor women inurban settings who work outside the home are oftenunable to breastfeed.
A health worker examines an infant in an incubator at Qingchuan CountyMaternity and Child Care Centre, Sichuan Province, China.
Maternal and newborn health
More than 350,000 women died in pregnancy orchildbirth in 2008,11and every year many more sustaininjuries, such as obstetric fistulae, that can turn intolifelong, ostracizing disabilities. Most of the womenwho die or are severely injured in pregnancy or child-birth reside in sub-Saharan Africa and Asia, and mostof the deaths are caused by haemorrhage, high bloodpressure, unsafe abortion or sepsis. Many of these inju-ries and deaths can be averted if expectant mothersreceive care from skilled professionals with adequateequipment and supplies, and if they have access toemergency obstetric care.12
Urban settings provide proximity to maternity andobstetric emergency services but, yet again, access anduse are lower in poorer quarters – not least becausehealth facilities and skilled birth attendants are inshorter supply.13Health services for the urban poortend to be of much lower quality, often forcing peopleto resort to unqualified health practitioners or pay apremium for health care, as confirmed by studies inBangladesh, India, Kenya and elsewhere.1418THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012Richest 20%CambodiaNepalHondurasEgyptIndiaDominican RepublicIndonesiaBangladeshPakistanHaitiSenegalRwandaGuineaUgandaNigerBenin020406080100120
Figure 2 .1 . Wealth increases the odds of survivalfor children under the age of 5 in urban areasUnder-five mortality rate (per 1,000 live births) in urbanareas inselected countries (right end of bar indicates average under-five mortality for the poorest quintile of the population; left endindicates that for the wealthiestquintile)Poorest 20%
140
160
180
200
Under-five mortality rateSource:WHO estimates and DHS, 2005–2007 Countries were selected based.on availability of data.
NutritionThe locus of poverty and undernutrition among chil-dren appears to be gradually shifting from rural to urbanareas, as the number of the poor and undernourishedincreases more quickly in urban than in rural areas.16Hunger is a clear manifestation of failure in social protec-tion. It is difficult to behold, especially when it afflictschildren. However, even the apparently well fed – thosewho receive sufficient calories to fuel their daily activities– can suffer the ‘hidden hunger’ of micronutrient malnu-trition: deficiencies of such essentials as vitamin A, ironor zinc from fruits, vegetables, fish or meat. Withoutthese micronutrients, children are in increased dangerof death, blindness, stunting and lower IQ.17The rural-urban gap in nutrition has narrowed inrecent decades – essentially because the situation hasworsened in urban areas.18In sub-Saharan Africa,a 2006 study showed that disparities in child nutri-tion between rich and poor urban communities weregreater than those between urban and rural areas.19Undernutrition contributes to more than a third ofunder-five deaths globally. It has many short- andlong-term consequences, including delayed mentaldevelopment, heightened risk of infectious diseasesand susceptibility to chronic disease in adult life.20Inlow-income countries, child undernutrition is likely tobe a consequence of poverty, characterized as it is bylow family status and income, poor environment andhousing, and inadequate access to food, safe water,guidance and health care. In a number of countries,stunting is equally prevalent, or more so, among thepoorest children in urban areas as among comparablydisadvantaged children in the countryside.21
A 2006 study of disparities in childhood nutritionalstatus in Angola, the Central African Republic andSenegal found that when using a simple urban-ruralcomparison, the prevalence of stunting was signifi-cantly higher in rural areas. But when urban and ruralpopulations were stratified using a measure of wealth,the differences in prevalence of stunting and under-weight between urban and rural areas disappeared.24A 2004 study of 10 sub-Saharan African countriesshowed that the energy-deficient proportion of theurban population was above 40 per cent in almostall countries and above 70 per cent in three: Ethiopia,Malawi and Zambia.25At the opposite end of the nutrition spectrum, obesityafflicts children in urban parts of high-income coun-tries and a growing number of low- and middle-incomecountries.26A diet of saturated fats, refined sugars andsalt combined with a sedentary lifestyle puts childrenat increased risk of obesity and chronic ailments suchas heart disease, diabetes and cancer.27
A study of the National Family Health Survey (NFHS-3)in eight cities in India from 2005 to 2006 found thatlevels of undernutrition in urban areas continue to bevery high. At least a quarter of urban children under5 were stunted, indicating that they had been under-nourished for some time. Income was a significantfactor. Among the poorest fourth of urban residents,54 per cent of children were stunted and 47percentwere underweight, compared with 33 per cent and26percent, respectively, among the rest of the urbanpopulation.22The largest differences were observed inthe proportion of underweight children in slum andnon-slum areas of Indore and Nagpur.23
EM28BAFebr RGua Ory ED2012Richest 20%PeruCambodiaBolivia (Plurinational State of)GhanaBangladeshKenyaSierra LeoneIndiaNigeriaMadagascar0%10%20%30%Source:DHS, 2006–2010.
Figure 2 .2 . Children of the urban poor are morelikely to be undernourishedThe proportion of children under 5 who are stunted (right end ofbar indicates prevalence of stunting for the poorest quintile of theurban population; left end indicates that for the wealthiest quintile)Poorest 20%
40%
50%
60%
Prevalence of stuntingNote:Estimates are calculated according to WHO Child Growth Standards.Countries were selected based on availability of data.
Children’s rights in urban settings
19
FOCUS ON
MATERNAL AND CHILD HEALTHSERVICES FOR THE URBAN POORA case study from Nairobi, kenyaare exactly where most local womengo for maternal and child health care –seeking better-quality options only oncecomplications occur. In contrast to publicservices, which seldom extend to infor-mal settlements, these private facilitiesare perceived as friendly, accessible andtrustworthy, perhaps because they investmore time in building relationships withpatients. Only a small proportion of theurban poor has access to more reliablematernal health care services, includingthose offered at clinics and hospitals runby missionaries and non-governmentalorganizations.their height-for-age index falls morethan two standard deviations below themedian of the reference population; theyare severely stunted if the index is morethan three standard deviations below themedian. Stunting prevalence is a usefultool for comparisons within and betweencountries and socio-economic groups.Figure 2.3 portrays the magnitude ofinequities in child undernutrition bycomparing average stunting levels forurban Kenya against data collectedbetween 2006 and 2010 in the Korogochoand Viwandani slum settlements. Thestudy covers all women who gave birth inthe area. The children’s measurementswere taken periodically up to 35monthsof age.As the graph demonstrates, the preva-lence of stunting among children livingin slum areas increases sharply fromless than 10 per cent during the first fewmonths of life to nearly 60 per cent inthe group aged 15–17 months, and thenremains at that level. In urban Kenyaoverall, the prevalence of undernutri-tion reaches a maximum of 35 per centamong children aged 15–17 months,then declines to around 25 per cent. Thegap between the poor (here, slum resi-dents) and the non-poor in Kenya widensfrom this point. For example, among chil-dren above 15months, the prevalence ofstunting stands at around 57 per cent inthe slums and nearly 28 per cent in urbanKenya as a whole. Separate analysis (notillustrated in Figure 2.3) reveals that theprevalence of stunting among the urbanrich is close to 21 per cent, suggesting
Access to health servicesIn Nairobi slums, public provision ofhealth services is limited. A studyconducted in 2009 shows that out ofa total of 503 health facilities used byresidents of three slum communities(Korogocho, Viwandani and Kibera), only6 (1 per cent) were public, 79 (16 percent) were private not-for-profit, and 418(83 per cent) were private for-profit. Thelast category largely consists of unli-censed and often ramshackle clinicsand maternity homes, with no work-ing guidelines or standard protocols forservices. Yet these substandard facilities
20
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012Urban child undernutritionIn developing countries, child under-nutrition remains a major public healthconcern. Both a manifestation and acause of poverty, it is thought to contributeto over a third of under-five deaths glob-ally. Insufficient nutrition is one of a widerange of interlinked factors forming theso-called poverty syndrome – low income,large family size, poor education andlimited access to food, water, sanitationand maternal and child health services.Stunting, underweight and wast-ing – measured by height-for-age,weight-for-age and weight-for-height,respectively – are the three mostfrequently used anthropometric indi-cators of nutritional status. Stunting isconsidered the most reliable measureof undernutrition, as it indicates recur-rent episodes or prolonged periods ofinadequate food intake, calorie and/orprotein deficiency or persistent or recur-rent ill health. Children are stunted if
Rapid urbanization has been takingplace in Kenya – as in much of sub-Saharan Africa – largely in a contextof weak economic development andpoor governance. As a result, local andnational authorities have not been ableto provide decent living conditions andbasic social services sufficient to meetthe needs of a growing urban popula-tion. Between 1980 and 2009, the numberof people living in Nairobi, the capital,increased from 862,000 to about 3.4 million.Estimates (2007) indicate that around60 per cent live in slums covering only5 per cent of the city’s residential land.Moreover, emerging evidence revealsthat the urban population explosion inthe region has been accompanied byincreasing rates of poverty and poorhealth outcomes. The incidence of childundernutrition, morbidity and mortal-ity has been shown to be higher in slumsand peri-urban areas than in more privi-leged urban settings or, sometimes, evenrural areas.
Figure 2 .3 . Stunting prevalence among children under 3 years old:Comparing the Nairobi slums with overall urban kenya70%
Nairobi slumsUrban kenya60%
50%
40%
30%
20%
10%
0%1–33–5
Source:Urbanization, Poverty and Health Dynamics – Maternal and Child Health data (2006–2009);African Population and Health Research Center; and Kenya DHS (2008–2009).
that children in urban poverty are nearly2.7 times as likely to be stunted.Effective interventions to reduce childundernutrition may include micronutrientsupplementation (iodine, iron and vitaminA); food supplementation (for micronu-trient deficiencies); infection preventionand treatment; growth monitoring and
EM28BAFebr RGua Ory ED20126–89–1112–1415–1718–2021–2324–2930–35
Goals 1 (eradicating extreme poverty andhunger), 4 (reducing child mortality) and5 (improving maternal health). In additionto a strong focus on health and nutritionalinterventions (e.g., antenatal, maternaland neonatal care, immunization,appropriate feeding practices), theimportance of reproductive health isbeing recognized in this context, asfamily planning can be a cost-effectiveand high-yield approach to improvingthe health of mothers and children. TheUrban Reproductive Health Initiative,sponsored by the Bill & Melinda GatesFoundation and currently implementedin selected urban areas of India, Kenya,Nigeria and Senegal, is an example.The programme seeks to significantlyincrease modern contraceptive preva-lence rates – especially among the urbanand peri-urban poor – through integratingand improving the quality of family plan-ning services, particularly in high-volumesettings; increasing provision, includ-ing through public-private partnerships;and dismantling demand-side barrierstoaccess.by Jean Christophe FotsoHead, Population Dynamics and Reproductive Health,African Population and Health Research Center,Nairobi, Kenya.The African Population and Health Research Center(APHRC) is an international non-profit organizationwhose mission is to promote the well-being of Africansthrough policy-relevant research on key population andhealth issues. Originally established as a programmeof the Population Council in 1995, APHRC has beenautonomous since 2001 and now has offices in Kenya,Nigeria and Senegal. The Center focuses on research,strengthening research capacity and policy engagementin sub-Saharan Africa.
Child age (months)
promotion; education about infantfeeding practices (breastfeeding andcomplementary feeding); and schoolfeeding programmes.If the needs of the urban poor are notaddressed, progress towards achiev-ing the Millennium Development Goals(MDGs) may be at stake, especially
Children’s rights in urban settings
21
Respiratory illnessChildren in low-income urban communities also sufferthe effects of air pollution, including respiratory infec-tions, asthma and lead poisoning. Every year, pollutedindoor air is responsible for almost 2 million deaths,almost half due to pneumonia, among children under5 years of age.28Outdoor air pollution claims aboutanother 1.3 million child and adult lives per year. InNairobi, Kenya, a 2005 study found that chronic expo-sure to pollutants in urban areas contributed to over60 per cent of all cases of respiratory disease amongchildren in these settings.29Studies in the United Statesshow that chronic exposure to high levels of air toxinsoccurs disproportionately in poor urban communitiessettled by people of minority races.30
HIV and AIDSRecent data suggest that new infections with thehuman immunodeficiency virus (HIV) among childrenare decreasing amid improvements in access to servicespreventing transmission of the virus from mother tochild during pregnancy, labour, delivery or breast-feeding. About one fourth as many new cases of HIVinfection among children are believed to have occurredin 2010 as in 2005.33Despite this progress, about1,000 babies a day were infected through mother-to-child transmission in 2010.34In addition, nearly 2,600 people aged 15–24 wereinfected every day in 2010. These infections weremainly the result of unprotected sex or unsafe injec-tion practices. In 2010, some 2.2 million adolescentsaged 10–19 were living with HIV worldwide, themajority of them unaware of their HIV status.During a critical period of transition out of child-hood, many of these adolescents were left withoutaccess to appropriate information, treatment, careor support, including age-appropriate sexual andreproductive health care and prevention services.
Vehicular traffic also poses a physical threat to children– one heightened by a lack of safe play spaces and pedes-trian infrastructure such as sidewalks and crossings. TheWorld Health Organization estimates that road trafficinjuries account for 1.3 million deaths annually31– theleading single cause of death worldwide among peopleaged 15–29, and the second for those aged 5–14.32
Figure 2 .4 . HIV is more common in urban areas and more prevalent among females
HIV prevalence among young women and men aged 15–24 in urban and rural areas in selected sub-Saharan African countries30%
25%
EM28BAFebr RGua Ory ED2012femalemalefemalemalefemalemalefemalemaleMalawiMozambiqueSwazilandZambia
Road traffic injuries
RuralUrban
20%
15%
10%
5%
0%
female
male
female
male
Lesotho
Zimbabwe
Source:Lesotho, DHS 2009; Malawi, DHS 2004; Mozambique, AIS 2009; Swaziland, DHS 2006–2007; Zambia, DHS 2007; Zimbabwe, DHS 2005–2006.Countries were selected based on availability of data.
22
THE STATE OF THE WORLD’S CHILDREN 2012
PERSPECTIVE
REACHING EVERY CHILDWiping out polio in Mumbaiby Amitabh Bachchan, UNICEF Goodwill Ambassador
For 10 years, I have been telling Indiathe life-saving message that every childshould take two drops of oral poliovaccine every time it is offered.And it is working.Today, India stands on the brink oferadicating polio – arguably the greatestpublic health achievement in its history.When the polio eradication campaignstarted, India was reporting around 500polio cases per day. Since then, morethan 4 million children have been savedfrom paralysis or death. All our hard workis paying off. But the simple truth is thatas long as polio exists anywhere in theworld, the threat will persist.
poor access to clean water, poor accessto toilets, poor breastfeeding rates andpoornutrition.Polio now is a virus of the poorest,making its final stand in the most forgot-ten places, among the most forgottenpeople. Reaching these people – theslum dwellers, the nomads, the migrants,the brick kiln workers, the families ofconstruction workers living beside theplush high-rises they build (for a dollar aday) under a sheet of plastic – is one ofthe greatest challenges in public health.The polio eradication programme isactively following a detailed ‘underservedstrategy’ to target India’s hardest-to-reach people, including those living inurban slums, in order to raise immunityamong those populations at highest risk.It is not an easy task – literally millionsof migrant families move back and forthacross the country each week, and in thetraditionally polio-endemic states of UttarPradesh and Bihar, around 750,000 chil-dren are born each month. In order toeradicate polio in India, it is essential toreach and immunize every last child. Andin the swelling slums of India’s heavingcities, every last child is hard to find.Consider Dharavi, one of the largestslums in my home town of Mumbai –home to a million people in just 3 squarekilometres. Here, poliovirus immunizationteams must follow carefully developedmicro-plan maps, walking single filealong the tiny lanes, scrambling up rick-ety ladders to reach the children livingin corrugated iron homes stacked one
on top of the other, three or four storieshigh. The immunization teams then markthose corrugated iron walls with chalk,so that the monitors who will follow in thecoming days can see which houses havebeen reached – and which children havebeen immunized. Additional teams returnto cover any children who were missed.Mumbai, India’s financial capital andhome to its film industry, is among theworld’s biggest and richest cities. It isalso believed to contain the highestproportion and largest absolute numberof slum dwellers. By some estimates,between 100 and 300 new families arriveeach day in search of work. All too often,migrant families of low socio-economicstatus find themselves in a slum. All toooften, these arrivals are never tracked,never chartered, never given a name. Alltoo often, the hardest-to-reach childrenin our country are living right underour noses.India’s polio eradication programmedemonstrates that it is possible toensure equity in the availability of healthservices in even the poorest, mostdensely populated environments. Itproves that you can find every last childin the city. And it means that in Mumbai,while the children of the slums continueto face many threats, polio need not beone of them.
I am immensely proud that independentstudies have shown that the ‘Every child,every time’ slogan is one of India’s mostrecognizable messages. I am even moreproud that Indian parents have answeredthat call. During two annual NationalImmunization Days, normally held eachJanuary and February, approximately170 million children under 5 are vacci-nated by immunization teams goingdoor-to-door to every house in the coun-try. Then, every month from March toDecember, almost all children under theage of 5 in India’s two traditionally polio-endemic states and highest-risk areasare vaccinated during polio immuniza-tion campaigns – campaigns that reach40–80 million children a year. Pause fora second to examine those numbers.Then consider what characterizes thehighest-risk areas for poliovirus transmis-sion: high-density living, poor sanitation,
Amitabh Bachchan is one of the most prominent figures in the history of Indian cinema. He has won 4 National Film Awards – 3 in the Best Actor category –and 14 Filmfare Awards. He has also worked as a playback singer, film producer and television presenter and was an elected member of the IndianParliament (1984–1987). He has been India’s polio eradication ambassador since 2002.
EM28BAFebr RGua Ory ED2012
Children’s rights in urban settings
23
HIV prevalence remains generally higher in urbanareas.35Adolescent girls and young women appear tobe at particular risk because of poverty, which drivesmany to commercial sex, and exposes them to a higherincidence of sexual exploitation and forced sex.36A 2010 review of estimates from more than 60 countriesfound that while the HIV infection rate had stabi-lized or decreased in most countries, including thoseworst affected, it had risen by more than 25 per centin seven – Armenia, Bangladesh, Georgia, Kazakhstan,Kyrgyzstan, the Philippines and Tajikistan. In thesecountries, the epidemic is concentrated among peoplewho inject drugs, people who engage in commercial sexand men who have sex with men.37Young people forma significant portion of the affected populations. InKazakhstan and the Philippines, they make up 29 and26 per cent, respectively, of all people aged 15 yearsand older living with HIV.38For most of them, infec-tion with HIV is a result of a chain of disadvantagesextending back into childhood: violence, exploita-tion, abuse and neglect – in other words, failures inprotection andcare.A 2009 study of adolescents living on the streets offour cities in Ukraine found that more than 15 per centinjected drugs, nearly half of these sharing equipment;almost 75 per cent were sexually active, most havingstarted before the age of 15; close to 17 per cent ofadolescent boys and 57 per cent of adolescent girlshad received payment for sex; and more than 10 percent of boys and over half of girls had been forced tohave sex.39Despite these clear vulnerabilities, the same
adolescents who are at greatest risk of HIV infectionare often the most likely to be excluded from services.Often, social stigma or barriers created by policies andlegislation prevent those adolescents most at risk fromobtaining preventive services.
Mental healthUrban life can also have a negative effect on themental health of children and adolescents, particu-larly if they live in poor areas and are exposed to thedangers of violence and substance abuse.40Childrenliving in urban poverty experience levels of depressionand distress that are higher than the urban average. Areview of social determinants of health in the UnitedStates concluded that children in neighbourhoods withlower socio-economic status had more behaviouraland emotional problems.41According to a number ofstudies, mental health problems experienced duringchildhood and adolescence may significantly affectgrowth and development, school performance, andpeer and family relationships, and may increase therisk of suicide.42One factor often cited by children andobservers as a cause of mental distress is the stigma thatcomes with being seen as a child of the underprivileged.Children and adolescents in urban areas are likely tohave greater access to alcohol and illegal drugs thantheir counterparts in rural areas. They may resort tothese substances as a means of coping with stress oras an outlet for idleness and frustration in the absenceof employment or opportunities for recreation such assports and youth clubs.
Figure 2 .5 . In urban areas, access to improved water and sanitation is not keeping pace with population growthWorld population gaining access to improved drinking water and sanitation relative to population increase, 1990–2008Populationgaining accessto improveddrinking waterPopulationgaining accessto improvedsanitationPopulationgrowth1,200
Rural370
Urban
0
200
Source:WHO/UNICEF Joint Monitoring Programme, 2010.
24
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED20127234501,0528131,0894006008001,000
Population (millions)
� UNICEF/NYHQ2009-1892/Josh Estey
Washing hands with soap and water at an elementary school in Aceh Besar District, Aceh Province, Indonesia.
Water, sanitation and hygiene
Article 24 of the Convention on the Rights of the Childcommits States parties to strive to ensure the high-est attainable standard of health for every child. Thisextends to providing clean drinking water and elimi-nating the dangers of environmental pollution.
Unsafe water, poor sanitation and unhygienic condi-tions claim many lives each year. An estimated 1.2million children die before the age of 5 from diarrhoea.Poor urban areas where insufficient water supplyand sanitation coverage combine with overcrowdedconditions tend to maximize the possibility of faecalcontamination.43Globally, urban dwellers enjoy better access to im-proved drinking water sources (96 per cent) than dopeople living in rural areas (78 per cent). Even so,improved drinking water coverage is barely keepingpace with urban population growth.44And access toan improved water source does not always guaranteeadequate provision. In the poorest urban districts, many
EM28BAFebr RGua Ory ED2012
people are forced to walk to collect water from otherneighbourhoods or to buy it from private vendors.45It iscommon for the urban poor to pay up to 50 times morefor a litre of water than their richer neighbours, whohave access to water mains.46Without sufficient accessto safe drinking water and an adequate water supplyfor basic hygiene, children’s health suffers. Improvingaccess remains vital to reducing child mortalityand morbidity.
The urban population as a whole has better access tosanitation than the rural population, but here, too,coverage is failing to keep up with urban populationgrowth. In consequence, the number of urban dwellerspractising open defecation increased from 140 millionto 169 million between 1990 and 2008.47The impactof this practice in densely populated urban settlementsis particularly alarming for public health. Congestedand unsanitary conditions make urban slums partic-ularly high-risk areas for communicable diseases,including cholera.
Children’s rights in urban settings
25
FOCUS ON
MAPPING URBAN DISPARITIESTO SECURE CHILD RIGHTSThe concept of mapping poverty originatedin London over a century ago as a way tohighlight differences in living standardsaccording to social class. Today’s computertechnology makes it possible to compilesimple interactive maps and correlationsto show complex information traditionallydisplayed in columns and tables.Where detailed data for a province,district or municipality may not beavailable, the ‘small area estimation’approach creates subnational estimatesbased on national census and house-hold survey information. Integrating theestimates with Geographic InformationSystems (GIS) produces maps that canshowcase differences between urbanand rural areas and within urban zones.The Columbia University Center forInternational Earth Science InformationNetwork used this method to highlightdisparities in urban income in Malawi(see Figure 2.6). The map displays gradi-ents of poverty, making possible asimple and intuitive urban-rural analysisas well as a comparison of the coun-try’s two major cities: Lilongwe, thecapital, and Blantyre, a city of compara-ble size. In this example, where darkershades denote greater poverty, Lilongweappears to have lower levels of povertythan Blantyre. Yet patterns of depriva-tion differ. While Blantyre exhibits greaterlevels of poverty than adjacent areas,Lilongwe is a relatively well-off urbancentre surrounded by poorer regions, butalso showing pockets of poverty (isolateddarker areas) within its limits. This casestudy demonstrates the variability ofurban patterns.Another example comes from theEnglish Public Health Observatories.Practitioners, policymakers and thegeneral public can use this interactiveonline tool to illustrate and analyse 32health profile indicators at the districtand local authority level. Examples of
Gathering accessible, accurate anddisaggregated data is an essential step inthe process of recognizing and improvingthe situation of children in urban areas.Innovative visual representations of infor-mation can help identify gaps, promptingaction from local decision-makers.
Figure 2 .6 . Mapping poverty in Lilongwe and Blantyre, Malawi
The shading on the map indicates levels of poverty, with darker shades denoting greater poverty. (Poverty ismeasured here by the average shortfall between actual household welfare level and the poverty line.) The blackline indicates the greater urban area.Source:Center for International Earth Science Information Network, Columbia University,Where the Poor Are:An atlas of poverty,Columbia University Press, Palisades, N.Y., 2006, p. 37 figure 5.5, based on 1997–1998,data. See <www.ciesin.columbia.edu>. Reproduced with permission.
26
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
indicators that specifically focus onchildren and young people includechildhood obesity and physical activ-ity, teenage pregnancy, breastfeeding,tooth decay, child poverty, homelessness,educational achievement, crime anddrug use (see Figure 2.7).Larger cities often encompass multi-ple local government districts, whichpermits a side-by-side comparison ofseparate administrative districts withinthe metropolitan area. Greater London isdivided into 32 boroughs. Urban dispar-ities are stark and clear: 57 per cent ofchildren in the inner London borough ofTower Hamlets live in poverty – a greaterproportion than in any other borough inEngland. The City of Westminster hasthe nation’s highest level of childhoodobesity, while Southwark has one ofthe highest rates of teenage pregnancynationwide. In contrast, the outer Londonborough of Richmond upon Thamesshows good levels of child health andwell-being, and London children overallseem to have above-average dental health.
Figure 2 .7 . Tracking health outcomes in London, United kingdomThe map on the left is shaded according to levels of deprivation. Boroughs selected for comparison appearin orange. Traffic-light colours in the table on the right indicate comparative performance in each area.
The tool also allows users to correlatevariables, such as urban deprivation,with various child health outcomes. Localgovernments and health services can usethis information to work towards reducinghealth inequalities by focusing on causesas well as results. Mapping urban indica-tors of child health and well-being revealsthat a keen focus on disparities shouldnot be limited to developing countries, aschildren’s rights and development pros-pects are uneven in some of the world’smost prosperous cities.
EM28BAFebr RGua Ory ED2012
The tool can be used to show correlation between indicators. Below, the scatter plot displays therelationship between the proportion of children living in poverty and educational achievement acrossLondon. On the top map, darker shades denote a greater proportion of children living in poverty; on thebottom, darker areas show better educational scores.
Source:English Public Health Observatories working in partnership. Sample snapshots from<www.healthprofiles.info>. Crown Copyright 2011. Reproduced with permission.
Children’s rights in urban settings
27
Figure 2 .8 . Urban income disparities also meanunequal access to waterUse of improved drinking-water sources in urban areas inselect countries in Africa (left end of the bar indicates access toimproved water among the poorest quintile of urban households;right end indicates that for the wealthiest quintile)Poorest 20%Sierra LeoneMadagascarSomaliaChadRwandaBurundiMaliDemocratic Republic of the CongoBeninGuinea-BissauZambiaNigeriaUnited Republic of TanzaniaCameroonGuineaSenegalCôte d’IvoireSwazilandTogoMalawiEthiopiaUgandaNigerCongoLesothoGambiaLiberiaNamibiaBurkina FasoZimbabwe
Richest 20%
Even where improved urban sanitation facilities exist,they are often shared by large numbers of people. Space,tenure and cost considerations limit the construc-tion of individual latrines in slums. Public facilitiesare frequently overcrowded, poorly maintained andcontaminated. Special provision for children is rare, sothose waiting to use communal toilets are often pushedaside at peak times. Girls in particular may be exposedto the danger of sexual harassment or abuse, as well asa lack of adequate privacy, especially once they havebegun menstruating.
EducationIn Article 28 of the Convention on the Rights of theChild, States parties recognize children’s right to educa-tion and commit to “achieving this right progressivelyand on the basis of equal opportunity.”Children in urban settings are generally consideredto have an educational advantage. They are better offacross a range of statistical indicators, more likely tobenefit from early childhood programmes, and morelikely to enrol in and complete primary and second-ary school.48As in other areas of social provision,however, the overall statistics can be misleading. Inreality, urban inequities profoundly undermine chil-dren’s right to education.49In urban areas blighted bypoverty, early childhood programming is often nota-ble for its absence. This is lamentable because the firstfew years have a profound and enduring effect on therest of a person’s life and, by extension, the lives of somany others.
0%
20%
40%
Use of improved drinking-water sourcesSource:MICS and DHS in African countries, 2004–2006. Countries wereselected based on availability of data.
28
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED201260%80%100%
Early childhood developmentChildren start to learn long before they enter a class-room. Learning occurs from birth, as children interactwith family and caregivers, and the foundation for alllater learning is established in the early years. Poverty,ill health, poor nutrition and a lack of stimulationduring this crucial period can undermine educationalfoundations, restricting what children are able toaccomplish. By one estimate, more than 200 millionchildren under 5 years of age in developing countriesfail to reach their potential in cognitive development.50
� UNICEF/NYHQ2008-0138/Giacomo Pirozzi
A boy works in a mechanic’s workshop in Herat, Afghanistan.
Some of the 4,000 children who attend Halit Coka Compulsory and High School, built for 1,000 students in Bathore, once a squatter settlement and nowthe largest suburb of Tirana, Albania.
Establishing good early childhood programmes inpoor urban communities is essential to supportingchildren’s survival, growth and learning. Early child-hood programmes contribute to children’s cognitive,social and emotional development and promote theirhealth, nutrition and hygiene. In addition, they canfree mothers and other female caregivers from theirtraditional roles, enabling them to participate in thepublic sphere. Yet even where such programmes exist,not all children benefit. While 25 per cent of childrenin Egypt’s urban areas attended kindergarten in 2005–2006, compared with 12 per cent in rural areas, only4 per cent of those from the poorest 20 per cent ofurban households were able to access this service.51Children from impoverished urban backgrounds havebeen found to be similarly disadvantaged in a numberof other countries.
EM28BAFebr RGua Ory ED2012
2008, 67 million primary-school-aged children werestill out of school, 53 per cent of them girls.52Primary education is generally more readily availablein urban than in rural areas but remains beyond thereach of many children growing up in poverty – espe-cially in slums, where there is often little or no publicschooling. Families often face a choice between paying
Primary educationSimilar gaps – reflecting inequalities in parental income,gender and ethnicity, among other factors – persist ingrade school, despite the progress many countries havemade in pursuing universal primary education. As of
A girl receives speech therapy in Chisinau, Republic of Moldova, as hermother looks on.
Children’s rights in urban settings
29
� UNICEF/NYHQ2011-1096/Kate Holt
Figure 2 .9 . School attendance is lower in slumsPrimary and secondary net attendance rates for urban areas in Kenya, Bangladesh, India and Ghana100%
Primary urban non-slumPrimary urban slumSecondary urban non-slumSecondary urban slum
80%
60%
40%
20%
0%Kenya (22% urban)Bangladesh (28% urban)India (30% urban)Ghana (51% urban)
Source:Kenya, DHS 2003; Bangladesh, DHS 2007; India, DHS 2005–2006; and Ghana, DHS 2003. Countries were selected for illustrative purposes.
for their children to attend overcrowded privateschools of poor quality or withdrawing their childrenfrom school altogether.
Even in countries where primary schooling is free, theancillary costs can leave people who live in poverty at adisadvantage. Students may have to purchase uniformsand classroom supplies or pay fees to take exams, andthese taken together are often expensive enough toprevent children from attending school. While parentsin Dhaka, Bangladesh, spend an average of 10 per centof household income per child on schooling costs, thisrises to 20 per cent in the poorest families. A recentsurvey of Sao Paulo, Brazil; Casablanca, Morocco;and Lagos, Nigeria, showed that families in the lowestincome quintile spent more than a quarter of house-hold income on schooling.53
Marginalized groups, including children living orworking on the street, migrant children and the chil-dren of refugees and internally displaced persons, faceparticular challenges. Until recently in China’s cities,for example, migrants who were not officially regis-tered had difficulty sending their children to school.54And all too often, children who are seen as different– because of poverty, language or gender, for example–face discrimination.Refugees and internally displaced people often live ininformal settlements in urban areas, and schools that
30
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
are already under strain may have great difficulty incoping with an influx of displaced children. Evidencesuggests that displacement severely disrupts chil-dren’s education – and again, the worst affected areoften those who were already marginalized because ofpoverty, gender, ethnic identity or other factors.55
Children from poor urban neighbourhoods are amongthe least likely to attend school. A survey in Delhi, India,found a primary school attendance rate of 54.5 percent among children living in slums in 2004–2005,compared with 90 per cent for the city as a whole.56In Bangladesh, according to 2009 data, the differenceswere even more pronounced at the secondary level:18 per cent of children in slums attended secondaryschool, compared with 53 per cent in urban areas asa whole and 48 per cent in rural areas.57Even whereprogress is made, it cannot be taken for granted.While enrolment improved in the rural and non-slum urban areas of the United Republic of Tanzania,Zambia and Zimbabwe in the late 1990s, it worsenedin urban slums.58The quality of available schooling options in poorurban areas is another issue to consider. Whiledata tend to focus on access, enrolment and reten-tion, these are linked to the perceived quality andbenefits of available education. Overcrowding and alack of appropriate facilities such as toilets are amongthe factors that undermine the quality of education.59
Creating employment opportunities for youth is vitalas well. Too many young people in urban areas seetheir improved literacy and educational achievementunrewarded with suitable jobs. Many young peoplearound the world are effectively idle – neither in schoolnor at work.
poverty, alcoholism, family dysfunction, drug abuse,sexual abuse and domestic violence increase the chil-dren’s vulnerability, and that those out of school, onthe streets or in institutions are also at greater risk.64Children lacking birth certificates or official registra-tion documents, including refugee and internally dis-placed children, can be at particular risk of traffickingand are among those most difficult for authorities totrace, much less protect. Many countries have adoptednational plans of action to combat child traffick-ing, but the lack of reliable statistical informationremains a significant obstacle – most data focus onlyon the cross-border trafficking of girls and women forsexual exploitation.
ProtectionArticle 19 of the Convention on the Rights of theChild commits States parties to “take all appropri-ate legislative, administrative, social and educationalmeasures to protect the child from all forms of phys-ical or mental violence, injury or abuse, neglect ornegligent treatment, maltreatment or exploitation,including sexual abuse, while in the care of parent(s),legal guardian(s) or any other person who has the careof the child.” Article 32 recognizes children’s right tobe protected from economic exploitation and hazard-ous work. Article 34 targets sexual exploitation andArticle 35, trafficking.
Child trafficking
At any given time, nearly 2.5 million people are inforced labour as a result of trafficking – 22 to 50 percent of them children.60Child trafficking is frequentlyhidden, denied or ignored, making comprehensive datadifficult to obtain. Some forms take place mainly inurban areas: trafficking for sex work, for example, andtrafficking that targets children who live or work oncity streets.
Many children are trafficked from rural to urban areas.A 2001 study of sexually exploited girls aged 9–17 inmajor cities of the United Republic of Tanzania foundthat many had been trafficked from the country’s inte-rior. Some had been recruited as domestic workers andabused within their employers’ homes; others weretrafficked directly into prostitution or recruited intoit by peers.61One study indicates that most traffickedgirls are put to work as sex workers, for example, inthe major Indian cities of Mumbai, Delhi and Kolkata.In Bangladeshi cities, large numbers of girls and boysare exploited in street sex markets and brothels.62In Eastern Europe, children aged 13–18 are particu-larly at risk of being trafficked.63Evidence suggests that
EM28BAFebr RGua Ory ED2012
A five-year-old girl sells goods to commuters on a train in Buenos Aires,Argentina. She has been working in the city’s mass transit system sellinghairpins and other products since she was 3 years old.
Children’s rights in urban settings
31
� UNICEF/NYHQ2011-0219/Sebastian Rich
A boy works in a mechanic’s workshop in Herat, Afghanistan.
Child labour
Even in the absence of trafficking, many children areforced to work in order to survive. Around the world,an estimated 215 million boys and girls aged 5–17were engaged in child labour in 2008, 115 million ofthem in hazardous work.65Children may work as ragpickers or shoeshiners, serveat tea stalls, sell cigarettes on the street, or work inhomes or factories. Many of those engaged in childlabour experience its worst forms – including forcedand bonded work, illicit activities, armed combatand domestic labour. Because they are largely invisi-ble, these forms of child labour are the most difficultto tackle.
Child domestic labour is predominantly an urbanphenomenon; children who work in rural areas tendto be involved in agricultural work as unpaid familymembers. Domestic workers, most of them girls, areisolated and subject to the whims and arbitrary disci-pline of their employers, from whom they may sufferabuse. Sexual abuse is frequent but seldom prosecuted.
32
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
Child domestic workers can also suffer from psycho-logical problems. Research in Kenya, for example,found that they were more likely than other childrento experience insomnia, bed-wetting and depression,among other conditions.66
Children living and workingon the streetsEstimates suggest that tens of millions of children liveor work on the streets of the world’s towns and cities– and the number is rising with global populationgrowth, migration and increasing urbanization.Children resort to living and working on the streetfor many reasons. Violence or abuse at home or inthe neighbourhood drives many away, as studies haveshown in cities as diverse as Dhaka, Bangladesh, andMoscow, Russian Federation.67Poverty also plays apart. While abuse, conflict or neglect can happen in anyfamily home, children whose poverty and marginaliza-tion leave them with few choices often see the street asthe best available option for escape.68
� UNICEF/NYHQ2007-1166/Shehzad Noorani
Living on the street exposes children to violence,yet crimes against them are rarely investigated, andfew people are prepared to act in their defence. Onthe contrary, in the many countries and cities wherevagrancy and running away from home are outlawed,children living or working on the street are often theprimary victims of such criminalization. Researchers,national bodies and international human rightsgroups have reported that police and security forceshave abused children on the streets of cities all overthe world.Children’s gender, age, ethnicity and disability statusinfluence the extent and type of violence they experi-ence and the coping mechanisms they develop. A 2000study of children on the streets of Brazil’s cities showed
that boys were more likely than girls to go hungryand to experience physical violence at the hands ofthe police. Girls were less likely to beg for money andmore likely to sleep in institutions rather than on thestreet.69Another study conducted that year indicatedthat girls more frequently internalize violence and areat greater risk of continuous abuse.70The problems outlined in this chapter constitute anunconscionable assault on the rights of children. Thefollowing chapters examine more closely some of thechallenges and opportunities that children face incities, and discuss initiatives that seek to improve lifefor children in an increasingly urban world.
The Millennium Development goalsThe eight Millennium Development Goals (MDGs) covera spectrum of issues, from poverty and hunger to educa-tion, child survival and maternal health, gender equality,combating HIV/AIDS and building a global partnership fordevelopment. Progress towards achieving the goals ismeasured against 21 specific targets.
MDG 7 contains the commitment to ensure environmentalstability. One of its urban facets, Target 11, aims to haveachieved a significant improvement in the lives of at least100 million slum dwellers by 2020. This is also known asthe ‘Cities without Slums’ initiative. In addition to envi-ronmental concerns and a specific focus on urban slums,MDG 7 also contains a commitment to halve, by 2015, theproportion of people without sustainable access to safedrinking water and basic sanitation.Although one of the targets of MDG 7 is dedicatedspecifically to slum dwellers, the goals should be seenas a continuum of development priorities. The lives ofpeople in the world’s slums cannot improve substantially
EM28BAFebr RGua Ory ED2012
without concerted action to eradicate poverty andhunger (MDG1); achieve universal primary education(MDG 2); promote gender equality and empower women(MDG 3); reduce child mortality (MDG 4); improve mater-nal health (MDG 5); combat HIV/AIDS (MDG 6); or createa global partnership for development (MDG 8).Evidence suggests that national approaches to slums areimproving as countries move away from negative policiessuch as neglect, forced eviction or involuntary resettle-ment towards more positive tactics such as communityengagement, slum upgrading and rights-based policies.Nevertheless, the number of slum dwellers worldwidehas increased by 60 million since Target 11 was estab-lished in 2000.Slums are the physical manifestation of the urbanizationof poverty. Growing numbers of urban dwellers are poor,and inequality in the urban sphere shows no signs ofabating. Future international targets will have to take intoaccount the expanding scale of the problem.
Children’s rights in urban settings
33
CHAPTER
3
EM28BAFebr RGua Ory ED2012� UNICEF/NYHQ2007-2316/Michael Kamber
UrbanchallengesThis chapter examines some of the phenomena shapingthe lives of children in urban areas, from their reasonsfor moving to the city and their experience of migrationto the challenges of getting by in the face of economicshocks, violence and disasters.
Migrant children
It has long seemed as if cities had a magical power todraw people in with bright lights and the promise ofadvancement. Images of people moving from rural tourban areas endure in the collective imagination, andmigration continues to play an important role in manyregions. Rural-to-urban migration is pronounced inWest Africa,1for instance, and international migra-tion remains a major factor in Europe, Asia andNorth America.2Historically, access to resources in urban areas hasnot been equitable. Every place has its own pattern ofvulnerability, stemming from accumulated and currentpolitical and social prejudices.3New arrivals may bepushed to the margins of urban society; this may be a
EM28BAFebr RGua Ory ED2012
deliberate response intended to deter future migra-tion. Migrants, especially those without documents,may be denied public services, social protection andeven emergency health care. Institutionalized exclu-sion can take the form of registration requirementsfor migrant workers – an ostensible means of proffer-ing services that, in practice, often serves the oppositepurpose. Rather than making such essentials as school-ing available to migrant families, these requirementsoften have the effect of denying such services to thosenot registered,4especially where the process or cost ofregistration is prohibitive.
Most child migrants move with their families,5accom-panying parents or caregivers seeking employment oropportunity. Almost a tenth of China’s child popula-tion, or 27.3 million children, took part in internalmigration with their parents in 2008.6A significantnumber of children and young people, however, movewithin countries on their own.7A recent analysis ofcensus and household data from 12 countries foundthat one in five migrant children aged 12–14 and halfof those aged 15–17 had moved without a parent.8
Urban challenges
35
Queuing for food at a camp for people displaced by the 2008 earthquake in the city of Mianyang, Sichuan Province, China.
Children and young people frequently follow establishedpatterns of migration. In West Africa and South Asia,where rates of independent child migration are partic-ularly high,9most child migrants leave home betweenthe ages of 13 and 17. Many of these children growup in impoverished rural areas where it is commonto travel to seek work in order to supplement familyincome, whether for part of each year, during leanperiods or for longer durations.10At least 4 millionchildren are thought to migrate seasonally, whether bythemselves or with their families, in India alone.11
Like adults, children migrate in response to a combi-nation of push and pull factors. For many, migrationis an attempt to secure a better life, whether in termsof economic or educational opportunities, or simply toescape poverty. Others relocate because of family circum-stances, such as the loss of a parent, or to escape conflictor natural disasters and the upheaval and food shortagesthat accompany them. An unstable or difficult familyenvironment often plays a role. Children may be forcedto leave owing to neglect or abuse from their caregivers.And in some cases, leaving is a way of marking out a
36
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
separate identity – effectively declaring independence.12Be it forced or voluntary, with adult caregivers or alone,migration entails risks that require age-appropriatemeasures to protect the children involved.Once in the city, children who moved to help theirfamilies can find that participation in the urbaneconomy weakens the bonds between them and theirparents.13Indeed, the act of leaving home may evenbe seen as an abandonment of family duties and thusmay cause conflict with parents. And all too often,young people who arrive in urban centres with hopesof educational advancement find it unattainablebecause of work commitments, as separate studies inBangladesh and Ghana have confirmed.14The quality of schooling also can be a cause forconcern. In Turkey as elsewhere, schools in poor quar-ters and on the urban periphery, where most migrantssettle, struggle with overcrowding and a lack ofresources. To this is added the challenge of accommo-dating an influx of students from diverse cultures whospeak differentlanguages.15
� UNICEF/NYHQ2008-0453/Adam Dean
PERSPECTIVE
A WORLD APARTby Eugen Crai, Country Director,Roma Education Fund, Romania
The isolation of Roma children
Romania, home to more than half amillion Roma according to the latest offi-cial data (other estimates run as high as2.8 million), illustrates the difficulties andopportunities involved in efforts to elimi-nate disparities and promote inclusion. In2001, the Government adopted a nationalstrategy to improve the situation of Romathroughout the country. Ten years on, only13 per cent of local governments haveimplemented specific measures for Romacommunities. Progress towards socialinclusion has been slow from the outsetand was further hampered by the globaleconomic crisis, which hit the region in2008. Many municipalities have cut socialspending amid rising unemployment.Poverty affects Roma communities inboth urban and rural Romania; the poor-est are clustered mainly in mid-size
Eugen Crai is the country director of the Roma Education Fund in Bucharest, Romania. He holds a master’s degree in law from McGill University, Canada,and specializes in human rights law and anti-discrimination legislation, as well as minority rights advocacy and education policy. His professional careercentres on Roma communities – over the past 14 years he has worked on the first European Union Phare Project for the Improvement of the Roma Situationin Romania and has also served as education officer and social policy specialist at UNICEF Romania.
EM28BAFebr RGua Ory ED2012What is life like for a child in a Bucharestghetto? Consider the case of Laurentiu,a 16-year-old in the Ferentari district,known for its large Roma population,its derelict buildings, its poverty andlarge numbers of children out of school.After Laurentiu’s father died, his motherabandoned him, and he was placed ina state institution. He now lives withhis 70-year-old grandmother and hisfive brothers in an apartment that hasbeen disconnected from water and gas
In 2005, governments in Central andEastern Europe proclaimed the RomaDecade of Inclusion and committedthemselves to “eliminating discrimina-tion and closing the unacceptable gapsbetween Roma [people] and the rest ofsociety.” With the clock running downto the Decade’s conclusion in 2015, thiseffort to right historical inequalities insuch key areas as education, genderand health has brought modest results.Roma children continue to have substan-tially lower vaccination coverage, withappalling consequences. When Bulgariaexperienced an outbreak of measles in2009, 90 per cent of all cases occurredamong the ethnic Roma community.
towns and larger villages. What sets thesituation in urban settings apart, hereas in the wider region, is the separationof Roma from the rest of the municipalpopulation, with the Roma populationliving in de facto ‘ghettos’. The problemof ‘ghettoization’ is a clear physical mani-festation of exclusion. Its roots date backto the mid-1800s, when laws were passedfreeing Roma from centuries of slavery.Without any policies to promote and easeintegration, freed Roma settled at themargins of urban areas – essentially, onno man’s land. Through my work I haveseen that Roma communities continueto be excluded from the developmentplans of cities that have expanded andencircled their neighbourhoods. Romacommunities remain isolated – manyare not connected to public utilities.The absence of permanent housing,combined with a lack of birth or identitydocuments, can significantly limit accessto health care, education and employ-ment. Evictions frequently occur withoutwarning, reinforcing thissegregation.
because the family struggled to pay thebills. Growing up in a damp space, with-out gas to cook food or water to wash,just a few blocks away from the glossycommercial boulevards of Bucharest– this is the brutal reality of two neigh-bouring worlds.Urban poverty is especially difficult forchildren, who have little control overtheir surroundings or level ofaffluence.Many find it impossible to attend school,and those who do attend struggle to dowell with limited support. Roma childrenin Romania have much lower enrolmentrates at all levels of education, startingwith preschool; many are unnecessar-ily placed in special education. In 2005,only 46 per cent of the Roma popula-tion aged 12 and above had spent morethan four years in school (compared with83 per cent of the general population),and of those only 13per cent acquired atleast some secondary education (63percent among the general population).The lucky ones find non-governmentalorganizations that provide counselling,tutoring, homework help and a spacein which children can discuss prob-lems, gain confidence and improve theirmarks, often in preparation for the crucial8thgrade final exam, a stepping stoneto high school or vocational studies. TheRoma Education Fund is one organizationworking to make a difference in the livesof some 5,000Roma children and youth inRomania. But there are so many more likeLaurentiu. So much remains to be done.
Urban challenges
37
Agents, not victimsChildren play no part in creating social hierarchies,classes or castes. They are born into deeply unequalsocieties and live out their lives hampered (and, occa-sionally, aided) by societal perceptions, conventions andstereotypes. It is easy, therefore, to regard them simply asvictims of forces beyond their control. But consider theirmotives and actions as migrants, and it becomes appar-ent that children also act as agents of their own destiny.A teenager’s decision to migrate or seek work may be anempowering experience – an attempt to reach objectives orassert independence. Indeed, for all the dangers and diffi-culties children face, studies suggest that most perceivetheir migration as having been positive – even when theiractual experiences have been negative. Many see migrationas a step towards taking material responsibility for them-selves and as an opportunity for superior education.Work, too, can have an empowering effect, particularlyif it provides vital resources for survival. While childlabour is too often premature, exploitative, dangerousand abusive, it is important to recognize that, especiallyfor older children, appropriate work can make a signifi-cant contribution to development by building self-esteem,teaching skills and helping children cope with poverty.The Convention on the Rights of the Child recognizes thatchildren should have increasing autonomy, in line withtheir evolving capacities.
Children who migrate unaccompanied by adults areparticularly vulnerable to exploitation, abuse and traf-ficking.16Without support and protection networks,they may have particular difficulty coping emotion-ally. Similar predations may await children who are,or who move with, refugees or internally displacedpersons fleeing conflict or environmental distress.More than half the world’s registered refugees live inurban areas.17Some have official status, but many more
� UNICEF/NYHQ2011-0015/Frederic Sautereau
An unaccompanied girl, aged 6, in the town of Loguatuo, Nimba County,Liberia, where she is staying with a Liberian family. She fled her home inCôte d’Ivoire following violence after the 2010 presidential election.
38
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
lack the legal right to urban residence and may there-fore be excluded from assistance. Women and childrenamong these urban refugees and asylum seekers are atrisk of harassment, exploitation, human trafficking andgender-based violence.18Refugee and asylum-seekingchildren and adolescents, particularly those unaccom-panied by adults, are especially vulnerable during theresettlement phase.19Children born to migrant parentsmay end up stateless and unable to enjoy the rights ofcitizenship. Internally displaced persons may find them-selves without economic resources and may be seen ascompeting with the urban poor for social services. Forhost communities, national governments and the inter-national community, providing effective assistance isparticularly challenging in such scenarios.Children are affected by migration to cities even whenthey do not move. Many are left behind in rural areas inthe care of a parent, relatives or community members.Such was the case with 55 million children in China in2008. Being left behind can cause physical, educationaland psychosocial distress.20The damage is not inevita-ble, however. A 1998 study of primary school childrenof Filipino migrants suggests that, with sufficient carefrom the extended family, migration on the part ofparents need not prove detrimental to child develop-ment, particularly when childcare training, counsellingand other forms of support are provided.21
FOCUS ON
HELPFUL STRATEGIESIN URBAN EMERGENCIESInformation on slum communities isoften inadequate, outdated or nonexis-tent, making it difficult to locate the mostvulnerable and those in greatest need.But solutions are at hand. In Nairobi,impoverished communities identifyat-risk families and pass this informationon to humanitarian agencies so theycan pinpoint those most likely to needemergency assistance.In Nairobi and Manila, cash-transferdelivery systems have helped recipi-ents regain a measure of food securityand restart their livelihoods. Communitycommittees identified the most vulner-able, agencies verified this information,and then SIM cards were distributed,allowing beneficiaries to get cash viamobile phones.immediately after crisis has struck, whenthe whole affected population needsassistance. Community drop-in centresproviding information, services andprotection can also prove helpful.Scant water and sanitation infrastruc-ture is a major challenge in poor urbansettings – even more so when disas-ter pushes large numbers of peopleinto these areas. The results of such asurge in users can include the contami-nation of drinking water. Sanitary toiletsystems consisting of commodes thatcan be emptied at designated wastedisposal points are being introduced inthe slums of Nairobi. Another innovation,the ‘peepoo’ bag, is biodegradable andcan be used as compost in gardens, soit does not add to the pressures on localsewage infrastructure. In Manila, raisedtoilets have been built to withstand flood-ing. The key to success in each of thesecases has been community involvementin the design and implementationof initiatives.In Port-au-Prince after the 2010 earthquakeand elsewhere, ‘child-friendly spaces’were established to address children’spsychological and social needs – and tohelp protect children from the increasedrisk of violence, abuse and exploitationthat accompanies emergencies. A partic-ular emphasis was placed on serving thesurvivors of gender-based violence.
All children are vulnerable in emergencies,but certain realities place those living inpoor urban areas at special risk.First, epidemics spread fastest incrowded places lacking health servicesand sanitation facilities. Second, violenceby armed groups, gangs, crime syndi-cates, rebels or government forcesspawns instability and insecurity. Thiscan be felt most acutely by children andwomen, who are also at risk of gender-based violence. Third, conflict or naturaldisasters in rural areas can lead to amassive influx of internally displacedpersons into urban areas, with largenumbers seeking refuge not in campsbut in host communities where the infra-structure and services are alreadyweak. This puts both host families anddisplaced people under extreme strainand leaves them more vulnerable toepidemics or urban violence. And fourth,pre-existing deprivations such as inade-quate shelter and limited access to cleanwater, sanitation, education and healthcare mean that delivery systems mustbe created before humanitarian aid canreach people.
When emergencies occur inmarginalizedurban areas, national and internationalagencies face threats to children’shealth, safety and well-being. But inno-vative responses tried in Port-au-Prince,Haiti; Nairobi, Kenya; and Manila,Philippines, haveproved successfuland could be applied elsewhere.
EM28BAFebr RGua Ory ED2012Also in Manila, an early warning surveil-lance system introduced in May 2010entails training health workers to reportthe incidence of disease by sending textmessages to computer hubs.It can be more difficult to identifybeneficiaries in cities where rich andpoor live shoulder-to-shoulder thanin those where the poor live in largeand distinct settlements. Some groups– undocumented immigrants, for exam-ple – may prefer not to be identified forfear this will bring on politically moti-vated violence, arrest or expulsion.Blanket targeting can overcome theseconstraints but it is only appropriate
Source:UNICEF Office of Emergency Programmes.
Urban challenges
39
Economic shocksThe effects of the economic crisis unleashed in thefinancial capitals of high-income countries in 2007continue to be felt around the world in high unem-ployment, deteriorating work conditions, dwindlingreal incomes, and food and fuel prices that are highand difficult to predict.Globally, there were 30 million more unemployedpeople in late 2010 than before the crisis broke, andthe number continued to grow in 2011.22The burdenis disproportionately borne by workers aged 15–24,whose unemployment rate rose from 11.8 per cent in2007 to 12.6 per cent in 2010.23Studies of previouseconomic downturns suggest that this generation ofyoung people could end up detached and disillusioned,with long-term repercussions for their personal andcollective well-being.24Unemployment figures for urban youth are hard toobtain, but those that are available paint a worryingpicture. Young people in Sierra Leone’s urban areasare more likely to be unemployed than either ruralyouth or urban adults.25In low-income countries, the
statistical evidence on youth unemployment tends tobe weak, partly because a significant proportion ofyoung people work outside the formal sector. Thereare indications, however, that the crisis has swelledthe ranks of the ‘working poor’ – a category in whichyoung people are overrepresented26– and slowed prog-ress in poverty reduction, education and health care.27In extreme cases, persistent unemployment can contri-bute to civil unrest. Urban areas tend to be the focus ofsuch turmoil, as the high concentrations of people makeit easier to reach critical mass. Potential or actual civildisturbance is a concern in many cities of West Africa,where the movement of young people from rural areasto cities has reached extremely high levels28and jobgrowth has been insufficient to absorb the influx.29In North Africa and the Middle East, young people frus-trated by a lack of economic opportunity accountedfor a significant proportion of demonstrators in thewave of protests that spread across the region inthe spring of 2011, following the self-immolationof a young graduate in Tunisia in December 2010.
EM28BAFebr RGua Ory ED2012
Residents of a neighbourhood in Manila, Philippines, contend with mud and stagnant water in the aftermath of floods caused by Tropical Storm Ketsana.
40
THE STATE OF THE WORLD’S CHILDREN 2012
� UNICEF/NYHQ2009-1449/Peter Wurzel
FOCUS ON
WOMEN, CHILDREN,DISASTER AND RESILIENCEsearching for missing or unaccompaniedchildren in Manila and its surroundingareas recorded 47 child deaths and257 children aged 6–18 who were sepa-rated from their families, missing or inneed of other assistance. Several chil-dren had drowned. Others succumbedto hunger, diarrhoea, dengue andrespiratory diseases.Young people showed resilience andcreativity. As long as their cell phonesremained intact, SMS networks couldtrack the locations of stranded neigh-bours and guide rescuers there.Fashioning makeshift boats out of what-ever floated, including a refrigerator withno door, they ferried people to safety.They helped clear mounds of mud andhauled away accumulated debris, someof which they sold as scrap. Many hadto drop out of school in order to work tosupport their families.Disruptions of household earnings inan already poor population seriouslyaffected the health and well-being ofchildren. Hard-pressed even before theflood, parents were forced to cut downon servings of food and stretch whatlittle they had over several meals.Better-off women shared their food withthe less fortunate and offered to lookafter children while mothers searchedfor work, money or relief goods. Motherstold heartbreaking tales of their chil-dren clinging hysterically to them formonths afterwards if they attempted toleavethehouse.Women showed strong leadership,especially in the recovery and recon-struction phases. By avidly helpingothers, organizing community responses,finding ways of earning, and demand-ing that local officials improve disastermanagement programmes, they graduallybrought the populace back to the famil-iar routines of pre-Ondoy life. Togetherwith the men, they protested or resistedattempts to relocate them to distant sites,arguing that with few earning opportunitiesthere, their children would starve.In 2011, new legislation was passed toprepare for future calamities related toclimate change. Disaster managementprogrammes were strengthened. So,when Typhoon Falcon brought compara-ble flooding to the metropolitan region,Marikina City ordered evacuations andmarshalled rescue and relief assistancein good time. Muntinlupa City reapedthe benefits of its ban on plastic bags.Its clear waterways facilitated drainage.The full benefit of these efforts willmaterialize too late for the childrenlost to or traumatized by Ondoy. Butimproved community data on who andwhere the children are, coupled withtraining of local officials and commu-nity members in more efficient reliefdistribution and rebuilding based oncommunity strengths, offer hope to thenext generation.
Early on 26 September 2009, TropicalStorm Ketsana, locally named Ondoy,struck Manila and resulted in the worstfloods in 50 years. It was followed a weeklater by Typhoon Parma, known locally asPepeng. Especially affected were an esti-mated 220,000families in the pooresturban neighbourhoods whose flimsyshelters had stood along waterwaysand in low-lying areas. Such families areaccustomed to dealing with typhoons.Early warnings find them hoisting theirhousehold items up to the rafters andtaking children to stay with relativesor friends on higher ground. Ondoy,however, took everyone by surprise.A post-disaster needs assessmentconcluded that Ondoy and Pepengdirectly affected some 9.3 million people.Nearly 1,000 deaths were registered. Thenumber of children or women who diedor were injured is not known becausedata were not disaggregated by age orgender. However, a special field team
EM28BAFebr RGua Ory ED2012
The Philippines is one of the 12 countriesin the world most vulnerable to disastersand climate change. From 1980 to 2009,some 33,000 people died and another 109million were affected by natural calam-ities. The nation’s vulnerability stemslargely from the 60 per cent of its 1,500municipalities and 120 cities locatedalong coastal shores. Many of them,like Metropolitan Manila with its popu-lation of 11 million, include areas belowsea level. Disasters loom large over thecountry’s future as the weather becomesincreasingly severe and unpredictable.
by Mary RacelisResearch Scientist, Institute of Philippine Culture, andProfessor, Department of Sociology and Anthropology,Ateneo de Manila University, Manila, Philippines.
Disparities affecting children in urban areasUrban challenges
4141
Violence and crime
Crime and violence affect hundreds of millions ofchildren in urban areas. Some are targets and othersparticipate in or witness such acts as assault, mugging,communal conflict and murder.
Armed conflict and children in urban areasSince Gra§a Machel’s landmarkImpact of ArmedConflict on Childrenreport was published in 1996, theinternational community has focused increasingly on thissubject of grave concern. Millions of children have beenkilled, injured, orphaned or separated from their fami-lies. Millions more have been deprived of schooling inIraq, Pakistan and other countries embroiled in armedconflict. Often, the deprivation has been worst in cities.In Tajikistan, for example, researchers have found thatprimary school enrolment rates remained lower inurban areas than in the countryside foryears afterthe 1992–1998 conflict.Although armed conflict is distinct from the quotidianviolence of gangs and organized criminal activity, thetwo increasingly overlap. To secure resources, armedgroups may become involved with criminal traffickingnetworks, as is the case with the drug trade in Colombia
42
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
The poor are also especially vulnerable to risingfood and fuel prices because they already spend50–80per cent of their money on food, leaving little formedicines, education, transport or cooking fuel. Thesefamilies can ill afford to pay more, yet their purchasingpower is further eroded by declining incomes, reducedpublic spending and shrinking remittances from familymembers working overseas.31Governments have anobligation to protect the poorest and most vulnerablechildren from the adverse effects of economic crises.
Brothers, aged 3–9, stand in the burnt-out ruins of their home, where theycontinue to live with their parents following ethnic violence in the city ofJalal-Abad, Kyrgyzstan, June 2010.
In addition to the obvious direct harm they cause,crime and violence can undermine children’s faithin adults and the social order. Chronic exposure canimpede children’s development and has been related topoor academic performance and higher school drop-out rates, anxiety, depression, aggression and problemswith self-control.32
and Afghanistan and trafficking in rare minerals in theDemocratic Republic of the Congo. Urban gangs, mostoften composed of young men, can morph into militias, aswas the case with the West Side Boys, who were tacti-cally employed by combatants in Sierra Leone’s civil warof 1991–2002.While armed conflict is not exclusive to urban areas, it isclear that an attack on a densely populated city neigh-bourhood – whether by government forces, rebel militiasor terrorists – maximizes casualties, including among chil-dren. In some cases, civilians are deliberately targetedin order to create a greater political impact – as withexplosive devices detonated in busy urban areas such asmarkets. In other cases, combatants claim that broaderwar aims justify the costs of civilian death or injury. Allassaults on civilians, however, and especially those onchildren, are violations of international human rights law.
� UNICEF/NYHQ2010-1241/Cliff Volpe
Unemployment in the region is particularly high amongbetter-educated, mostly urban, young people. Thesupply of skilled jobs has simply not matched demandfor them. The opposite is true of the member coun-tries of the Organisation for Economic Co-operationand Development (OECD), where unemployment ishighest among the least educated.30
PERSPECTIVE
SPEAkING FOROURSELVESby the ATD Fourth World MovementYouthGroup, New York City
In the neighbourhoods where we aregrowing up, we see the rougher side ofthis famous city. Poverty is part of life inour overcrowded and under-resourcedcommunities. Peer pressure influenceskids to drop out of school, and many endup in jail or dead. The face of poverty mightchange from one place to the next, but howpoverty is felt is the same. It connects uswith young people from other cities.
We live in different parts of the city, but wehave had the common experience of shar-ing in street libraries. These are outdoorlibraries, set up on blankets by volunteerswho bring books and arts to our neigh-bourhoods. The libraries are places ofpeace where young people and childrencan work together and support each other.They are important because violence is amajor part of our lives. We have had to runaway from family barbecues when shoot-outs began, and we have teachers whohave stopped even trying to break up fightsin class because they’re so common.Gangs are one of the worst problemsfacing our communities. Gangs affect theentire neighbourhood, causing outbursts
This essay was contributed by Crystal Dantzler (aged 17), Najayah Foote (13), Tatyana Foote (13), Jammie Hatcher (11), Brianna Jeanniton (15), JadoraLindsey (18), Malcom Smith (14), Shakora Townsend (15) and the young people of All Together in Dignity (ATD) Fourth World Movement, New York City.
EM28BAFebr RGua Ory ED2012Violence is serious in poor communi-ties; it creates a cycle that keeps peoplein poverty. But extreme poverty is a formof violence itself, because it forces chil-dren and families to use so much of theirenergy to defend their rights againstsuch threats as eviction and gentrifica-tion, which cause rents to rise and forcepoorer families to move frequently. As aresult, many of us have had to move tocompletely different neighbourhoods andschools. These kinds of transitions arealways scary and challenging, but in thecity, they are common and can be down-right dangerous for us. When you’re newto a neighbourhood or school, people
People all over the world hear stories,watch movies and see postcards of NewYork City. They recognize our skyline – theEmpire State Building, the Statue of Libertyor the Brooklyn Bridge – on sight. But NewYork City is not just about the big lights, thebig buildings. There are the streets, andthen there are the people who walk them,and when you live here you learn thatNew York is just like any city, filled withpeople who struggle to make ends meet.
of violence and retaliation in our parksand influencing every decision we make,down to when and where we buy grocer-ies, so that we can have a better chanceof avoiding confrontation. We’ve seenenough to know that once you’re in agang, you’re done. There is a good chancethat you’ll have to die to get back out.Young people feel a common pressure togain respect and a sense of belonging,but overcrowded living conditions andconstant changes in our lives can makeaccomplishing that impossible. Gangsgive a kind of power and protection, andthis creates a lot of pressure to join. It’strue that you can get respect for doingsomething you’re good at, but if you livein an under-resourced neighbourhood theopportunities and support you need to gettruly good at something don’t come sooften. The fact that people believe join-ing a gang is their best option shows howdeeply problems run here.
want to test you. If you fail those tests,you’re a target. Kids who don’t fit in getteased, harassed and even attacked. Asour 17-year-old peer Crystal told a UnitedNations panel in 2011, she was attackedby seven girls on her way to a bus stopbecause she was wearing brand-nameclothes popular at the school from whichshe had just moved, but shunned at hernew school.We’ve all had these kinds of experiences,but we have learned how to handle themand move forward.Young people like us have a role to play.Even in difficult neighbourhoods there arethe positive influences of strong fami-lies and inspiring people, and we havethe power to seek out those positive rolemodels and to become them ourselves.All of us want to be those people, and wewant a chance tochange the communi-ties we grew up in for the better. By livingthrough so many of the injustices associ-ated with growing up in under-resourcedneighbourhoods, we’ve gained the knowl-edge we need to start the process ofchange, change that will create placeswhere all families are treated withrespect and dignity.Speaking out about our lives is part ofhow we can create that change. Peoplecan’t speak for us who have never livedthe lives we describe. But when we getto speak on behalf of our own experi-ences and ourselves, that’s freedom ofspeech, and that’s a positive step.
Urban challenges
43
A boy pushes a cart in the flooded city of Hyderabad, Sindh Province, Pakistan.
The causes of violence affecting children in urban areasare many and complex, but prominent among themare poverty and inequality. The insufficient provisionof public services and such community infrastruc-ture as schools and recreational areas is common tothe cities of low-income countries and those in high-income countries whose governments are prone tosocial austerity. High rates of crime and violence oftenprevail in such places. The experience of being deprivedof something to which one believes one is entitled trig-gers a sense of exclusion and can lead to frustrationand violence. A study of 24 of the world’s 50 wealth-iest countries confirmed that more unequal societiesare more likely to experience problems associated withthis kind of relative deprivation: high rates of crime,violence and imprisonment.33Incarceration is itself aproblem because violence is common in prisons anddetention centres.In many parts of the world, urban gangs made upentirely or partly of young people are known forcommitting such crimes as extortion, petty theft,selling or trafficking drugs, armed robbery, murderand carjacking.
44
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
On average, children join gangs around age 13, butevidence suggests a trend towards earlier enlistment.34In marginal urban settings, gangs can offer children asense of identity, belonging and protection, as well asfinancial reward. Children from poor backgrounds,often growing up with few opportunities to escapeunemployment, may see little prospect of securing theirown future or supporting their families. They dropout of school, disillusioned with its lack of potentialto improve their situation. In urban areas where thestate fails to provide such essentials as safe water, elec-tricity or gas, health care, housing, education or legalprotection, gangs sometimes step in to fill the vacuum.35While it is difficult to measure the impact of specificinstitutional approaches to the challenge of reducingviolence, evidence suggests that community policingprogrammes – which include community participationand special training for police personnel – have provedsuccessful in urban areas of Brazil, Colombia, CostaRica and Guatemala.36Successful strategies to prevent violence involve alllevels of the community and serve to establish trust
� UNICEF/NYHQ2011-1402/Warrick Page
between them, creating ties among children, adults,schools, institutions, civil society and local and nationalgovernments.37The ideal protection, albeit one thatis unattainable for many children, is a stable familyunit, characterized by strong bonds between childrenand parents and non-violent forms of discipline. Suchsettings help insulate children from a violent urbanreality and enable them to better recover from psycho-logical distress if they do suffer violence.38
among young children in particular. Warmer temper-atures are expanding the endemic areas of malaria,dengue fever and other vector-borne diseases – forinstance, into the East African Highlands.44Children,along with the elderly, are also at highest risk of harmfrom heat stress, especially in urban ‘heat islands’.A 2003 study in Sao Paulo found that for every degreeof increase in temperature above 20� C, there was a2.6 per cent increase in mortality among childrenunder 15.45Disasters take a particular toll on underprivilegedurban residents because of where they live, and alsobecause they are inadequately served and ill-equippedto prepare for or recover from extreme events. Thepoorest urban populations and their children maketheir homes wherever they can find land or afford rentwithin reach of work: often in congested slums or infor-mal settlements on flood plains or steep slopes, underbridges or on sites close to industrial waste. Childrenare at high risk in such locations, as they seldomhave access to information or the protective infra-structure – storm drains, sewer systems, sea walls orpaved roads – that can help people withstand extremeevents. Homes are often built from flimsy materialsthat cannot stand up to high winds, mudslides, rushingwater or earthquakes.� UNICEF/NYHQ2011-0140/Graeme Williams
Disaster riskFor millions of children, urban poverty is complicatedand intensified by exposure to hazards such ascyclones, floods, mudslides and earthquakes. Whencombined with acute vunerability, these hazards canbecome disasters. While large-scale events are majorenough to qualify as disasters, others, far more numer-ous and ultimately affecting many more children andfamilies, are too minor or too slow-moving to meet theformal criteria for ‘disaster’.39But they are still signifi-cant enough to turn lives upside down, bringing intenserainfalls that flood homes and destroy possessions,prolonged droughts that exhaust an already unreliablesupply of water, or heat waves that turn unventilatedshacks into ovens.Since the middle of the twentieth century, recordeddisasters have increased tenfold, with the major-ity stemming from weather-related hazards.40Evenconservative models predict more extreme weather –heavier rainfall, stronger windstorms and more intenseheat waves – adding to the existing burden of disaster.41Vulnerable locations and the great and generally in-creasing concentrations of people and enterprises canmake cities especially dangerous. The proximity ofresidential and industrial areas, the lack of space forevacuation, poor drainage, the potential for the rapidspread of communicable disease due to high populationdensity – all of these factors can intensify disaster risk.42In the face of a disaster, children are among the mostsusceptible to injury and death. Over three quartersof casualties in recent decades have been children insub-Saharan Africa or South Asia.43Droughts, flood-ing and post-disaster conditions all intensify the riskof, for example, sanitation-related illnesses and schooldropout, especially in congested urban areas and
EM28BAFebr RGua Ory ED2012
A boy stands near a rubbish-strewn gully on the outskirts of Luanda,Angola. The area lacks running water, basic sanitation and adequatehousing. The gully floods during the rainy season.
Urban challenges
45
PERSPECTIVE
PACIFIC CHALLENGESby Tuiloma Neroni Slade, Secretary General,Pacific Islands Forum Secretariat
Almost a quarter of Pacific Islanders livein urban centres (up from only 8.5 percentin 1950), and half of the countries in theregion already have majority urban popu-lations. While Vanuatu and SolomonIslands remain predominantly rural –74per cent and 81 per cent, respectively– their urban growth rates are among thehighest in the world. In Fiji, urban growthhas been compounded by the terminationof land leases in some rural areas, whichpushed renters to seek employment andshelter in towns and cities. Migration, bothrural-urban and international, has resultedin the decline of stable populations inparts of Polynesia. Rapid urban growth isparticularly significant in the context ofthe geography of Pacific Island countries.For example, the Tarawa atoll in archipe-lagic Kiribati includes some of the mostdensely populated islands in the world,
Tuiloma Neroni Slade is the Secretary General of the Pacific Islands Forum Secretariat. He was formerly a judge at the International Criminal Court inThe Hague, Netherlands; Ambassador/Permanent Representative of Samoa to the United Nations in New York and, concurrently, Ambassador to theUnited States; as well as High Commissioner to Canada. Justice Slade has also served as Attorney-General of Samoa and as senior legal adviser ofthe Commonwealth Secretariat in London.
46
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012Traditionally, the land and the sea haveprovided generations with shelter andsustenance. The links between urbancommunities and the environment areweaker. People are more dependent onstore-purchased commodities and, conse-quently, are vulnerable to the vagaries ofglobal economic fluctuations. The knock-on effects are felt as children are takenout of school, families cut back on food,and financial worries lead to increaseddomestic violence and youth crime.Despite the disadvantages, thepossibilities offered by the urban envi-ronment attract young people over anyother group. These include opportunities
There are few places in the world wherepopulation growth and urbanization collidemore starkly with vulnerability to climatechange and disaster risk than in thePacific region. This confluence of issuesis central to the focus of the Pacific Plan,the master strategy for regional devel-opment endorsed by leaders of thePacific Islands Forum in 2005 to promoteeconomic growth, sustainable develop-ment, good governance and security. Asincreasing numbers of Pacific Islandersmove to towns and cities, the region’slong-standing tradition of rural ‘subsis-tence affluence’ is being eroded, andsocieties are grappling with new aspectsof urban poverty, including undernutri-tion, youth unemployment and crime.
with certain areas reaching a density of7,000 people per square kilometre.While urbanization affects all members ofour communities, it is clear that its mani-fold social, environmental and economicconsequences significantly affect thelives of children and young people. Arecent study conducted by the PacificIslands Forum Secretariat and the PacificCentre of the United Nations DevelopmentProgramme,Urban Youth in the Pacific:Increasing resilience and reducing risk forinvolvement in crime and violence,docu-mented a wide range of links betweenurbanization and social problems, with aparticular focus on young people’s height-ened exposure to crime and violence.Another research study found that onethird of all children in Port Vila, Vanuatu,live in poverty – a rate nearly 20 per centhigher than the national average.
for artistic expression, forging of newidentities, better access to technology,wider social networks and new formsof entertainment. At the same time, thecombination of elevated school dropoutrates, unemployment and the absenceof stabilizing traditional social supportstructures renders many young peoplevulnerable to destructive influences.Proactively addressing the challengespresented by urbanization will have a greatimpact on the well-being of children andyoung people – the major players in build-ing the future success of our communitiesand ensuring the continued viability ofour environments. The situation demandsa holistic and equitable approach, begin-ning with critical issues such as access tosafe water, housing and schools. Disastermitigation and preparedness strategies arealso of fundamental importance in denselypopulated areas. At the same time, adeeper understanding of the push and pullfactors that result in the rural-urban driftmay enable us to develop sustainable,targeted and practical policies to betterharness the potential of our young peoplein both the formal and informal sectors.Pacific leaders need to make a deter-mined effort to tackle the challenges ofurbanization, because unless we addresswhat is one of the most pressing forcesof our time, the vision of the Pacific as aregion of peace, harmony, security andeconomic prosperity – where everyonecan lead free and worthwhile lives – willremain illusory. The future of the nextgeneration is at stake.
In Haiti, the January 2010 earthquake is estimated tohave destroyed 250,000 residences and 25,000 publicand commercial buildings, and to have killed an esti-mated quarter of a million people.46The underlyingcauses of the devastation and the human death tollin Haiti were manifold. Extensive deforestation haddegraded the soil, resulting in the loss of rural live-lihoods and pushing many people to move to cities.Inadequate or poorly enforced building codes meantthat few homes had been built to resist earthquakes.47(It remains an open question whether people couldhave afforded the costs of complying with higherstandards.) The slums of Port-au-Prince were over-crowded, and sanitation systems, where these existed,had long been fragile. This combination proved espe-cially conducive to the spread of disease after the event.In poor urban areas, failures in development contributeto disasters, and disasters, in turn, undo or underminedevelopment gains – deepening poverty and furtherwidening the social and health gaps separating poorfrom rich.48Routine, small-scale calamities in manysettlements result from poor governance, planning andmanagement, and often indicate vulnerability to muchlarger disasters.
The Hyogo Framework for Action, endorsed by 168governments in 2005, calls for the enhancement ofcommunities’ and countries’ resilience. Moreover,there is growing recognition of the role children havein helping themselves and their communities to be safe.In the Philippines, for example, school children madea video of the risks in their community and presentedit to the local authorities. This resulted in dialoguebetween adults and children, the planting of trees toreduce the risk of landslides, and the relocation of aschool to facilities built to minimize vulnerability toflood damage.50Case studies from the Caribbean suggest that effortsgeared towards reducing local risks – supporting, forinstance, community construction of emergency accessstairs, bridges, drains and walkways along ravines –have served to build local governance and strengthendisaster risk reduction as an integral part of city devel-opment.51In Thailand, enabling disaster survivors tomanage rehabilitation through shared communityfunds has served not only to stretch resources further,but also to enhance collectiveorganization.52Indeed, inclusive approaches often prove to be highlyeffective in solving all sorts of problems. The nextchapter provides examples from around the world andacross the spectrum of urban issues.� UNICEF/NYHQ2010-0764/Roger LeMoyne
Existing poor health and nutrition can increase disasterrisk for children, hamper recovery and, if not addressedin the emergency response, leave children more vulner-able to future shocks.
When disaster strikes, supportive environments criti-cal to children’s well-being may break down. Familiesmay remain in emergency camps for extended periods,and these dysfunctional environments can become theonly home children know during their formative years.In this context, the experience of young girls in particu-lar may be fraught with particular challenges. Simply byattempting to use distant toilet blocks or to wash wherethere is no privacy, young girls may find themselvesexposed to harassment and danger. Reports of gender-based violence are common in post-emergency settings.49Recent years have seen the emergence of initiativesaimed at reducing disaster risk.
EM28BAFebr RGua Ory ED2012
The Pinchinat camp, set up on a football field in the city of Jacmel,housed some 5,000 children and adults displaced by an earthquake thatstruck Haiti in 2010.
Urban challenges
47
CHAPTER
4
EM28BAFebr RGua Ory ED2012� UNICEF/NYHQ2011-0549/Olivier Asselin
Towards citiesfit for childrenMany cities have pursued initiatives to improvechildren’s well-being. This chapter outlines some exam-ples of good practice spanning service delivery, socialprotection and safe and inclusive urban environments.These cases illustrate the myriad possibilities and bene-fits of including children and their interests in urbandesign and management.
Policy and collaboration
National policies – particularly decentralization –can enable municipalities to deliver for children. Forinstance, in 1991, the Philippines enacted the LocalGovernment Code, granting fiscal and administrativeautonomy and planning authority to local governmentunits. This opened the door for a number of localities– notably Pasay City, a subdivision of MetropolitanManila – to pursue pro-child urban governance. Inaddition to creating plans and evaluating projects, thePasay City Child Welfare Council, the regulatory bodyresponsible for all initiatives for children, promoteschild-friendly regulations and budgets, provides
EM28BAFebr RGua Ory ED2012
technical assistance to community-based workers andprepares contingency measures to protect children andtheir families in crisis situations.1Collaboration between authorities and child rightsagencies can facilitate such efforts. In 1999, theBrazilian state of Ceara teamed up with UNICEF tolaunch the Municipal Seal of Approval, an initiativethat encourages mayors to promote child well-beingthrough local cultural, political and administrativechannels. By recognizing and rewarding success, theprogramme provides municipal authorities with strongincentives to prioritize the well-being of children andyoung people in their jurisdictions. The initiativehas now spread to over a thousand municipalitiesacross Brazil and has been taken up by other coun-tries in the region; mayors from El Salvador signed upin 2009. Within Brazil, it became the inspiration forthe Platform for Urban Centres, which aims to reducedisparities that affect children and adolescents livingin large cities.
Towards cities fit for children
49
The impetus for collaboration can come from thecommunity itself. Shack/Slum Dwellers International(SDI) is a global alliance of 34 national federations ofcommunity-based organizations in developing coun-tries. SDI represents associations of the urban poor thathave come together to work towards secure habitats,basic amenities and safer neighbourhoods in dialoguewith local and national governments. The movementis founded on empowering women, and children’sinterests rank high on the agenda.‘Bottom-up’ approaches are prevalent in many cities.Civil society organizations and community institutions– including, among others, houses of worship – areoften closest to the issues of greatest importance to themost excluded communities. These issues may includewater and sanitation, housing, health, education andchildcare. In urban settings lacking effective formalmeans of participatory decision-making, communityorganizations can enable citizens, including youngpeople, to express their concerns. The challenge is toalign the efforts of groups that work to alleviate theplight of the urban poor with those that focus onprotecting the rights of the most vulnerablechildren.
of the city’s population, to submit proposals to obtainfunds for projects they choose to implement. Braziliancities pioneered this approach more than a decade agoand although many retain participatory budgeting, fewcontinue to include adolescents in theprocess.In some cities, young slum residents are involved insurveying, documenting and mapping their urbansurroundings, generating essential information forboth their communities and municipal authorities.Such initiatives have helped build partnerships withofficial agencies in ways that enable young peopleto play a part in influencing the planning, financeand management of urban infrastructure. Children’scommunity mapping has proved successful in pinpoint-ing local needs and resources in places as diverse asKolkata, India; Nairobi, Kenya; Karachi, Pakistan; andCape Town, South Africa.Participatory approaches are not without their challenges.It may be difficult to ensure that the most marginal-ized children are adequately represented, and carefulplanning is needed to ensure that participation is nottokenistic. Coordination is further complicated by thefragmentation of service delivery. Agencies responsi-ble for water, sanitation, waste management, pollutioncontrol or public transport may not explicitly giveconsideration to children as users and may lack exper-tise in appropriate approaches.Nevertheless, the critical mass and dynamic socialexchange characteristic of urban environments canprovide singular opportunities for children. A healthyand vibrant city opens avenues to varied educationaloptions; recreational, social and cultural choices;civic engagement; women’s empowerment and youthemployment, among other benefits and opportuni-ties. Young people can be involved in micro-planningcommunity water and sanitation models, or they maytake part in civil society networks that protect childrenfrom exploitation. Children’s participation can bothhelp guarantee their rights to basic services and protec-tion and contribute to their development as activemembers of society.
Participatory urbanplanning and management
Children’s right to have their views taken into accountin all matters affecting them is enshrined in theConvention on the Rights of the Child. Nevertheless,children are seldom invited to take part in decisionsinforming urban planning and design. Urban decision-making and governance on such issues as road safety,land use and air quality can have direct and adverseeffects on the lives of both current and future generationsof children.Participatory budgeting, which in some cities involvesyoung citizens in determining how a portion of themunicipal budget is spent, can bring about improvedresults for children.2In Ventanilla, Peru, a successfulpilot scheme introduced in 2008 has allowed childrenand adolescents, who represent a significant portion
50
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
PERSPECTIVE
BUILDING CHILDREN’SLIVES TO BUILD A CITYby José Clodoveu de Arruda Coelho Neto,Mayor, Sobral Municipality, Brazil
Urban growth adds to the challengesof ensuring that people can enjoy anadequate standard of living.In Sobral, a municipality in the northwestof the state of Ceara and home to morethan 188,000 people, serious efforts havebeen made to include an expandingpopulation in the labour market, schools,housing and all the social and economicaspects of daily life.
Almost 70,000 people – just over a third ofSobral’s population – are not yet 19. Withthe right policies and services, we canplay a part in creating an environment inwhich they can thrive and build healthy,fulfilling lives.Although enabling children to realize theirrights is part of our mandate, successcan also bring long-term rewards. Today’sbeneficiaries are likely to become tomor-row’s benefactors, contributing tostronger, more cohesive communities.
So much needs to be done. An increasingpopulation puts existing resources understrain. Poverty and inequality create asense of helplessness and frustration,which in turn often leads to crime andviolence – daily realities in urban centresacross the region – complicating thealready complex process of fosteringan environment where children can grow.It is difficult not to notice the factorsthat make young people especiallysusceptible to violence: poor quality oflife, limited opportunities for developmentand recreation, and an absence ofviable prospects.
José Clodoveu de Arruda Coelho Neto is a lawyer and professor. Politically active since his youth, he served as vice-mayor of Sobral from 2005 to 2010and became mayor in January 2011.
EM28BAFebr RGua Ory ED2012Sobral is pursuing a series of intercon-nected initiatives to enable all its chil-dren, regardless of background, tohave access to appropriate tools tofully develop their capacities. We havesteadily focused on enhancing education,chiefly by renovating school facili-ties and providing continuous coachingto teachers – efforts rewarded byimproved results in national tests. Weare working to extend access to otherforms of training, for example througha planned partnership with the Palaceof Sciences and Foreign Languages todeliver language and information tech-nology programmes. This would build onsuccessful initiatives already in place.The School of Music offers compli-mentary courses in a variety of musicalinstruments to nearly 650 students,largely from public schools. The SchoolWorkshop of Arts and Professionsprovides training in such professionalskills as preserving the city’s historicalheritage. In addition, more than 10,000 ofour students participate in after-schoolsports and tutorial classes under SecondRound, a federal government project.
Of course, an environment conduciveto child well-being cannot be createdthrough sporadic, isolated actions.We need a comprehensive, concertedapproach to policymaking as well as inte-gral service delivery. Our achievements inimproving the lives of children and youthhave earned us the UNICEF MunicipalSeal of Approval every time it has beenissued: in 2000, 2002, 2004, 2006 and 2008.
Our municipality also recognizes theeducational and social benefits of sports– especially their contribution to buildingdecision-making skills, respect for diver-sity and confidence among young people.Our Social Nucleus of Sports Initiationprogramme allows children and adoles-cents to practice sports by making existingsports facilities in all districts of the cityavailable and accessible to them. We alsopartner with child rights advocates and alocal business to promote the participationof marginalized youth in cultural workshopsand training programmes. Many of theseyoung people are adolescents who areexcluded because they have experienceddrug addiction, pregnancy or sexual abuse.Beyond the numbers and formal initia-tives, individual stories tell us that ourefforts help adolescents make positivedecisions to the benefit of their communi-ties. I remember one young man who, at arecent project impact assessment meet-ing, said that many of his friends had beenlost to drugs and crime. He had found themotivation to succeed despite the odds.Having entered the School Workshopvocational training programme at 16, hewas now, 10 years later, working as aninstructor in historical restoration.I am one of countless mayors facingsimilar challenges and opportunities. Weall have our own insights and experiences.But some motivations are universal – thesatisfaction of seeing children on the brinkturn their lives around and become rolemodels for others. This is why I believe inthe unique role of local government – inSobral and around the world.
Towards cities fit for childrenTowards
51
FOCUS ON
URBAN HEART
Measuring and responding to health inequityexisting interventions and are effectiveand sustainable over time.The tool is based on three essentialelements:S• ound evidence: reliable, representative and comparable data, disaggregated bysex, age, socio-economic status, majorgeographical or administrative region,and ethnicity, as appropriate• ntersectoral action for health: building Irelationships beyond the health sectorin order to influence a broad range ofhealth determinants – in particular,working with other government sectors(e.g., education, transport and publicworks), community groups and non-governmental organizations• ommunity participation: involving Ccommunity members in all aspects of theprocess, from planning, designing andimplementing interventions to helpingensure that these efforts are learned fromand sustained beyond the initial phase.Urban HEART revolves around a planningand implementation cycle compris-ing four phases: assessment, response,policy and programme. Monitoring andevaluation take place during each phase.Urban health inequities are identified inthe assessment phase. Evidence gath-ered at this stage forms the basis forraising awareness, determining solutionsand promoting action.
The spectrum of urban living conditionsis reflected in the health of a city’s resi-dents. Despite the wide disparities inhealth outcomes that stem from differ-ential circumstances, few countriesroutinely examine such inequities withinor between cities.The Urban Health Equity Assessmentand Response Tool (Urban HEART) helpsurban policymakers, communities andother stakeholders better understand thelocal socio-economic factors that influ-ence health outcomes. Developed bythe World Health Organization (WHO),Urban HEART is designed to tackle urbanhealth inequities – avoidable differencesin health that are socially producedrather than biologically determined. Thetool serves to identify and correct poli-cies that perpetuate these inequities – forinstance, the higher rates of illness anddeath among the children of families inurban poverty than among those borninto relatively affluent homes.Urban HEART provides local and nationalauthorities with the evidence they needto set priorities, allocate resources andmobilize urban communities to promotehealth equity. To determine which inter-ventions are likely to improve health andreduce inequities, this evidence seeks toshow not just the immediate causes ofdisease but also the ‘causes of causes’– underlying social hierarchies and theresulting conditions in which peoplegrow, live, work and age.Reducing health and social inequitiesis complex. Implementation of UrbanHEART focuses on local solutions thatengage all stakeholders, consider
52
THESTATE OF THE WORLD’S CHILDREN 2012STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012Defining theproblem
Figure 4 .1 . Urban HEART planning and implementation cycle
Setting theagenda
AssessmentMonitoringand evaluation
Response
URBAN HEARTProgrammePolicy
Implementingthe programme
Developingpolicy
Source:WHO Urban HEART.
During the policy stage, the mostrelevant interventions are prioritizedand budgeted to ensure that they becomepart of the local government policy-making process. Success is measuredby the laws, programmes and interven-tions implemented.
Programme implementation hinges onresources and time frames determined bylocal authorities. Health sector programmesimplementing pro-equity health policies arecomplemented by other sectors’ actionsto bring about health equity.
Figure 4 .2 . Twelve core indicatorsHealthInfant mortalityDiabetesTuberculosisRoad trafficinjuries
EM28BAFebr RGua Ory ED2012Physical environmentand infrastructureAccess to safe waterAccess to improvedsanitation
The response stage involves identify-ing appropriate responses, designatingkey actors, defining goals and estab-lishing targets. This is an opportunity toengage all relevant sectors and commu-nities in setting the agenda – determiningwhich policies, programmes and proj-ects should be introduced, continued,expanded, improved, changed or stoppedto achieve equity goals.
Monitoring and evaluation encompassboth process and outcomes.Core indicatorsIndicators measuring selected healthoutcomes and social determinants fordifferent urban population groups formthe basis of the assessment compo-nent of Urban HEART. Indicators fall intotwo main categories: health outcomes(shown in blue in Figure 4.2) and socialdeterminants of health (shown in grey).Twelve core indicators are used acrossall Urban HEART schemes, allowingcomparison across cities and countries.This basic set was selected to providea general picture of the urban healthsituation in any urban setting, based ongenerally available data, universalityand potential to uncover inequity. The12 ‘core’ indicators are complemented by‘strongly recommended’ and ‘optional’ones to provide an analysis responsiveto local priorities and specific healthequity concerns. It is recommended that
each indicator be further disaggregatedby location, sex, age and/or socio-economic group.Embedding Urban HEARTUrban HEART is primarily a tool toenhance current interventions as part ofexisting national and local health plan-ning and programme frameworks. Thechosen health equity solutions shouldbe results-focused, cost-effective andtimely; use available local resourceswhere possible; ensure broad supportamong affected communities; and complywith national priorities. Interventionstrategies include incorporating healthin urban planning and development,strengthening the role of urban primaryhealth care and promoting an emphasison health equity.
Social and humandevelopmentCompletion ofprimary educationSkilled birthattendanceFully immunizedchildrenPrevalence oftobacco smoking
EconomicsUnemployment
governancegovernmentspending on health
WHO Urban HEART was developed by the WHO Centre for Health Development in Kobe, Japan (WHO Kobe Centre), in collaboration with regional officesof WHO and city and national officials from across the world. In total, 16 municipalities and 1 state in 10 countries – Brazil, Indonesia, Iran (IslamicRepublic of), Kenya, Malaysia, Mexico, Mongolia, the Philippines, Sri Lanka and Viet Nam – participated in the pilot scheme.
Towards cities fit for children
53
PERSPECTIVE
TRAFFICkED CHILDRENIN OUR CITIESby Ricky Martin, UNICEF Goodwill Ambassador
Protecting the exploited in the Americas
For the most part, trafficking is deniedor ignored – even if, by some estimates,it is a global industry with US$32 billionin annual profits from forced labour.Trafficked children toil behind the wallsof private homes, hotel rooms and sweat-shops – obscure places from which mostnever come forward for fear of prosecu-tion or, for those who were taken acrossborders, deportation.I was moved to join the fight againsttrafficking when I visited India in 2002.In 2006 I launched Llama y Vive (Calland Live), a campaign that establishedand promoted prevention and victim-protection hotlines. A first for the regionwhen it was launched, the campaignhas taken root in Costa Rica, Ecuador,Mexico, Nicaragua and Peru as wellas in in the Hispanic community ofWashington, D.C.
Multiple Grammy winner, renowned international artist and UNICEF Goodwill Ambassador since 2003, Ricky Martin established the Ricky MartinFoundation to advocate for the well-being of children around the globe.
54
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012The testimonies we collected were heart-breaking but ultimately enabled us torecommend ways to end this noxiousthreat to our children and communities.One consequence of these recommen-dations will be the construction of a safehaven for children and young peoplein the coastal town of Loiza, where theincidence of trafficking is high.To effectively address this scourge, wemust begin by establishing a universaldefinition of trafficking. Child traffick-ing must be distinguished from humansmuggling and the activities of orga-nized crime. Doing so will help generatemore specific data on which to base poli-cies designed to protect children. Betterinformation will also help ensure thatpeople in general, and policymakers inparticular, see all aspects of the prob-lem – a key to mobilizing political supportfor adequate anti-trafficking legislationand enforcement.
There are an estimated 2.5 million peopleworldwide who have been trafficked intoforced labour. Some 22 to 50 per centof trafficking victims are children. Theprecise magnitude of the problem is diffi-cult to ascertain because definitions varyand trafficking is a clandestine business.We do know that children are usuallytrafficked from rural to urban areas andthat the forms of exploitation to whichthey are subjected – domestic servitude,sexual exploitation linked to tourism, anddrug running, to name a few – are mostcommon in highly populated places andon the streets.
In my homeland of Puerto Rico, I collabo-rated with the University of Puerto Ricoand the Protection Project at JohnsHopkins University on the first study oftrafficking in the territory. Among otherthings, we learned that although theUnited States passed the TraffickingVictims Protection Act in 2000, there areno comprehensive local laws to combatthis crime in Puerto Rico.
Effective anti-trafficking laws must bepassed in conjunction with work doneby local protection offices. In order todo this, we urgently need governments,non-governmental organizations andmultilateral agencies to work in concertto raise awareness, implement holistictraining and guidance programmes forenforcement agencies and build effectivesystems to protect children and prose-cute and punish perpetrators.Finally, it is our responsibility to supportsurvivors of trafficking. We must endeav-our to create a safe environment thatallows survivors to come forwarddespite the inherent difficulties. Policiesmust be revised to exempt identifiedvictims of trafficking from persecutionor deportation, and assistance mustbe provided to help their reintegration,including tracing families where appro-priate. Some of these actions havealready been initiated at the state andinternational levels.It is easy to forget the silent and invisible– especially when they are lost amongthe masses in congested cities. For thisreason, we must reinforce and developeffective solutions to put child traffickingat the top of the agenda. Taking actionnow can help address the root causesof trafficking, safeguarding children anddefending their right to protection andsocialdevelopment.
Child-Friendly CitiesThe Child-Friendly Cities Initiative has generated someof the most effective models for involving children inthe governance and development of their communities.In essence, cities aspiring to be ‘child-friendly’ committo implementing the principles of the Convention onthe Rights of the Child, including through a strongparticipatory approach and the mainstreaming of chil-dren’s rights in budgets and policies.Tracking improvements in child well-being over timeis an important component of the initiative. It hasbecome apparent that traditional assessment meth-ods are not always sufficient to reveal the extantdifferences in child well-being across neighbourhoodswithin a city. More rigorous monitoring and evalua-tion, with children and communities playing a greaterpart in collection and ownership of data, are necessaryto ensure equitable progress. To address these needs,the Child-Friendly Cities and Communities ResearchInitiative led to the development of a set of indicatorsand tools to assemble a wider range of disaggregateddata, enabling more meaningful community engage-ment in local planning processes. The methodology isbased on the experience of nine countries representinga variety of geographic, socio-economic and culturalcontexts: Brazil, the Dominican Republic, France,Italy, Jordan, Morocco, the Philippines, Spain andtheSudan.3Many towns and cities form children’s councils as away to involve children in governance. This concept istaken further in the Dominican Republic, where child-friendly towns engage all schoolchildren in electionsfor the children’s council, using this as an opportu-nity to teach citizenship rights. Children can also bedirectly involved in decisions that affect their lives byparticipating in the management of school and earlychildhood facilities; the planning and design of commu-nity recreation areas; the assessment and monitoring ofthe physical environment of their neighbourhoods; andthe running of children’s organizations.4
gender or any other distinction is paramount. Forsome children, such as those with disabilities, addi-tional measures may be necessary to ensure equalityofopportunity.Within the urban context, an inclusive environmentcan be created with a focus on two major issues: spaceand transportation. Cities must be designed to mini-mize the social and structural barriers children withdisabilities may face. Improving physical access toservices, for example by building wheelchair ramps, isonly a starting point in a strategy that must both strivefor equal access for all children with disabilities andtarget the causes of social marginalization. The mosteffective initiatives are often those that enable childrenwith disabilities to interact with non-disabled peers –in classrooms and recreational settings.The parents of children with disabilities in Bangalore,India, found that none of the parks or playgroundsin their garden city were accessible to children withphysical disabilities. So they set up Kilikili, a non-governmental organization, in order to create inclusiveneighbourhood play spaces for all children, regardlessof their abilities, and to involve children in the designprocess. The success of this initiative led to a partner-ship with the Bangalore Municipal Corporation.5As discussed in the preceding chapters, while urbansettings may offer a greater range of services than ruralareas, children from poorer families or marginalizedcommunities do not always enjoy equal access to theseservices. Children growing up in urban environments –especially those who live with disabilities, happen to befemale, live on the street or belong to a minority – mayhave particular protection needs.
Non-discriminationThe right to non-discrimination is one of the four over-arching principles of the Convention on the Rightsof the Child. Ensuring that all children are treatedequally regardless of race, ethnicity, language, religion,
EM28BAFebr RGua Ory ED2012
Nutrition and hungerIn the informal settlement of Korogocho in the Kenyancapital of Nairobi, where around 200,000 people livein crowded conditions, the combination of extremepoverty and lack of basic services threatens the healthand development of children. The Korogocho NutritionProgramme involves a range of cost-effective interven-tions, including treatment for malnutrition, vitamin Asupplementation and deworming, as well as promo-tion of breastfeeding and improved hygienepractices.
Towards cities fit for children
55
FOCUS ON
THE CHILD-FRIENDLYCITIES INITIATIVE
Fifteen years of trailblazing workWhile these are necessary componentsof child-friendly programming andadvocacy, true ‘child-friendliness’ canonly be achieved through a long-termcommitment to the implementation ofchildrights.The Child-Friendly Cities approach canbe adapted to diverse contexts. In high-income countries, the focus has beenlargely on urban planning, safe andgreen environments and child participa-tion. Low-income countries have tendedto prioritize service delivery in health,nutrition, education and child protection.Child-Friendly Cities initiatives range fromsingle-city endeavours (as in Amman,Jordan) to national-level networks (as inFrance). The potential to promote child-centred governance at the local level isleading to the spread of child-friendlyapproaches beyond large cities and evento rural settings, for instance in Moroccoand the Sudan.In the Philippines, the Child-FriendlyMovement has established an accredi-tation mechanism for urban communitiesand municipalities, measuring improve-ments in 24 priority indicators of childwell-being in the fields of protection,health, nutrition, education, water andsanitation, and participation.In the absence of a formal evaluationmechanism, the benefits of CFCI can bedemonstrated by example. In 2005, localauthorities in Brazil that had earned theMunicipal Seal of Approval were foundto have cut infant mortality by 16.4 percent (against 12.1 per cent elsewhere)and neonatal mortality by 8.5 per cent(against 1.6per cent), while increasingaccess to early childhood educationfrom 56 per 100 children to 63.5 per 100.Underpinning child-friendly urbanplanning and programming is a humanrights-based governance model thatembodies the principles of non-discrimination, survival and develop-ment, and participation enshrined in theConvention on the Rights of the Child.Children are recognized as rights holderswho should be involved in both plan-ning and implementation of measuresthat affect them. By making neglectedgroups more visible and granting all chil-dren a platform to secure their needs andrights, the Child-Friendly Cities approachcontributes to achieving developmentgoals with equity.
City administrations have had to facesignificant challenges in addressing theneeds of a growing urban population.Coinciding with increasing decentraliza-tion and as part of efforts to strengthengovernance, CFCI taps into the wideracceptance of community participa-tion in decision-making to promote localaccountability for children’s rights.
The International Secretariat of CFCIhas identified nine principal buildingblocks for local administrations aiming tobecome ‘child-friendly’:1. Child participation at all stages ofplanning and implementation2. Child-friendly legislation3. A child rights strategy4. A coordinating mechanism or agencyfor children5. Assessment of policy andprogramme impact on children6. A budget and resources for children7. A regular report on the state ofchildren in the city8. Awareness-raising and capacitybuilding on child rights9. Independent advocacy for children.
56
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012Integrated, multi-level approaches arean important feature of the Child-FriendlyCities movement. In Brazil, the Platformsfor Urban Centres promote synergyamong municipal and state authoritiesand other stakeholders in order to reducesocio-economic inequalities affectingchildren in the biggest cities. Childrenand other community members assesschildren’s living conditions and developa plan of action that includes perfor-mance indicators for communitiesand municipalities.
With nearly half of the world’s childrennow living in towns and cities, urbanplanners and policymakers need to payspecial attention to the rights and inter-ests of children. The Child-FriendlyCities Initiative (CFCI) – launched byUNICEF and the United Nations HumanSettlements Programme (UN-Habitat) in1996 – is the first multi-stakeholder part-nership to put children at the centre ofthe urban agenda.
� UNICEF/NYHQ2006-1483/Giacomo Pirozzi
A peer educator discusses how to prevent HIV/AIDS and other sexually transmitted diseases in Barangay Don Carlos, a poor neighbourhood inPasay City, Metropolitan Manila, Philippines.
Farming within and on the fringes of urban areas – onabandoned plots, community allotments or roofs, orin sacks and containers, for example – is an increas-ingly important means of enhancing food security andgenerating income. Around half the food consumedin Hanoi, Viet Nam, in 2001 was grown in the city.6Additional benefits accrue as the presence of trees andcrop plants enhances urban air quality and contributesto a healthier, greener environment for children.7
HealthThe Global Equity Gauge Alliance is an internationalinitiative designed to target urban health inequities.For example, in Cape Town, South Africa, communi-ties and health workers were involved at every stageof the project, which entailed reallocating healthstaff, running health promotion programmes inschools and piloting the introduction of dry toilets ininformalsettlements.8
EM28BAFebr RGua Ory ED2012HIV and AIDS
In the neighbourhood of San Juan de Lurigancho inmetropolitan Lima, Peru, the Stronger Voices forReproductive Health project focuses on improving thequality and accessibility of reproductive health servicesfor adolescent girls and other young people, many ofthem indigenous migrants, by consulting them on howbest to deliver these services.9
Engaging young people is an essential ingredient ofsuccessful efforts to prevent HIV. Take the case ofShuga,a television drama set and produced in Nairobi,Kenya. The show uses a plot revolving around youngurban Kenyans to explore such themes as alcoholabuse, risky sexual behaviour, stigma and HIV. Anassessment of viewers – adolescents and young people– found that quality popular media can be a success-ful channel through which to transmit knowledge andpromote safer practices.10
Towards cities fit for children
57
The Brazil Active project aims to protect children wholive or work on the street and therefore are at higherrisk of contracting HIV and other sexually transmit-ted diseases. These children are particularly vulnerableto rape, sexual exploitation and drug abuse. Breakingwith a legacy of mistreatment, the project involves localnon-governmental organizations (NGOs) in creatingsafe spaces, recreational opportunities and measures toprevent HIV and sexually transmitted diseases for thesemarginalized children and adolescents in the cities ofRecife, Rio de Janeiro and Salvador. The NGOs alsoexchange examples of best practice and advocate forchanges in public policies to address HIV preventionamong children living and working on the streets.
Particular attention should be devoted to extendingservices to slums and informal settlements. User fees,where applicable, must be kept low enough to avoidexcluding the poorest. Climate change adaptationstrategies, including disaster risk reduction plans andmeasures to increase infrastructure resiliency, shouldalso be implemented.
EducationAccess to education for poor and marginalized chil-dren, including the provision of quality schooling ininformal settlements, is of paramount importance.Other forms of training, such as vocational courses,can be particularly useful for adolescents seeking tosecure future livelihoods in the urban context. Whetherthrough classroom or on-the-job training, appren-ticeships or skill-specific courses such as language orcomputer training, vocational initiatives should aim toincrease young people’s employability.Accelerated learning programmes are a practicalsolution for children who may have had their school-ing disrupted, whether by emergency or circumstance.Such programmes offer students the opportunityto follow certified education courses on the basis ofcompetency, not age or previous grade.In Bangladesh, the Basic Education for Hard-to-Reach Urban Working Children project was set up toprovide quality non-formal training in basic literacy,numeracy and life skills. Between 2004 and 2011, theprogramme reached almost 200,000 children in sixcities. Evaluations showed that the project was effectivein developing an appropriate curriculum and materi-als that were tailored to the children’s needs, allowingthem to overcome the limitations of their environmentand receive a quality education. The project providesuseful lessons for similar efforts elsewhere.The Biratnagar Working Children’s Club, in Nepal, isan example of children and young people establishingsocial support networks based on shared educationalexperiences. Graduates of the local two-year supple-mentary educational programme for working childrenestablished the network in order to continue regularlymeeting their peers after completing the course. Sincethe first club was founded in 2001, the network has
Water, sanitation and hygieneAccording to the World Health Organization, everyUS$1 spent on improving water supply and sanitationproduces economic gains of at least US$5 and perhapsas much as US$28, depending on local circumstances.Investment in hygiene promotion, sanitation and waterservices is also among the most cost-effective ways ofreducing child mortality.11
Of course, improved investment in water, sanitationand hygiene is urgently needed in both rural and urbansettings. The urban water and sanitation situation,while comparatively better, is worsening as provi-sion fails to keep pace with urban population growth.
� UNICEF/NYHQ2006-2402/Susan Markisz
An indigenous Wayuu woman holds her newborn daughter in MaracaiboCity, Zulia state, Bolivarian Republic of Venezuela. The family is partic-ipating in the Ministry of Health Trio por la Vida programme, whichpromotes birth registration, breastfeeding and immunization.
58
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
� UNICEF/NEPA2011/Karki
Girls attending the Urban Out of School Programme in Biratnagar, Nepal. The programme offers working and underprivileged children anopportunity to catch up on their education.
grown to include over 2,000 members – more than halfof whom are girls – across the whole city. The clubsraise awareness of child rights; campaign on importantissues, such as exploitative labour, child marriage andtrafficking; and advocate for more child participation inschools, in the community and in governance – includ-ing by working with municipal authorities to makeBiratnagar a child-friendly city. Many of those who havegone on to pursue college education or professionalcareers return to the club to mentor their younger peers.Mobile libraries are an effective way of making surethat all children have access to books. In Manila,Philippines, for example, library carts deliver books toworking children.12The Forsa (Opportunity) programme based in ElMarg, a large slum community outside Cairo, Egypt,provides three months’ training to young people and
EM28BAFebr RGua Ory ED2012
helps them secure employment. Trainees are recruitedvia posters, roadshows and social media. The project,run by Plan International, was developed by the CAPFoundation, a public-private partnership aiming toalleviate poverty by linking the learning and livelihoodneeds of working children and disadvantaged youth. Itwas first tried successfully in India.13Following the influx of Iraqi refugees into Syria – morethan 200,000 people, according to 2009 data, themajority settling in Damascus – the Syrian Governmentopened the doors of its public schools to Iraqi children.Allowances were made for late registration and cross-border examinations. Among the obstacles encounteredwere the absence of school records, children’s needto work to contribute to their family’s income, anddifferences between the Iraqi and Syrian curricula. Anumber of innovative approaches were pursued. Oneinvolved ‘education volunteers’ – selected professionals
Towards cities fit for children
59
Drug use among adolescents and young people is agrowing problem in the rapidly urbanizing Sunsaridistrict of Nepal. A local community-based organiza-tion, Kirat Yakthung Chumlung, reaches out to drugusers through peer leaders with similar backgroundsand works closely with other agencies to provide vitalservices, such as rehabilitation, needle and syringeexchange, and HIV testing and counselling.Project Smile in Pakistan’s Punjab province offers abroad range of services to children who live or work onthe street, and who may be ostracized because peopleassociate them with drug use and other risky behaviour.A mobile team of trained health and social workersprovides participants with access to services includingmedical care, food, clean clothes, counselling, referralfor drug treatment, and training. The service also oper-ates a drop-in centre and a peer education programme.Communities can also help transform social habits,attitudes and practices. Simple but straightforwardcampaigns have helped transform such violent citiesas Bogota, Colombia. Here, three campaigns – ‘brokenwindow’, ‘zero tolerance’ and ‘carrot hour’ – succeededin reducing crime rates by improving infrastructureand reducing hours for alcohol consumption.
� UNICEF/GUAA2010/Donna Cesare
Students attend computer classes as part of the CEIBA Programme,which provides supplementary education to young people inmarginalized communities in Guatemala.
Child protection
The UN-Habitat Safer Cities Programme seeks totackle violence within the world’s cities, especiallyin Africa, by developing municipal-level preventionstrategies. Participatory processes are used to estab-lish regional plans to reduce overall levels of urbanviolence. The programme holds regional conferenceswhere young people have a chance to talk with govern-ment agencies, civil society organizations, the policeand magistrates to identify the causes of and possibleapproaches to violence among their peergroup.15The CEIBA Programme in Guatemala aims to createa protective environment to counteract the unhealthyinfluence of drugs and gangs on young people in poorsections of Guatemala City and nine other municipal-ities. The programme emphasizes a quality educationfor younger children, provides training in skills suitedto the local job market and offers community coun-selling to help parents find alternatives to violentstreet culture.
60
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
from the Iraqi refugee community – whose role wasto identify not only out-of-school children, but alsoteachers who could provide remedial classes insubjects such as English, Arabic and mathematics. Thevolunteers also acted as a conduit for communicationbetween the United Nations High Commissioner forRefugees and the refugee community.14
Housing and infrastructureFamilies cannot adequately support their children if theylive in precarious circumstances or under threat of evic-tion. Evidence shows that adequate housing can protectchildren and families living in dense urban areas fromcommunicable and chronic diseases as well as injuriesand accidents. Good environments promote social inter-action, limit psychological stress and bolsterhealth.The best national and municipal policies recognize thatthe urban poor need not only housing, but also basicservices. In Brazil, for example, efforts to address a leg-acy of inequity and exclusion through investment inurban housing and infrastructure include the federalgovernment’s Minha Casa, Minha Vida (My Home,My Life) programme, which aims to build 3 millionhomes in five years while also prioritizing social provi-sion for the poor through education, cash transfersand job creation. This initiative is one of many aiming
to turn the right to housing and ‘right to the city’enshrined in Brazil’s Constitution and innovative CityStatute into reality.
Urban planning forchildren’s safetyUrban planning needs to ensure that children can movesafely within their environments. As noted in Chapter 2,road traffic injuries claim a disproportionate numberof young lives in low- and middle-income countries.It is common for high-speed roads to be routed closeto schools or through residential areas. Cities mustbe designed in a way that reduces risk to children.Segregating traffic and reducing speed can save lives.Sweden’s Vision Zero road safety policy, introducedin the late 1990s, uses car-free play areas, bicycle andpedestrian lanes, and tunnels to protect vulnerableroad users. Where it is not possible to separate motortraffic from others on the road, such measures as speedlimits are used to safeguard pedestrians.16
The UN-Women Global Programme on Safe CitiesFree of Violence against Women and Girls, working inpartnership with five cities around the world, endeav-ours to find the best comprehensive approaches toprevent and reduce violence against women and girlsin public spaces.18Based on successful pilot schemes inLatin America and grounded in rigorous assessment,the initiative is developing a model to be used by localauthorities and decision-makers that encompassesgood governance, urban planning and political partic-ipation. Data collection is critical to the success of theinitiative. The absence of reliable and situation-specificinformation conceals problems and hinders the devel-opment of solutions.Notable among specific initiatives is Safe Spaces, estab-lished in Kenya in 2008 by Peninah Nthenya Musyimi,the first girl from Nairobi’s Mathare slum to graduatefrom university and now a women’s rights advocate.The organization creates safe environments for adoles-cent girls growing up in slums, providing spaces forrecreation, opportunities for mentoring and a forum fordiscussion.19Biruh Tesfa (Bright Future) is a governmentprogramme for girls at risk of exploitation and abuse in aslum area of Addis Ababa, Ethiopia. The project reachesout to girls aged 10–19, mostly migrants living awayfrom their families, who are out of school. It providesthem with a space to build peer support networks andoffers tuition in literacy, life skills, reproductive healthand livelihoods.� UNICEF/NYHQ2004-0707/Giacomo Pirozzi
Bogota, Colombia, has been implementing strategiesto cater to the needs of non-motorized road users,improving public transport and significantly decreas-ing transit times. Between 1995 and 2002, the cityintroduced dedicated cycling and pedestrian-onlyroutes, excluded cars from its centre and developed arapid transit bus system capable of carrying 700,000people a day. Subsequently, traffic fatalities fell by50 per cent.17
Safe cities for girls
Sexual harassment and violence are a daily realityfor girls and women in urban public spaces, and onethat has been largely neglected. The risk and reality ofviolence limit women’s freedom to exercise their rights,as equal citizens, to education, work, recreation andpolitical expression. Those living in poverty may beexposed to heightened risk if they walk through inse-cure areas to reach school or work. It is increasinglyrecognized that cities that are safe for women and girlsare safe for all, yet municipal development and safetyplans frequently overlook specific threats to womenand girls.
EM28BAFebr RGua Ory ED2012
A group session at a centre for children and adolescents in Kaliningrad,Russian Federation. The facility offers counselling on drugs, alcohol,HIV/AIDS, abuse and other issues.
Towards cities fit for children
61
Safer, more inclusive and more accessible cities cancome about only if girls participate in creating them.Experts in their urban realities, girls can activelycontribute to urban design and municipal decision-making – a process that, in turn, can empower them tobecome municipal leaders of the future.
come up with ideas for creating small play spacesbetween residences.24Children also need access to nature. There is a largebody of evidence indicating that exposure to trees,water and other aspects of the natural landscape haspositive impacts on children’s physical, mental, socialand spiritual health.25Contact with nature has beenfound to restore children’s ability to concentrate, whichis the basis for improved cognition and psychologicalwell-being.26Measures that bring nature and its bene-fits to children include tree-planting programmes inurban neighbourhoods, incorporating green areas intomunicipal housing and using plants, sand and water inchildren’s playgrounds.
Safe spaces for playPlay, both spontaneous and organized, is an importantcomponent of healthy development. When childrenplay, they reap the benefits of physical exercise, developadvanced motor skills and find relief from stress andanxiety. Play also promotes children’s cognition, creativ-ity and socialization. In urban settings, public playspaces can help mitigate the effects of overcrowding andlack of privacy in the home and may enable childrento mix with peers of different ages and backgrounds,laying the foundation for a more equitable society.Facilitating play can also serve to counteract increasingrates of obesity and overweight among children, whichare related not only to changes in diet but also to asedentary lifestyle reinforced by, among other things,the loss of recreational opportunities.20Children withdisabilities are at a higher risk of obesity, not leastbecause they may have more difficulty obtaining suffi-cient physical exercise.21
WHO recommends at least one hour of daily physicalactivity for children aged 5−17. Urban planners andother authorities can create better opportunities for chil-dren to participate in physical activities by providing safeand accessible spaces for recreation and designing neigh-bourhoods, streets and outdoor spaces that encourageactive transportation, including walking and cycling.In this vein, some cities in Europe, South Africa and theUnited States have initiated programmes to close offstreets either permanently or at particular times so thatchildren have a safe place to play outdoors.22Examplesinclude the Dutchwoonerf,where closing one end of astreet to through traffic effectively reclaims it for chil-dren, reinforcing a sense of community and safety.23
Neighbourhood play spaces can be created withmodest material assistance from local governments.With such support, communities can, for example,conduct mapping exercises in order to collectively
62
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012Cultural inclusion
Social capital
Social capital is pivotal to the development of childrenand young people. Trust, reciprocity and a sense ofbelonging within their family, school, peer groups andlarger community have far-reaching effects on chil-dren’s opportunities, choices and outcomes in life.Just as physical toxicity threatens human survival andwell-being, a toxic social environment – for exam-ple, one in which violence, deprivation and abuse arecommon – can hamper the development of childrenand adolescents. In general, children are less mobilethan adults and can exercise only limited control overtheir external circumstances. When growing up amidsocial disorder, they are likely to internalize prob-lem behaviours, including aggression and substanceabuse.27Factors that can mitigate the impact of such anenvironment include social support, group belonging,stable emotional relationships with parents and rela-tives, a sense of self-efficacy, access to education andacademic support. In addition, opening public spacesto children can foster interaction between adults,enhancing social cohesion.
Host to diverse peoples, cities spur social and culturalexchange, creating opportunities for children to expe-rience diversity. Immigrants make up a great share ofsome of the world’s cities. More than half the residentsof Miami, United States, were born abroad, as were
nearly half of those living in Toronto, Canada, andaround a third of those in Sydney, Australia; Abidjan,Côte d’Ivoire; Singapore; London, United Kingdom;and New York, United States.28Unfortunately, theurban experience can be alienating, particularly ifnewcomers or indigenous groups are not in a position toshape urban spaces according to their needs. Planningdecisions must be sensitive to cultural diversity andshould cater to each group’s preferences for housing,land use, facilities, services and transportation.29
TechnologyAlthough not equally accessible to all, information andcommunications technology (ICT) is especially impor-tant in the lives of those born after 1980. Often termed‘digital natives’,31these young people are employingtechnology in most areas of their lives – in the class-room, on the street and in the home.32Young people all over the world are harnessing thepower of ICT to improve city life. For example, some areusing social networking sites or community websitesto help run carpools and thereby reduce vehicu-lar traffic and its attendant ills. ICT can also beused to prevent violence. For example, computer-aided mapping of the urban environment helpsprotect and empower young people and allowsthem to remain safe by keeping in touch throughtheir social networks. While narrowing the ‘digitaldivide’ that separates technological haves and have-nots is a challenge, so is ensuring the physical andpsychological safety of children and young peoplein the face of online exploitation, cyber-bullying,invasions of privacy and Internet addiction.33
Culture and artsArticle 31 of the Convention on the Rights of the Childstates that children should “participate fully in culturaland artistic life.” Urban areas, as heterogeneous placesof contrast, plurality and interaction, in general provideopportunities for cultural exchange and entertain-ment for both children and adults. While schools oftenserve as the gateway to the arts, the community alsoprovides a platform for cultural life. Where childrenof different backgrounds live side by side, municipalgovernments and civil society are given an opportu-nity to embrace and promote diversity by, for example,creating sections related to each of the cultural groupsin local libraries or by guaranteeing the use of publicspaces for celebrations, festivals and parades.To promote integration, Singapore’s OnePeople initia-tive assists underachieving students from lower-incomefamilies and strengthens bonds between children fromdifferent backgrounds – for instance, by promptingchildren to reflect on the experience of living in themultiracial and multicultural city-state.30
� UNICEF/NYHQ2011-0622/Marta Ramoneda
Adolescents take a photograph with a mobile phone in a cafe inTunis, Tunisia.
EM28BAFebr RGua Ory ED2012
Take Back the Tech! campaigns use technology toraise awareness about violence against women. Overthe course of the 16 Days of Activism against GenderViolence (25 November–10 December), people – espe-cially girls and women – are encouraged to use mobilephones, digital cameras, websites and blogs to opposegender-based violence. In 2009, the campaign wasactive in 24 countries and 12 languages, using audio-casts in Malaysia, tweets in Mexico and chat relays inBrazil to spread its message.34The Amagezi Gemaanyi Youth Association in Ugandais a grassroots NGO that uses technology to empowerchildren and young people in the slums of Kampala.In addition to providing tuition in bookkeeping andmarketing, the community centre in Nabulagalatrains young people aged 12−25 to operate profes-sional sound equipment and recording software inits solar-powered recording studio. Its after-schoolprogramme teaches children to use film and photog-raphy to tell their own stories and raise awareness oftheir situation.
Towards cities fit for children
63
FOCUS ON
UPGRADING INFORMALSETTLEMENTS IN JEDDAHOne of the biggest obstacles todeveloping slum infrastructure is the lackof formal land ownership. In Jeddah,the authorities are addressing this chal-lenge through the Jeddah without Slumsprogramme. Since 2007, this effort hasbeen overseen by a public-private part-nership, the Jeddah Development andUrban Regeneration Company (JDURC),formed specifically to facilitate legaliza-tion of land titles, improvement of localenvironments and increased provision ofservices for residents.include physical changes to buildingsand the public realm to improve struc-tural soundness and comfort, or theprovision of social infrastructure (such asschools and clinics) and utilities (water,energy and sewerage). In each case,care is taken to minimize the disruptioncaused by the construction process.Each plan contains interchangeableoptions that involve greater or lesserdegrees of change to the physicalfabric. This allows the upgrading plan torespond to different levels and combi-nations of official, private-sector andcommunity commitments of financial andpolitical capital. Higher levels of fund-ing allow a more complete upgradingof buildings, public realms, social infra-structure and utilities. Lower levels meanthe focus will be less on individual build-ings and more on shared public services(see Figure 4.3). During all stages ofdevelopment, consultations are held withlocal residents, municipalities, traditionalrepresentatives, developers and JDURCto ensure that stakeholders are engagedand included in the upgrading process.Child rights, unfortunately, are not alwaysat the forefront of urban planning and– as inclusive as these stakeholderconsultations seek to be – more needs tobe done to listen to children’s voices. Theperception seems to be that conditionsadequate for adults are sufficient for all.However, it is important not to treat chil-dren as a homogeneous group. Girls andboys of different ages use urban spacein diverse ways, respond to it differently
Jeddah’s 50-plus unplanned settlementsoccupy around 16 per cent of the city’sarea and house more than 1 millionpeople – one third of its population.Inhabitants often lack sanitation, propershelter and secure tenure, and they alsoexperience inequality in the allocation ofsocial services and amenities. Despitethe challenges, these neighbourhoods doprovide opportunities to prosper. Manyresidents are migrants who join the exist-ing communities by setting up smallbusinesses or working in the serviceindustries that support the local andregional economies.
64
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012In their joint work, the Municipalityof Jeddah, JDURC and Space Syntaxhave sought to address a wide rangeof conditions by combining scientificmeasurement, spatial analysis andphysical intervention with communityengagement and cultural considerations.Each settlement is studied, using theurban planning technique of spatiallayout analysis, to understand how itsproblems are related to the streets, pathsand other routes that knit it togetherand link it to the wider city. Many infor-mal settlements are poorly connected.This complicates residents’ attempts tomake use of opportunities in other partsof the city and can lead to or reinforceeconomic exclusion, social segregationand stigmatization. Overcoming theseproblems involves the creation of newphysical connections and the redesignof existing ones.An upgrading plan is developed for eachneighbourhood based on its unique situ-ation and needs. These needs might
Informal settlements pose a complexquestion: how best to formalize theirunofficial existence, legalize makeshifthomes and provide them with appropri-ate infrastructure and services? Often,such settlements have simply been relo-cated. But UN-Habitat, recognizing thatsocio-economic networks have takenroot in these areas, identifies partici-patory slum upgrading as one of thepreferred strategies for achieving citieswithout slums. This kind of slum upgrad-ing is an extremely complicated task andis truly participatory and effective onlywhen it incorporates the needs of chil-dren – because communities that workfor their youngest members tend to workfor everyone. Space Syntax Limited, anurban planning and design consultancyaffiliated with University College London,has developed an evidence-based, partic-ipatory approach to upgrading informalsettlements in Jeddah, SaudiArabia.
Figure 4 .3 . Design scenarios for an informal settlement, showing the scale of change from maximum(high-level funding) to minimum (low-level funding) intervention
Source:Reproduced courtesy of Space Syntax Limited.
EM28BAFebr RGua Ory ED2012High-levelfundingMid-levelfundingJeddah’sinformalsettlementsLow-levelfunding
and may have varying preferences andconcerns regarding safety, participation,privacy and other factors. For example,small children might be happiest whenthey can play close to their caregiversin small spaces, but older ones will needlarger spaces for activities such as ballgames. Reconstruction presents anopportunity to provide children and theirfamilies with control over planning andbuilding their environment in a way thatworks for them. Specific spatial designelements that need careful consideration
by planners and input from children andtheir families include health and safetyfeatures and accessibility.One way to facilitate children’s partici-pation as stakeholders is to ask them tocollect information about their surround-ings. Again, differing preferences mustbe considered. Some girls may be reluc-tant or unable to voice their opinionsin a meeting where boys, men or evenolder women are present, for example.Children and their families can also be
included in core planning groups, wherethose most interested in the developmentof their area can represent their commu-nity and take part in decision-making.Placing children’s rights at the heart ofurban policymaking, budgeting and plan-ning would ensure that new proposalsand completed projects are judged bytheir impact on children’s lives.
by Tim StonorManaging Director, Space Syntax Limited.
Towards cities fit for children
65
CHAPTER
5
EM28BAFebr RGua Ory ED2012� UNICEF/NYHQ2006-2457/Giacomo Pirozzi
This edition ofThe State of the World’s Childrenhassought to shed light on the experience of children andyoung people in urban areas, especially the poorestand most marginalized. It has covered issues as diverseas sanitation, gangs and governance. And it has takenin the broad sweep of global trends and focused in onindividual, concrete examples of positive practices inspecific urban neighbourhoods. Throughout, it hasbeen concerned about disparity and the harm it doesto the youngest members of the human family.Hundreds of millions of children and young people livein the same cities as political, cultural and commercialelites – yet they struggle to subsist. Too many spendtheir days picking through rubbish for something tosell or making bricks for other people’s homes. Theyspend their nights in makeshift dwellings under threat
EM28BAFebr RGua Ory ED2012
Uniting forchildren in anurban world
of eviction or on the street, where they are at risk ofviolence and exploitation. Moreover, they are deniedtheir right to take part in decisions affecting them.Instead, they are excluded from the process of findingthe solutions that could improve their lives and thoseof countless others.
Mainstream approaches to development often view allchildren in urban areas as a homogeneous group anduse statistical aggregates to determine resource allo-cation and programming actions. An equity-focusedapproach is needed to direct solutions precisely tothose children who are hardest to reach. It is time todo things differently: to live up to the commitmentsof the Millennium agenda by ensuring that marginal-ized children in urban centres receive greater attentionand investment.
Uniting for children in an urban world
67
This chapter explores five key areas in which actionis required if the needs and rights of nearly half of theworld’s children – namely, those who reside in urbanareas – are to be fulfilled. These are: understanding thescale and nature of urban poverty and exclusion; iden-tifying and removing the barriers to inclusion; puttingchildren first within a broader pursuit of equity in urbanplanning, infrastructure development, governance andservice delivery; promoting partnerships between theurban poor and their governments; and ensuring thateveryone works together to achieve results for children.
Expanding the collection of reliable and detailed urbandata in international household surveys and nationalstatistical processes will be vital to gaining deeperinsights into the reality of urban life for children.Additionally, research on specific neighbourhoodsand households should be conducted more frequentlyin order to capture the shifting and diverse nature ofurban habitats.Information is useful only if it is shared, so data must bedisseminated widely and analysed in ways that exposecausality and enable effective responses to inequalityand exclusion. Such initiatives are under way, notablythe analysis of National Family Health Survey (NFHS)findings in urban areas in India, and the World Bank’sasset-based interrogation of Demographic and HealthSurveys (DHS).1Nevertheless, more needs to be done tounderstand how poverty evolves and affects children inurban environments – and why it persists from gener-ation to generation. This will require not only soundstatistical work but also relevant research and evalua-tion of interventions intended to address these problems.
Understand urbanpoverty and exclusionReliable data and analysis highlighting the spectrum ofurban realities is essential if those children with the great-est needs are to be reached. National and internationalsurveys do not always include children and families onthe urban margins, who may lack official status and havelimited access to available services. Gathering accurate,disaggregated information should be the starting pointfor creating equitable, child-focused urban policies.To begin with, a practical definition of what constitutesan urban area is needed if the particular problemsfaced by children in urban areas are to be identifiedcorrectly. Existing definitions vary greatly, complicatingcomparative analysis.
EM28BAFebr RGua Ory ED2012
Next, the tools of data collection must be honed so theymore precisely reflect disparities in children’s needs andthe realization of their rights based on wealth, gender,ethnicity, disability or neighbourhood. Determiningwhich children and families are most at risk of exclusionmay also require measures that highlight populationscommonly omitted in surveys. One such technique isoversampling, or the deliberate inclusion of a higherproportion of individuals or families who wouldotherwise be undercounted or overlooked in standardrandom samples of the general population. Sample sizesneed to be large enough for the various urban cohorts tobe meaningfully compared; it may be necessary to over-sample in slum areas, for example, to make such compar-isons possible. In addition, mapping and spatial analysis– for instance, linking specific urban areas with partic-ular health outcomes – can help target at-risk groupsand identify priority areas for service and investment.
A boy stands on railroad tracks in Kibera, a slum area of Nairobi, Kenya,as fires smoulder in the background. Over a quarter of the city’s populationlives in Kibera. The train does not stop there.
68
THE STATE OF THE WORLD’S CHILDREN 2012
� UNICEF/NYHQ2006-1768/Michael Kamber
FOCUS ON
THE PAUCITY OFINTRA-URBAN DATAWhere there is demand to incorporateurban slums into more surveys, design-ers can do so.The difficulty of defining ‘urban’ and‘slum’ poses another challenge. Nationalcriteria may not be fully transparent ormay have changed over time. Definitionsvary. Urban areas may be defined byadministrative jurisdictions (e.g., munici-palities), athreshold population size and/or density, or socio-economic conditions.The challenge of obtaining reasonableslum estimates is further complicatedwhere slums are considered illegalsettlements by national governments.measured byconsumer durables andhousing quality.This means that if effortsto reach the poor focus exclusively onslum areas, many poor households willbe excluded.Finally, some of the most vulnerableand marginalized – children living on thestreet or in institutions, or those engagedin child labour – are often excluded fromthe sample frame. Capturing the locationand situation of these children remains amajor challenge for international house-hold surveys.Experience indicates that showing thefull spectrum of urban realities willrequire, at a minimum:
Urban households – rich and poor –are often grouped together to providea single average estimate of nationalurban poverty or malnutrition. This canbe particularly misleading in countriescharacterized by high social and incomeinequality. Such averages mask thedifferences between cities and withinurban communities whose residents havevastly divergent living standards.Available population-based data setsmay not lend themselves to further disag-gregation at the urban level becausesample sizes are often too small. In addi-tion, although slum areas are generallyincluded in census sample frames, theyare seldom identified as slums.
Cost is a consideration. In order to obtainreliable estimates for slum areas, samplesizes would have to be increased signifi-cantly. Introducing additional categoriesof sampling (e.g., urban slums) to a surveyincreases its size and cost. But biggersurveys are not always better surveys.Keeping sample sizes down to manage-able levels can yield data of higher qualityas it enables survey managers to monitorprogress and better train and supervisefield staff who collect the data.
EM28BAFebr RGua Ory ED2012Urban-rural comparisons can also provemisleading. If assessed against a nationalwealth index, few urban residents arelikely to fall in the poorer quintiles, orfifths, of the population, concealing thefact that while incomes may be higherin urban areas, so is the cost of living(rent, food, transport and basic services,for example). Many standard indica-tors, such as those relating to stunting oraccess to water and sanitation, are notreadily comparable between rural andurban households. In a city, for instance,access to a reliable source of cleanwater may entail higher costs andlonger queues.While it is important to capture urbanslum data, it should be emphasizedthat not all poor households are foundin slums – and not all slum residentsare poor. In fact, a 2005 study of 85Demographic and Health Surveys (DHS)found that 1 in 10 of a poor household’sneighbours was relatively affluent, as
Reliable statistics can help illuminatethe plight of poor and marginalized chil-dren in urban settings – after all, it isdifficult to argue with facts. However,this seemingly straightforward processis hampered by the limited availabil-ity of urban data that are meaningfullydisaggregated – by wealth, residence,gender, ethnicity, city size or otherrelevantcriteria.
• Political will to establish urban data as a priority amongcompeting interests• Collaboration among agencies tocollect, analyse and disseminatethese data• Clear definitions of ‘urban slums’ that reduce conceptual confusion andenable meaningful comparison• Oversampling in slum areas to gathersufficient data for stratified analysis• Making sure no slum has been overlooked, for example, by usingsuch tools as GeographicInformation Systems• Going beyond national averages and rural-urban comparisons toanalyse and document disparitieswithin urban areas• Devising new wealth indices that facilitate analysis and comparison ofdisparities within and between urbanand rural areas.
Uniting for children in an urban world
69
Remove the barriers to inclusionImproved understanding of exclusion must lead to theidentification and dismantling of barriers that preventimpoverished children and their families from usingservices and enjoying such core elements of citizen-ship as legal protection and security of housing tenure.Service delivery will be a vital part of the response, butthe essential problem remains that exclusion consistentlyundermines the capacity to secure children’srights.A starting point is to determine the bottlenecks andbarriers in each urban setting and to review theevidence on proven strategies to overcome them. Manyfactors, such as household income poverty, direct andindirect service costs, poor transportation and lackof official identification documents, serve to excludethe urban poor. Experience shows that service cover-age for the poorest can be enhanced by abolishing userfees, setting up community partnerships, using masscommunication and other strategies.
One reason such initiatives hold promise is that theybalance greater supply of services with measures toenhance demand and utilization. Expanding the supplyside (i.e., commodities, facilities, human resources),while necessary to extend health and nutrition services,is not enough to ensure effective coverage of suchservices among the poorest children and families.Effective supply-side measures must be complementedby demand enhancements that promote knowledgeand take-up of services, continuity of use and assuranceofquality.Increased social protection also can have a markedimpact in overcoming the financial barriers thatexclude the urban poor. Conditional cash transfersto poor families, often in urban settings, have provedsuccessful in a number of Latin American and Africancountries.2Mobile services are another creative possi-bility; in Washington, D.C., mobile health clinics assistchildren and adolescents who lack proper accessto comprehensive paediatric health care in the city’sunderserved communities.3
EM28BAFebr RGua Ory ED2012
A 14-year-old girl stands on the balcony of a hostel in Benghazi, Libya. Following armed conflict that also displaced her family in 2011, the city’s schoolswere closed and adolescent girls had few recreational opportunities.
70
THE STATE OF THE WORLD’S CHILDREN 2012
� UNICEF/NYHQ2011-0956/Marta Ramoneda
� UNICEF/NYHQ2009-1786/Susan Markisz
Children in Moravia, a low-income neighbourhood in Medellin, Colombia.
Promoting knowledge and use of available servicesamong target populations is also vital. Since 2002, forexample, the Global Equity Gauge Alliance has chal-lenged urban health inequities through outreach andcommunity engagement in a number of countries. InCape Town, South Africa, for example, residents andhealth workers are involved at every stage of the proj-ect, which entails reallocating health staff, runninghealth promotion programmes in schools and provid-ing dry toilets in informal settlements.4
The agenda must encompass not only services butalso protection. Violence, in all its forms, is a commondenominator in the poorest and most marginalizedneighbourhoods. It is increasingly and accuratelyviewed by the international community as a majorthreat to the rights and well-being of all, especiallychildren and women. Efforts are being made to tackleviolence as an international issue, as evidenced bySafe and Friendly Cities for All, a joint initiative ofUN-Habitat, UN-Women and UNICEF that aims todevelop municipal prevention strategies with a strongfocus on participation. Through such measures aslegislation and policy, training, mass media campaigns,activism and budget review, it engages women, children
EM28BAFebr RGua Ory ED2012
and their communities, the police, town plannersand policymakers in fighting gender-based violence.Promising national initiatives are also under way, nota-bly in Latin America. In Guatemala, for example, theCEIBA programme aims to provide young people withan alternative to drugs and a way out of violence bytraining them in job skills that are in local demand.Safe public transport and well-regulated traffic arevital components of a city fit for children. Road acci-dents kill more of the world’s young people than anyother single cause. Successful initiatives in Colombia,Sweden and the Netherlands have combined car-freeareas, dedicated bicycle and pedestrian routes, andpublic transport to reduce injuries and deaths.Ensuring that all children are registered and docu-mented must be a top priority because, however ardentthe efforts to promote equity, it likely will elude chil-dren who lack official documents. About a third of allchildren in urban areas go unregistered at birth, andthat proportion is closer to 50 percent in sub-SaharanAfrica and South Asia.5
Uniting for children in an urban world
71
PERSPECTIVE
HOME-GROWNSOLUTIONSby Celine d’Cruz and Sheela Patel,Shack/Slum Dwellers International
One of the more promising developmentsin the effort to reduce urban poverty isthe emergence of networks of grassrootsgroups in which women play a prominentrole as agents of positive change in theircommunities and around the world.We have had the privilege of workingwith one such network – Shack/SlumDwellers International (SDI) – sinceits inception in 1996. There are similarnetworks of street vendors, home-basedworkers and waste pickers.
women form collectives to pool savingsand make loans to one another so theycan put food on the table, buy medicines,get transport to find jobs and pay for chil-dren’s education. In time, they examinetheir environs and identify what they need.At the top of the list of needs is securityof tenure. Children need a decent placeto live, places to play and neighbour-hoods in which they feel safe. They needclean water and toilet solutions that donot force two-year-olds to stand in lineor expose adolescent girls to harass-ment. Security of tenure makes it easierto fulfil these needs. It also frees childrenfrom the stress and lost opportunitiesthat come with the ever-present threatof being forcibly evicted or having theirhomes demolished. Insecurity of tenuremeans that women and children mustwork near their dwellings so they areclose at hand in case of eviction. Childrenserve as ‘road runners’, warning parentsand neighbours when a demolition squadhas been sighted; as their homes aredestroyed, they scramble to protectwhatever they can from being taken bythe police. Living in constant fear of evic-tion erodes whatever resources a familyhas. But when secure tenure is negoti-ated, children start going to school, andparents feel more confident about invest-ing in proper shelter.Here, too, the experience of grassrootsnetworks is instructive. An essentialelement of SDI’s work is making whatwas invisible hard to ignore. Cities oftenhave no data recording the presence of
We believe that unless we band together,the challenges of urban poverty will notbe addressed. By joining forces andpooling our knowledge, experience andcreative solutions, we can achieve actionon a meaningful scale. So it is that slumdwellers in such cities as Nairobi, Kenya,and Kampala, Uganda, are consult-ing counterparts in Mumbai, India, whopersuaded government, railway author-ities and international developmentlenders to relocate some 20,000 house-holds as part of an effort to update therail system. Ultimately, the Mumbai slumresidents were able to design their ownresettlement, moving from locations wheremany children had been killed by trainspassing a mere 9 metres fromhomes.SDI has hundreds of thousands offederated members in cities spreadacross 34 countries. They work for decenthousing and infrastructure, usually seek-ing to collaborate with local government.This takes years of organizing, mobilizingand building relationships. It begins when
Sheela Patel chairs the board of SDI. She works with the Indian non-governmental organizations Mahila Milan, the National Slum Dwellers Federation andthe Society for the Promotion of Area Resource Centres (SPARC), which was established in 1984 to address issues faced by the pavement dwellers ofMumbai. Celine d’Cruz is the coordinator of SDI. A founder of SPARC, she began working for the rights of pavement and slum dwellers in India in the early1980s, helping impoverished women in Mumbai bargain collectively to bring housing, education and health services to their families.
72
THESTATE OF THE WORLD’S CHILDREN 2012STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
people living ‘illegally’ on pavements, underbridges and on waste land. These residentsare not counted in the census; they areexcluded from voting lists; and their chil-dren’s births are not recorded. But whentheir presence is documented throughsettlement profiles and family identifica-tion papers, it becomes clear that theyare gainfully employed, contribute to thecity’s economy and are worthy of citizen-ship. Because such documentation alsoidentifies the children in each household,it becomes possible to determine howmany need immunization and schooling,how many work and what kind of workthey do. In addition to being our basicorganizing tool, this process of enumer-ation enables negotiation for tenure andservice provision. The process yieldsanother benefit for children–seeingparents, especially their mothers, nego-tiate collectively to improve lives andsurroundings is a vital part of children’ssocialization.Clearly, these networks cannot solvethe problems of all children. But theyare important allies in the endeavour tosafeguard child rights, and they under-take critical foundational work to makechildren’s homes and neighbourhoodssafe and secure. They can bridge thegap between the formal urban develop-ment world and poor urban communities,promoting solutions that work for theirmembers. We know from our work thatpoor communities are fed up with otherssetting development priorities for them.True alliances and partnerships meanmaking choices together.
� UNICEF/NYHQ2005-1199/Roger LeMoyne
Clearly, urban governance needs strengthening so thatit is more capable of delivering policies and servicesthat benefit and safeguard the rights of children. Toomany city governments pander to vested interests andare too readily prepared to accept the status quo, whichoften involves vast, unplanned informal settlementsthat fail to meet people’s needs. There is a manifestneed to enhance accountability.Moreover, city governments need to ground urbanplanning and programming in a commitment to equityand human rights. One hallmark of this commitment isthe involvement of grassroots organizations in design-ing and monitoring implementation of urban policiesand programmes. Participatory approaches can createsustainable solutions; communities’ and children’sperspectives are often invaluable in improving urbanplanning and design. Take the example of CLEAN-Delhi, a joint advocacy initiative of NGOs andschoolchildren in New Delhi, India. Launched in 1996in the face of rising waste, emissions, traffic and pollu-tion, CLEAN is credited with persuading policymakersto invest in composting and recycling units, permanentwater and air monitoring systems and water filtra-tion systems at schools and municipal water treatmentplants. Following its initial success, the programme hasbeen expanded to other Indian cities.Similarly, recovery from natural disasters requiresplanning tailored to the needs of children in urbansettlements. Two evaluations assessing the responseto the 2010 earthquake in Haiti highlight the need todo better at matching humanitarian interventions withthe specific needs of children in urban settlements. Onestudy found that agencies had not been prepared wellenough for the urban character of the disaster and as aresult had failed to tailor their responses to the urbanenvironment.6A separate review found that water,sanitation and hygiene interventions would have beenmore cost-effective had they been based on a betterunderstanding of the urban topography, its residentialpatterns and the needs and behaviours of the urbanpopulation – including children.7
Girls attend a school in the Kucukbakkalkoy neighbourhood of Istanbul,Turkey, that offers remedial classes for Roma children who may havemissed out on regular educational opportunities.
Put children firstChildren’s well-being is determined, in no smallmeasure, by their environment. Their particular needsand priorities must be incorporated into efforts toimprove housing, infrastructure, safety and gover-nance. It follows that the work of local governmentand urban planning must be carried out with explicitrecognition of the rights of children and young people,and with greater attention to age andgender.This will entail a wider frame of reference for urbandevelopment that accommodates and reduces risksto children of all ages and needs, from infants andtoddlers to adolescents, children with disabilities andthose who do not attend school.
Ensuring that the urban poor have adequate housingand secure tenure must be a priority. Among its othersocial benefits, decent housing can protect childrenand families living in densely populated urban settingsagainst many injuries, accidents and diseases.
Sound policies combine action to improve and expandhousing for the urban poor with extension of services.Brazil’s Minha Casa, Minha Vida (My Home, MyLife)programme, for example, aims to build 3 millionhomes in five years while prioritizing social provi-sion for the poor through education, conditional cashtransfers and job creation.
EM28BAFebr RGua Ory ED2012
Uniting for children in an urban world
73
Promote partnershipwith the urban poorThe challenges of poverty and inequity within mosturban areas demand active partnership between theurban poor and government. Local authorities andcommunities will need to coordinate efforts so thatlimited resources are used most efficiently and equi-tably; so that the efforts and painfully accumulatedassets of the poor are built on, not undermined; andso that people living in poverty – often the major-ity of the population – are included in broader urbandevelopment andgovernance.The voice and involvement of children and adolescentscan be an important aspect of this partnership but, alltoo frequently, child participation becomes a matter oftokenism. Examples from around the world show themany benefits, for both children and policymakers, ofencouraging representation at the municipal level. Infour South American cities, a multi-stage, long-termprocess of urban consultation with local governmentshas led to safer and more equitable cities. Positiveoutcomes include improvements to public infrastruc-ture in Rio de Janeiro and Sao Paulo, Brazil; higherliteracy rates in Cotacachi, Ecuador; and expandedbirth registration in Ciudad Guayana, BolivarianRepublic of Venezuela.
programming. In Johannesburg, South Africa, 10- to14-year-olds in low-income neighbourhoods succeededin identifying risky areas of their city and proposingviable improvements.8Such mapping exercises can help communities comeup with ways to provide for play and leisure, whichare children’s rights and essential to their development.With modest material support from local government,for example, residents can create small play spacesbetween residences. Such settings allow parents andcaregivers to be nearby.Where municipal authorities do not have sufficientcapacity, community-based organizations and NGOscan also play a part. Examples include Kilikili, anorganization in Bangalore, India, that creates greenplay spaces and involves children, including those withspecial needs, in the design process.
The international Child-Friendly Cities Initiative hassucceeded in putting child rights on the urban agenda.To be awarded child-friendly status, a city must showthat it fosters child participation and pursues childrights through its strategy, legislation, budgeting,impact assessments and public awareness programmes.The scheme has great potential for expansion,particularly in rapidly growing, rapidly urbanizingmiddle-incomecountries.
Children and adolescents should be encouraged tobecome involved in projects to improve their cities.Their participation gives them an empowering chanceto air their views and engages them in understandingurban development and respecting their environment.Successful projects, such as Map Kibera in Nairobi,Kenya, have shown how adolescents can assist in gener-ating an effective base of knowledge for development
74
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
There is more at stake here than ‘child’s play’. Publicplay spaces can help mitigate overcrowding and lackof privacy in the home and enable children to mix withpeers of different ages and backgrounds. This earlyexperience of diversity can add to the foundations ofa more equitable society.9Moreover, a large body ofevidence shows that exposure to trees, water and thenatural landscape benefits children’s physical, mentaland social well-being.10
Work together to achieveresults for childrenThe projects and programmes discussed in this reportoffer only a glimpse of what is being done to ensureequitable access to services and protection. Takentogether, they provide a sense of what can happenwhen children’s rights are placed at the centre of theurban agenda in active partnership with communities.Under any circumstances, but especially in these strait-ened times, actors at all levels – from the local to theglobal – and from civil society as well as the publicand private sectors need to pool their resources andenergies to create urban environments conducive tochildren’s rights.
� UNICEF/NYHQ2010-1854/Shehzad Noorani
A boy reads in his bed in Kuleana, a centre for boys who work on the streets, in the city of Mwanza, United Republic of Tanzania.
Non-governmental organizations and internationalagencies can play a crucial part in fostering theengagement of children in municipal governance andcommunity decision-making. Local communities andauthorities must engage each other if children’s rightsare to be realized. In addition, such cross-borderissues as migration and trafficking demand urgentcoordinated action.
International partnerships among civil society orga-nizations can tap into the power of their constituentorganizations to further children’s interests and linkcommunities around the world. Shack/Slum DwellersInternational provides one example. This networkbrings together grassroots federations of the urbanpoor – many led and sustained by women – that addresstenure, housing and basic infrastructure problems.These networks facilitate exchange among marginal-ized communities across the globe and serve as bridgesbetween these communities, local and national author-ities and internationalagencies.Policies and actions that involve urban areas anddifferent levels of government require greater coordi-nation. Dealing with urban violence affecting children,for example, requires collaboration to address local
EM28BAFebr RGua Ory ED2012Towards fairer cities
and national political and economic realities, influencecultural norms and attitudes, and re-establish trustamong authorities, institutions and the generalpublic.Civil society organizations, and particularly commu-nity-based organizations, should be embraced in urbanprogramming and governance, as they play a criticalpart in enabling local communities to influence policy.
More than half the world’s people already live in townsand cities and, increasingly, children are growing upagainst an urban backdrop. Their urban childhoodsreflect the broad disparities that cities contain: richbeside poor, opportunity beside struggle for survival.Equity must be the guiding principle in efforts forall children in urban areas. The children of slums– born into and raised under some of the most chal-lenging conditions of poverty and disadvantage – willrequire particular attention. But this must not comeat the expense of children elsewhere. The larger goalmust remain in focus: fairer, more nurturing cities andsocieties for all people – starting with children.
Uniting for children in an urban world
75
REFERENCESCHAPTER 11 Baker, Judy L.,Urban poverty: A global view,Urban papers, The World Bank, Washington, D.C.,2008, p. 1.2 World Health Organization and United NationsHuman Settlements Programme,Hidden Cities:Unmasking and overcoming health inequities inurban settings,WHO, Geneva, 2010, p. ix.3 Stephens, Carolyn,Urban Social andEnvironmental Inequities: Impacts on childrights, health and wellbeing in cities,UNICEFBackground Discussion Paper forState of theWorld’s Children 2012,2011, p. 2.4 United Nations,World Urbanization Prospects:The 2009 revision,Department of Economic andSocial Affairs, Population Division, United Nations,New York, 2010; World Health Organization andUnited Nations Human Settlements Programme,Hidden Cities: Unmasking and overcoming healthinequities in urban settings,WHO, Geneva,2010, p. 5.5The 2009 revision,p. 5.6 Chen, Nancy, Paolo Valente and Hania Zlotnik,‘What Do We Know about Recent Trends inUrbanization?’, inMigration, Urbanization andDevelopment: New directions and issues,edited by Richard E. Billsborrow, United NationsPopulation Fund, New York, 1998, pp. 59–88;United Nations Population Fund,State of WorldPopulation 2010: Unleashing the potential ofurban growth,UNFPA, New York, 2007 p. 13.,10 United Nations Human Settlements Programme,State of the World’s Cities 2006/7: The MillenniumDevelopment Goals and urban sustainability– 30years of shaping the Habitat agenda,UN-Habitat, Nairobi, 2006, p. 14.12 Khan, Khalid S., et al., ‘WHO Analysis of Causesof Maternal Death: A systematic review’,Lancet,vol. 367 no. 9516, 1 April 2006, pp. 1066–1074,,as cited in Ziraba, Abdhalah K., et al., ‘MaternalMortality in the Informal Settlements of NairobiCity: What do we know?’,Reproductive Health,vol. 6, no. 6, May 2009, pp. 1–8.13 Ziraba, ‘Maternal Mortality’; ‘Trends inMaternal Mortality’.14 ‘Understanding Urban Inequalities in Bangladesh’;Montgomery, ‘Urban Poverty and Health inDeveloping Countries’; Ziraba, ‘Maternal Mortality’.15 Ruel, Marie T., James L. Garrett and LawrenceHaddad, ‘Rapid Urbanization and the Challengesof Obtaining Food and Nutrition Security’, inNutrition and Health in Developing Countries,2nd ed., edited by Richard D. Semba andMartinW.Bloem, Humana Press, Totowa, N.J.,2008, p.646.16 Fotso, ‘Child Health Inequities in DevelopingCountries’, p. 2; Van de Poel, Ellen, OwenO’Donnell and Eddy van Doorslaer, ‘Are UrbanChildren Really Healthier? Evidence from 47developing countries’, Tinbergen InstituteDiscussion Paper TI 2007-035/3, TinbergenInstitute, Amsterdam, 2007 <www.tinbergen.nl/,discussionpapers/07035.pdf>, accessed 8 August2011; United Nations, Background paper for theInteragency Meeting on Urbanisation in New Yorkon 6 March 2007 United Nations, New York, as,cited in Harpham, T., ‘Urban Health in DevelopingCountries: What do we know and where do wego?’,Health & Place,vol. 15, no.1, March 2009,pp. 107–116.17 HarvestPlus, ‘Nutrients: What is hidden hunger?’,<www.harvestplus.org/content/nutrients>,accessed 4 September 2011.18 Van de Poel, O’Donnell and van Doorslaer, ‘AreUrban Children Really Healthier?’; Fotso, JeanChristophe, ‘Urban-Rural Differentials in ChildMalnutrition: Trends and socio-economic corre-lates in sub-Saharan Africa’,Health & Place,vol. 13, no. 1, March2007 pp.205–223,,<http://irnegotiation0708.pbworks.com/f/download+malnutrit.pdf>, accessed30September 2011; Kennedy, G., et al.,‘Does Living in an Urban Environment ConferAdvantages for Childhood Nutritional Status?Analysis of disparities in nutritional status bywealth and residence in Angola, Central AfricanRepublic and Senegal’,Public Health Nutrition,vol. 9, no. 2, April 2006, pp. 187–193, <http://bvs.per.paho.org/texcom/nutricion/ango.pdf>,accessed 30 September2011.19 Fotso, ‘Child Health Inequities in DevelopingCountries’, pp. 9–10.20 Ibid., p. 2.21 Menon, Purnima, Marie T. Ruel and Saul SutkoverMorris, ‘Socioeconomic Differentials in ChildStunting Are Consistently Larger in Urban Thanin Rural Areas’, FCND Discussion Paper No. 97,International Food Policy Research Institute,Washington, D.C., October 2000, pp. 282–289;Montgomery, ‘Urban Poverty and Health inDeveloping Countries’, p. 6.
CHAPTER 21 Smith, Terry, and Laura Brownlees, ‘AgeAssessment Practices: A literature review andannotated bibliography’, Discussion paper, ChildProtection Section, United Nations Children’sFund, New York, 2011, p. 1.2 Habib, R. R., et al., ‘Housing Quality and IllHealth in a Disadvantaged Urban Community’,Public Health,vol. 123, no. 2, February 2009,pp.174–181.3 United Nations Human Settlements Programme,‘The Habitat Agenda: Istanbul Declarationon Human Settlements’, June 1996,<www.unhabitat.org/downloads/docs/2072_61331_ist-dec.pdf>, accessed4September 2011.
7 Satterthwaite, David, ‘The Under-estimationof Urban Poverty in Low- and Middle-IncomeNations’, IIED Working Paper 14 on PovertyReduction in Urban Areas, International Institutefor Environment and Development, London, 2004;Sabry, Sarah, ‘How Poverty Is Underestimatedin Greater Cairo, Egypt’,Environment andUrbanization,vol. 22, no. 2, October 2010,pp. 523–541; Chandrasekhar, S., andMark R. Montgomery, ‘Broadening PovertyDefinitions in India: Basic needs in urban hous-ing’, IIED Working Paper, International Institutefor Environment and Development, London, 2010.8 Montgomery, Mark R., ‘Urban Poverty and Healthin Developing Countries’,Population Bulletin,vol. 64, no. 2, June 2009, p. 6, <www.prb.org/pdf09/64.2urbanization.pdf>, accessed5 August 2011.9 Bitran, J., et al., ‘Keeping Health in an UrbanEnvironment: Public health challenges for theurban poor’, inThe Urban Poor in Latin America,edited by M. Fay, The World Bank, Washington,D.C., 2005, pp. 179–194; Fotso, Jean Christophe,‘Child Health Inequities in Developing Countries:Differences across urban and rural areas’,International Journal for Equity in Health,vol. 5,no. 9, 11 July 2006; National Research Council,Cities Transformed: Demographic change andits implications in the developing world,editedby Panel on Urban Population Dynamics et al.,National Academies Press, Washington, D.C.,2003, in Montgomery, ‘Urban Poverty and Healthin Developing Countries’, p. 5; Matthews, Zoe,et al., ‘Examining the “Urban Advantage” inMaternal Health Care in Developing Countries’,PLoS Medicine,vol. 7 no. 9, 14 September 2010.,
76
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED20124 Sverdlik, Alice, ‘Ill-Health and Poverty: A literaturereview on health in informal settlements’,Environment and Urbanization,vol. 23, no. 1,April2011, p. 126.5 Barrett, Julia R., ‘A Marked Disadvantage: Rapidurbanization and mortality of young children inNigeria’,Environmental Health Perspectives,vol.118, no. 5, June 2010, pp. 118–259.6 Slum under-five mortality rate: 95 per 1,000livebirths. See United Nations Children’s FundBangladesh, ‘Understanding Urban Inequalitiesin Bangladesh: A prerequisite for achieving Vision2021 – A study based on the results of the2009 Multiple Indicator Cluster Survey’, UNICEFBangladesh, Dhaka, November 2010, p.13,<www.unicef.org/bangladesh/Urban_paper_lowres.pdf>, accessed 4 September 2011.7 Kyobutungi, Catherine, et al., ‘The Burden ofDisease Profile of Residents of Nairobi’s Slums:Results from a demographic surveillance system’,Population Health Metrics,vol. 6, no.1, March 2008,pp. 1–8, <www.ncbi.nlm.nih.gov/pmc/articles/PMC2292687>, accessed 5 September 2011.8 Montgomery, ‘Urban Poverty and Health inDeveloping Countries’.9 Sims, Mario, Tammy L. Sims and Marino A.Bruce, ‘Urban Poverty and Infant Mortality RateDisparities’,Journal of the National MedicalAssociation,vol. 99, no. 4, April 2007 pp. 349–356;,Centers for Disease Control and Prevention,‘Racial and Ethnic Disparities in Infant MortalityRates: 60 largest cities, 1995–1998’,Morbidity &Mortality Weekly Report,vol. 51, no.15, 2002,pp. 329–332.10 Brown, David, et al., ‘A Summary of GlobalRoutine Immunization Coverage Through 2010’,The Open Infectious Diseases Journal,vol. 5,2011, pp. 115–117.11 World Health Organization, United NationsChildren’s Fund, United Nations PopulationFund and the World Bank, ‘Trends in MaternalMortality: 1990 to 2008 – Estimates developedby WHO, UNICEF UNFPA, and the World Bank’,,WHO, Geneva, 2010, <http://whqlibdoc.who.int/publications/2010/9789241500265_eng.pdf>,accessed 5 August 2011.
22 Agarwal, Siddarth, ‘The State of Urban Health inIndia: Comparing the poorest quartile to the restof the urban population in selected states andcities’,Environment and Urbanization,vol. 23,no.1, April 2011, pp. 13–28.23 Gupta, Kamla, Fred Arnold and H. Lhungdim,Health and Living Conditions in Eight IndianCities,National Family Health Survey (NFHS-3),India, 2005–2006, International Institute forPopulation Sciences and ICF Macro, Mumbaiand Calverton, Md., 2009.24 Kennedy, et al., ‘Does Living in an UrbanEnvironment Confer Advantages?’.25 Ruel, Marie T., and James L. Garrett, ‘Featuresof Urban Food and Nutrition SecurityandConsiderations for Successful UrbanProgramming’,Electronic Journal of Agriculturaland Development Economics,vol. 1, no. 2, 2004,pp. 242–271.26 Popkin, Barry M., ‘The Nutrition Transition and ItsRelationship to Demographic Change’, in Sembaand Bloem,Nutrition and Health in DevelopingCountries,pp. 427–445.27 Ruel, Marie T., et al., ‘The Food, Fuel, andFinancial Crises Affect the Urban and Rural PoorDisproportionately: A review of the evidence’,Journal of Nutrition,vol. 140, no. 1, January 2010,pp. 1S–7S, <http://jn.nutrition.org/content/140/1/170S.full>, accessed 5September2011.28 World Health Organization, ‘Clean HouseholdEnergy for All’, <www.who.int/indoorair/interventions/CHEA_brochure_rev.pdf>, accessed5September 2011; World Health Organization,‘Air Quality and Health’, Fact sheet No. 313,WHO, updated September 2011, <www.who.int/mediacentre/factsheets/fs313/en/index.html>,accessed 30 September 2011.
38 United Nations Children’s Fund, United NationsJoint Programme on HIV/AIDS, United NationsEducational, Scientific and Cultural Organization,United Nations Population Fund, InternationalLabour Organization, World Health Organizationand the World Bank,Opportunity in Crisis:Preventing HIV infection from early adoles-cence to young adulthood,UNICEF New York,,June2011, Table 1, pp. 39, 41.39 Busza, Joanna R., et al., ‘Street-BasedAdolescents at High Risk of HIV in Ukraine’,Journal of Epidemiology and Community Health,23 September 2010, <http://jech.bmj.com/content/early/2010/09/23/jech.2009.097469.full>,accessed 4 September 2011.40 Black, Maureen M., and Ambika Krishnakumar,‘Children in Low-Income, Urban Settings:Interventions to promote mental health andwell-being’,American Psychologist,vol. 53,no. 6, June 1998, pp. 635–646; Patel, V., et al.,‘Promoting Child and Adolescent Mental Healthin Low and Middle Income Countries’,Journal ofChild Psychology and Psychiatry,vol. 49, no. 3,March 2008, pp. 313–334, <www.sangath.com/images/file/Promoting%20child%20and%20adolescent%20mental%20health%20.....pdf>,accessed 30 September 2011.41 Flournoy, Rebecca, and Irene Yen, ‘The Influenceof Community Factors on Health: An annotatedbibliography,’ PolicyLink, Oakland, Calif., 2004,p. 17 <www.policylink.org/atf/cf/%7B97c6d565-,bb43-406d-a6d5-eca3bbf35af0%7D/ANNOTATEDBIBLIOGRAPHY_FINAL.PDF>,accessed 5 September 2011.
52 United Nations Educational, Scientific and CulturalOrganization,EFA Global Monitoring Report 2011:The hidden crisis – Armed conflict and education,UNESCO, Paris, 2011, pp. 40, 43.53 United Nations Human Settlements Programme,State of the World’s Cities 2010/2011: Bridging theurban divide,Earthscan on behalf of UN-Habitat,London and Nairobi, 2008, p. 117.54EFA Global Monitoring Report 2010,p. 176.55EFA Global Monitoring Report 2011,p. 158.56 Tsujita, Yuko, ‘Deprivation of Education: A studyof slum children in Delhi, India’, Paper commis-sioned for theEFA Global Monitoring Report2010,2010/ED/EFA/MRT/PI/12, April 2009, p. 4.57 ‘Understanding Urban Inequalities inBangladesh’,p. 13.58State of the World’s Cities 2006/7p. 122.,59 Duflo, Esther, Pascaline Dupas and MichaelKremer, ‘Poverty Action Lab’, Unpublished study,2008, cited in Bartlett, Sheridan, and DavidSatterthwaite, ‘Urban Poverty and Urban Children:A review of the literature’, UNICEF internalworking paper, United Nations Children’s Fund,New York, p. 60.60 International Labour Office,A Global Allianceagainst Forced Labour: Global report under thefollow-up to the ILO Declaration on FundamentalPrinciples and Rights at Work 2005,ReportI (B), International Labour Conference, 93rdSession 2005, ILO, Geneva, 2005, pp. 14–15,<www.ilo.org/wcmsp5/groups/public/---ed_norm/---declaration/documents/publication/wcms_081882.pdf>, accessed 30 September 2011.61 International Labour Organization,Tanzania:Children in prostitution – A rapid assessment,International Programme on the Elimination ofChild Labour, ILO, Geneva, 2001, p. 15.62 Ali, Masud, et al.,Misplaced Childhood: A shortstudy on the street child prostitutes in Dhakacity,Red Barnet supported by Save the ChildrenDenmark, Dhaka, 1997 in INCIDIN Bangladesh,for the International Labour Organization,International Programme on the Eliminationof Child Labour, and the Trafficking in Children– South Asia Project,Rapid Assessment onTrafficking in Children for Exploitative Employmentin Bangladesh,ILO, Dhaka, February 2002, p. 17.
29 Overseas Development Institute, ‘Livelihoods andGender in Sanitation, Hygiene and Water Servicesamong the Urban Poor’, MailiSaba ResearchReport, ODI, March 2005, pp. 14–15,<www.odi.org.uk/resources/download/2959.pdf>,accessed 5 September 2011.30 Corburn, Jason, ‘Urban Land Use, Air Toxicsand Public Health: Assessing hazardous expo-sures at the neighborhood scale’,EnvironmentalImpact Assessment Review,vol. 27 no. 2,,March2007 pp. 145–160. Low-income neighbour-,hoods with elevated air toxins cited in the studyinclude the South Bronx; Harlem; Greenpoint andWilliamsburg in Brooklyn, New York; Roxbury,Boston; Barrio Logan, San Diego, California; andSouth Baltimore, Maryland.31 World Health Organization,Decade ofAction for Road Safety, 2011–2020: Savingmillions of lives,WHO, 2011, <www.who.int/violence_injury_prevention/publications/ road_traffic/saving_millions_lives_en.pdf>, accessed30September 2011.32 World Health Organization,Global StatusReport on Road Safety: Time for action,WHO,Geneva, 2009, <http://whqlibdoc.who.int/publications/2009/9789241563840_eng.pdf>,accessed 30 September 2011.33 UNAIDS estimates, 2011.34 Ibid.35 Garenne, Michel, ‘Urbanization and Child Healthin Resource-Poor Settings with Special Referenceto Under-Five Mortality in Africa’,Archives ofDisease in Childhood,vol. 95, no. 6, June 2010.36 Hallman, Kelly, ‘Socioeconomic Disadvantage andUnsafe Sexual Behaviours among Young Womenand Men in South Africa’, Paper 190, PolicyResearch Division Working Papers, PopulationCouncil, New York, 2004.37 Joint United Nations Programme on HIV/AIDS,AIDS Scorecards: Overview–UNAIDSreport on the global AIDS epidemic 2010,UNAIDS, 2010, pp. 17 61, <www.unaids.org/,globalreport/AIDSScorecards.htm>, accessed4September2011.
EM28BAFebr RGua Ory ED201242 Bhatia, Shashi K., and Subhash C. Bhatia,‘Childhood and Adolescent Depression,’AmericanFamily Physician,vol. 75, no. 1, January 2007,pp.73–80.43 Alirol, E., et al., ‘Urbanisation and InfectiousDiseases in a Globalised World’,Lancet,vol. 11,no. 2, February 2011, pp. 132–133.44 World Health Organization and United NationsChildren’s Fund Joint Monitoring ProgrammeforWater Supply and Sanitation,Progress onSanitation and Drinking-Water: 2010 update,WHOand UNICEF Geneva, March 2010, pp.18–19,,<http://whqlibdoc.who.int/publications/2010/9789241563956_eng_full_text.pdf>, accessed5September 2011.45 Water and Sanitation Program,GlobalExperiences on Expanding Water and SanitationServices to the Urban Poor: Accompanyingvolume to the ‘Guidance Notes on Services forthe Urban Poor’,WSP August 2009, p. 161.,46 UN-Water Decade Programme on Advocacy andCommunication, ‘Water and Cities: Facts andfigures’, UNW-DPAC, 2011, p. 2, <www.un.org/waterforlifedecade/swm_cities_zaragoza_2010/pdf/facts_and_figures_long_final_eng.pdf>,accessed 5 September 2011.47Progress on Sanitation and Drinking-Water,p. 22.48 United Nations Educational, Scientific and CulturalOrganization,EFA Global Monitoring Report 2008:Education for All by 2015 – Will we make it?,UNESCO and Oxford University Press, Paris andOxford, UK, 2007 as cited in Bartlett, Sheridan,,‘Urban Children: Discussion of UNICEF program-ming directions’, Discussion paper, Division ofPolicy and Practice, United Nations Children’sFund, New York, February 2010, p. 14.49 United Nations Educational, Scientific and CulturalOrganization,EFA Global Monitoring Report 2010:Reaching the marginalized,UNESCO and OxfordUniversity Press, Paris and Oxford, UK, 2010, p. 6.50 Grantham-McGregor, S., et al., ‘DevelopmentalPotential in the First 5 Years for Children inDeveloping Countries’,Lancet,vol. 369, no. 9555,6 January 2007 pp. 60–70.,51 El-Zanaty, Fatma, and Stephanie Gorin,EgyptHousehold Education Survey (EHES) 2005–06,El-Zanaty and Associates and Macro InternationalInc., Cairo, 2007 p. 126.,
63 United Nations Children’s Fund,Child Traffickingin Europe: A broad vision to put children first,Innocenti Insight, UNICEF Innocenti ResearchCentre, Florence, 2007 p. 12.,64 United Nations Children’s Fund RegionalOffice for Central and Eastern Europe and theCommonwealth of Independent States and Terredes hommes Foundation,Action to Prevent ChildTrafficking in South Eastern Europe: A prelimi-nary assessment,UNICEF and Terre des hommesFoundation, Geneva, 2006, inChild Trafficking inEurope,p. 12.65 International Labour Office,Accelerating Actionagainst Child Labour: Global report under thefollow-up to the ILO Declaration on FundamentalPrinciples and Rights at Work,ILO, Geneva, 2010,pp. xiii, 5.66 Bwibo, N. O., and P Onyango,Final Report of the.Child Labour and Health Research,University ofNairobi, Nairobi, 1987 cited in Bourdillon, Michael,,‘Children as Domestic Employees: Problemsand promises’,Journal of Children and Poverty,vol.15, no. 1, March 2009, p. 3.67 Moscow Humanitarian University and UnitedNations Children’s Fund,Street Children: Overallsituation and challenges,a study commis-sion by the Moscow City Children’s RightsOmbudsman, Moscow, 2009, p. 2; Conticini,Alessandro, and David Hulme,Escaping Violence,Seeking Freedom: Why children in Bangladeshmigrate to the street,Economic and SocialResearch Council Global Poverty Research Group,September2006,p. 8.
References
77
68 Thomas de Benitez, Sarah,State of the World’sStreet Children: Violence,Consortium for StreetChildren, London, 2007 p. 17,.69 Raffaeli, Marcela, et al., ‘Gender Differences inBrazilian Street Youth’s Family Circumstancesand Experiences on the Street’,Child Abuse& Neglect,vol. 24, no. 11, November 2000,pp.1434, 1437 1438.,70 Barker, Gary, et al.,Urban Girls: Empowerment inespecially difficult circumstances,IntermediateTechnology Development Group, London, 2000,cited in Thomas de Benitez,State of the World’sStreet Children,p. 8.
CHAPTER 31 Black, Richard, et al., ‘Migration and Pro-poorPolicy in West Africa’, Working Paper C8,Development Research Centre on Migration,Globalisation and Poverty, University of Sussex,Brighton, UK, November 2004.2 United Nations Department of Economic andSocial Affairs,Trends in International MigrantStock: The 2008 revision – CD-ROM documen-tation,UNDESA, Population Division, New York,2009, p. 2, <www.un.org/esa/population/publications/migration/UN_MigStock_2008.pdf>,accessed 2 October 2011.3 Stephens, Carolyn,Urban Social andEnvironmental Inequalities: Impacts on childrights, health and wellbeing in cities,UNICEFbackground discussion paper forThe State of theWorld’s Children 2012,2011, p. 13.4 Lu, Hong, and Shunfeng Song, ‘Rural Migrant’sPerceptions of Public Safety Protections in UrbanChina’,Chinese Economy,vol. 39, no. 3, 2006,pp. 26–30.5 van de Glind, Hans, ‘Migration and ChildLabour: Exploring child migrant vulnerabili-ties and those of children left behind’, Workingpaper, International Labour Office, InternationalProgrammes on the Elimination of Child Labour,Geneva, 2010, p. 1.
16 Whitehead, Ann, and Iman Hashim, ‘Children andMigration: Background paper for DFID MigrationTeam’, March 2005, <www.childtrafficking.com/Docs/dfid_05_child_mig_bac_0408.pdf>,accessed 12 September 2011, p. 29; Bhabha,Jacqueline, ‘Seeking Asylum Alone: Treatment ofseparated and trafficked children in need of refu-gee protection’, Faculty Research Working PapersSeries, Harvard University, Cambridge, Mass.,March 2004.17 United Nations High Commissioner for Refugees,2009 Global Trends: Refugees, asylum-seek-ers, returnees, internally displaced and statelesspersons,UNHCR, Geneva, June 2010, p. 3.18 United Nations High Commissioner for Refugees,UNHCR Policy on Refugee Protection andSolutions in Urban Areas,UNHCR, Geneva,September 2009, p. 2.19 Lustig, Stuart L., et al., ‘Review of Child andAdolescent Refugee Mental Health’,Journal ofthe American Academy of Child and AdolescentPsychiatry,vol. 43, no. 1, January 2004, p. 24.20Children in China,pp. 110–111;China Population2008.21 Battistella, Graziano, and Cecilia G. Conaco,‘The Impact of Labour Migration on the ChildrenLeft Behind: A study of elementary school chil-dren in the Philippines’,SOJOURN: Journalof Social Issues in Southeast Asia,vol. 13,1998, <www.questia.com/googleScholar.qst?docId=5002305580>, accessed12 September 2011.22 International Labour Organization,Update onEmployment and Labour Market Trends,preparedfor G20 meeting in Seoul, November 2010,cited inNew Internationalist,no. 440,March 2011, p. 16.23 International Labour Organization,GlobalEmployment Trends for Youth: Special issue onthe impact of the global economic crisis on youth,ILO, Geneva, August 2010.24 Ibid., p. 13.
CHAPTER 2 PANELSMaternal and child health services forthe urbanpoorUnited Nations Human Settlements Programme,UN-Habitat and the Kenya Slum UpgradingProgramme,UN-Habitat, Nairobi, 2007 p.7;,UnitedNations Human Settlements Programme,The State of African Cities: Governance, inequalityand urban land markets,UN-Habitat, 2010, p.iii,<www.unhabitat.org/content.asp?cid=9141&catid=7&typeid=46&subMenuId=0>, accessed 25 August2011; Menon, Ruel and Morris, ‘Socio-economicDifferentials in Child Stunting’, pp.282–299; Fotso,‘Child Health Inequities in Developing Countries’,pp. 1–10; African Population and Health ResearchCenter,Strengthening Information Systems,Knowledge Sharing and Partnerships for AddressingUrban Health Vulnerabilities in the Slums ofNairobi, Kenya,APHRC, Nairobi, 2009; Fotso, JeanChristophe, Alex Ezeh and Rose Oronje, ‘Provisionand Use of Maternal Health Services among UrbanPoor in Kenya: What do we know and what can wedo?’,Journal of Urban Health,vol. 85, no. 3, 2008,pp. 428–442, <www.ncbi.nlm.nih.gov/pmc/articles/PMC2329740/pdf/11524_2008_Article_9263.pdf>, accessed 25August 2011; Fotso, JeanChristophe, and Caroline Mukiira, ‘Perceived Accessto and Quality of Care and Utilization of DeliveryCare Services among the Urban Poor: Harnessingthe potentials of private clinics in urban, resource-deprived settings?’,Health Policy and Planning,forthcoming; Izugbara, Chimaraoke, Alex Ezehand Jean Christophe Fotso, ‘The Persistence andChallenges of Homebirths: Perspectives of tradi-tional birth attendants in urban Kenya’,Health Policyand Planning,vol. 24, 2009, pp. 36–45, < http://heapol.oxfordjournals.org/content/24/1/36.full.pdf>,accessed 18 September 2011; Black, Robert E.,et al., ‘Maternal and Child Undernutrition: Globaland regional exposures and health consequences’,Lancet,vol. 371, no. 9608, 2008, pp. 243–260,<http://download.thelancet.com/pdfs/journals/lancet/PIIS0140673607616900.pdf?id=e16241398b8eb460:67ac7f42:1320261e66f:727b1314304374913>,accessed 25 August 2011; World Health OrganizationWorking Group, ‘Use and Interpretation ofAnthropometric Indicators on Nutritional Status’,Bulletin of the World Health Organization,vol. 64,no. 6, 1986, pp. 929–941; The World Bank,Lessonsfrom a Review of Interventions to Reduce ChildMalnutrition in Developing Countries: What can welearn from nutrition impact evaluations?,The WorldBank, Washington, D.C., 2010, <http://siteresources.worldbank.org/EXTWBASSHEANUTPOP/Resources/Nutrition_eval.pdf>, accessed 26 August 2011.
Mapping urban disparities to secure child rightsCenter for International Earth Science InformationNetwork, Columbia University,Where the Poor Are:An atlas of poverty,Columbia University, Palisades,N.Y., 2006, pp. v, 1, 37 <http://sedac.ciesin.columbia.,edu/povmap/downloads/maps/atlas/atlas.pdf>,accessed 20 September 2011; Bedi, Tara, AlineCoulouel and Kenneth Simler,More Than a PrettyPicture: Using poverty maps to design better poli-cies and interventions,The World Bank, Washington,D.C., 2007 pp. 5, 16; Association of Public Health,Observatories, <www.apho.org.uk/default.aspx>,accessed 20 September 2011.
78
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED20126 United Nations Children’s Fund,Children in China:An atlas of social indicators,UNICEF Beijing,,2010, pp. 110–111; National Bureau of Statisticsof China,China Population and EmploymentStatistics Yearbook 2008,China Statistics Press,Beijing, 2009.7 van de Glind, ‘Migration and Child Labour’, p. 5.8 McKenzie, David J., ‘A Profile of the World’sYoung Developing Country Migrants’, Backgroundpaper to the 2007World Development Report,WPS4021, The World Bank, October 2006, pp. 3, 7.9 Whitehead, Ann, et al., ‘Child Migration, ChildAgency and Inter-generational Relations in Africaand South Asia’, Working Paper T24, Developmentand Research Centre on Migration, Globalisationand Poverty, Brighton, UK, December 2007 p. 10.,10 Development Research Centre on Migration,Globalisation and Poverty, ‘Independent ChildMigration: Introducing children’s perspectives’,Briefing No. 11, Sussex Centre on MigrationResearch, Brighton, UK, August 2008, p. 2.11 International Labour Organization andUnderstanding Children’s Work,Joining Forcesagainst Child Labour: Interagency report for theHague Global Child Labour Conference of 2010,ILO and UCW, Geneva, May 2010, p. 58.27 Ibid., pp. 1–2.12 Whitehead et al., ‘Child Migration, Child Agency’,p. 17.13 Ibid.14 For a review see Whitehead et al., ‘ChildMigration, Child Agency’, p. 28; Kwankye,Stephen O., et al., ‘Coping Strategies ofIndependent Child Migrants from NorthernGhana to Southern Cities’, Working Paper T-23,Development Research Centre on Migration,Globalisation and Poverty, Brighton, UK,November 2007 pp. 11–12, <www.migration-,drc.org/publications/working_papers/WP-T23.pdf>, accessed 2 October 2011; Khair, Sumaiya,Preliminary Report on Child Migrant Workersin the Informal Sector in Dhaka,Refugee andMigratory Movements Research Unit andDevelopment Research Centre on Migration,Globalisation and Poverty, Dhaka, Bangladesh,and Sussex, UK, 2005.15 Akar, Hanife, ‘Challenges for Schools inCommunities with Internal Migration Flows:Evidence from Turkey’,International Journalof Educational Development,vol. 30, no. 3,May 2010, pp. 263, 269.
25 Peeters, Pia, et al., ‘Youth Employment inSierra Leone: Sustainable livelihood opportuni-ties in a post-conflict setting’, The World Bank,Washington, D.C., April 2009, pp. 123–124, TableA1.1, <http://issuu.com/world.bank.publications/docs/9780821378229>, accessed12 September 2011.26Global Employment Trends for Youth: Specialissue,p. 26.
28 United Nations Office for West Africa,YouthUnemployment and Regional Insecurity inWest Africa,UNOWA Issues Papers, Dakar,December 2005, p. 10; Odigie, S.A., and A.I.Orobosa, ‘Population, Poverty and SustainableDevelopment: An empirical investigation of theNigeria scenario’, in Aghayere, V. O., et al.,NigeriaPolitical Economy and Sustainable Developments,All Nations Printing Press, Benin City, 2008;Wosu, Eze, and A. Kinikanwo Anele, ‘Rural-Urban Migration of Young Persons from SelectedConflict Ridden Communities in Rivers State: Asociological approach’,African Journal of PoliticalScience and International Relations,vol. 4, no. 6,2010, p. 210, <www.academicjournals.org/ajpsir/pdf/pdf2010/June/Wosu%20and%20Anele.pdf>,accessed 2 October 2011.29 Sommers, Marc,West Africa’s Youth EmploymentChallenge: The case of Guinea, Liberia, Sierra Leoneand Côte d’Ivoire,United Nations IndustrialDevelopment Organization, Vienna, October 2007,pp. 6, 15–18; Blum, Robert, ‘Youth in Sub-SaharanAfrica’,Journal of Adolescent Health,vol. 41,no. 3, 2007 p. 231;Youth Unemployment and,Regional Insecurity in West Africa,p. 10.30 International Labour Organization,GlobalEmployment Trends for Youth,ILO, Geneva,2006, p. 20.
31 de Pee, Saskia, et al., ‘How to Ensure NutritionSecurity in the Global Economic Crisis to Protectand Enhance Development of Young Children andOur Common Future’,Journal of Nutrition,vol. 140, no. 1, January 2010, pp. 138S–142S.32 Krug, E., et al.,World Report on Violence andHealth,World Health Organization, Geneva, 2002;Baker-Henningham, H., et al., ‘Experiences ofViolence and Deficits in Academic Achievementamong Urban Primary School Children inJamaica’,Child Abuse and Neglect,vol. 33,no. 5, May 2009, pp. 296–306; Mudege,Netsayi N., Eliya M. Zulu and ChimaraokeIzugbara, ‘How Insecurity Impacts on SchoolAttendance and School Dropout among UrbanSlum Children in Nairobi’,International Journalof Conflict and Violence,vol. 2, no. 1, 2008,pp. 98–112.33 Pickett, Kate E., and Richard G. Wilkinson,‘Child Wellbeing and Income Inequality in RichSocieties: Ecological cross sectional study’,BMJ,vol. 335, no. 7629, 16 November 2007,pp. 169–172.34 Pinheiro, Paulo Sérgio,World Report on Violenceagainst Children,No. 8, United Nations, New York,2006, pp. 304–305.35 Moser, Caroline, Ailsa Winton and AnnaliseMoser, ‘Violence, Fear, and Insecurity among theUrban Poor in Latin America’, in Fay,Urban Poor inLatin America,pp. 132–133.36 Ibid., p. 148.37 The World Bank,Violence in the City:Understanding and supporting communityresponses to urban violence,The World Bank,Washington, D.C., 2010, p. 38.38 Pinheiro,World Report on Violenceagainst Children.
46 Margesson, Rhonda, and Maureen Taft-Morales,Haiti Earthquake: Crisis and response,CRS Reportfor Congress, Congressional Research Service, 8March 2010, pp. 3, 10, 24, <www.dtic.mil/cgi-bin/GetTRDoc?AD=ADA516429&Location=U2&doc=GetTRDoc.pdf>, accessed 2 October 2011.47 Bilham, Roger, ‘Lessons from the HaitiEarthquake’,Nature,vol. 463, 18 February 2010,pp. 878–879, <www.nature.com/nature/journal/v463/n7283/pdf/463878a.pdf>,accessed 2 October 2011.48 Costello et al., ‘Managing the Health Effectsof Climate Change’, p. 1712.49 Fisher, Sarah, ‘Violence against Women andNatural Disasters: Findings from post-tsunamiSri Lanka’,Violence against Women,vol. 16,no. 8, August 2010, pp. 902–918, abstract availa-ble at <http://vaw.sagepub.com/content/16/8/902.abstract>, accessed 12 September 2011.50 Plan UK,Child-Centred Disaster Risk Reduction:Building resilience through participation –Lessons from Plan International,Plan UK,London, 2010, pp. 4, 29–30.51 Pelling, Mark, ‘Urban Governance and DisasterRisk Reduction in the Caribbean: The experiencesof Oxfam GB’,Environment and Urbanization,vol. 23, no. 2, in press.52 Archer, Diane, and Somsook Boonyabancha, ‘Seeinga Disaster as an Opportunity: Harnessing the energyof disaster survivors for change’,Environment andUrbanization,vol. 23, no. 2, 21June 2011, abstractavailable at <http://eau.sagepub.com/content/early/2011/06/21/0956247811410011.abstract>,accessed 12September 2011.
Fund, New York, 2011, pp. 17–18; Inter-AmericanDevelopment Bank,Assessment of ParticipatoryBudgeting in Brazil,Inter-American DevelopmentBank and Center for Urban DevelopmentStudies, Harvard University, Washington, D.C.,and Cambridge, Mass., 2005; Cabannes, Yves,‘Children and Young People Build ParticipatoryDemocracy in Latin American Cities’,Environmentand Urbanization,vol. 18, no. 1, 2006, pp. 195–218.3 In Spain, for example, nine indicators of thequality of child-friendly cities were tested in40cities that participated in the programme.These nine indicators are: noise restriction,pollution, electromagnetic radiation, safe playareas, safe routes between main communityareas, the school as a dynamic centre, publicfacilities for all age groups (adapted for chil-dren), child-friendly public services, adequateprivacy at home and in the community, andjuxtaposition of built-up areas and the country-side. Information supplied by the UNICEF SpainNational Committee.4 Hart, Roger,Children’s Participation: The theoryand practice of involving young citizens incommunity development and environmental care,UNICEF London and New York, 1997; Driskell,,David,Creating Better Cities with Children andYouth: A manual for participation,Earthscan,London, 2002.5 Hart, ‘Planning Cities’, p. 6.6 Anh, M. T. Phuong, et al., ‘Urban and Peri-urbanAgriculture in Hanoi: Opportunities andconstraints for safe and sustainable food produc-tion’, Technical Bulletin No. 32, AVRDC – TheWorld Vegetable Center, Shanhua, Taiwan, 2004,pp. 31–32.7 The World Bank,Agriculture Investment,TheWorld Bank, Washington, D.C., 2006, p. 32.8 Scott, Vera, et al., ‘Research to Action to AddressInequities: The experience of the Cape TownEquity Gauge’,International Journal for Equity inHealth,vol. 7 no. 6, 4 February 2008.,9 United Nations Population Fund,State of WorldPopulation 2007: Youth Supplement – Growingup urban,UNFPA, New York, 2007 <www.unfpa.,org/swp/2007/youth/english/story/preface.html>,accessed 19 September 2011.10 Borzekowski, Dina L.G., ‘The Project IgniteEvaluation:Tribesin Trinidad and Tobago andShugain Kenya and Zambia’, Johns HopkinsUniversity, 2010.11 Cairncross, Sandy, and Vivian Valdmanis, ‘WaterSupply, Sanitation, and Hygiene Promotion’,Chapter 41 inDisease Control Priorities inDeveloping Countries,2nd ed., edited by DeanT. Jamison et al., The World Bank and OxfordUniversity Press, Washington, D.C., and NewYork, April 2006, <www.ncbi.nlm.nih.gov/books/NBK11728>, accessed 19 September 2011;Gunther, I., and G. Fink, ‘Water and Sanitationto Reduce Child Mortality: The impact and costof water and sanitation infrastructure’, PolicyResearch Working Paper 5618, The World BankDevelopment Economics Prospects Group,Washington, D.C., March 2011.13 Plan International,Because I Am a Girl: Thestate of the world’s girls 2010 – Digital andurban frontiers: Girls in a changing land-scape,Plan International, Brussels, 2010,<http://plan-international.org/girls/static/docs/BIAAG_2010_EN2.pdf>, accessed19 September 2011, pp. 3–5.14 United Nations High Commissioner for Refugees,Refugee Education in Urban Settings: Casestudies from Nairobi, Kampala, Amman andDamascus,Operational Solutions and TransitionSection, Division for Programme Support andManagement, UNHCR, Geneva, December 2009,pp. 25–30.
39 According to the Centre for Research on theEpidemiology of Disasters (CRED), at least oneof the following criteria must be fulfilled for asituation to be officially recorded as a disas-ter: 10 ormore people reported killed, 100 ormore people reported affected, the declarationof a state of emergency, a call for interna-tional assistance. See Centre for Research onthe Epidemiology of Disasters, EM-DAT: TheInternational Disaster Database, <www.emdat.be>,accessed 11 August 2011.40 Centre for Research on the Epidemiology ofDisasters, EM-DAT: The International DisasterDatabase, <www.emdat.be>, accessed11August 2011.
41 Intergovernmental Panel on Climate Change,Climate Change 2007: Synthesis report,IPCC,Geneva, 2007 pp. 44–54, <www.ipcc.ch/pdf/,assessment-report/ar4/syr/ar4_syr.pdf>,accessed 2 October 2011.
42 Bicknell, Jane, David Dodman andDavid Satterthwaite, eds.,Adapting Cities toClimate Change: Understanding and addressingthe development challenges,Earthscan, London,2009, p. 11.43 DARA,Climate Vulnerability Monitor: The stateof the climate crisis,DARA Climate VulnerableForum, Madrid, 2010, p. 12, <http://daraint.org/wp-content/uploads/2010/12/CVM_Complete-1-August-2011.pdf>, accessed 18 September 2011.44 Costello, Anthony, et al., ‘Managing the HealthEffects of Climate Change’,Lancet,vol. 373,16 May 2009, pp. 1693–1733.
45 Gouveia, Nelson, Shakoor Hajat and Ben Armstrong,‘Socioeconomic Differentials in the Temperature-Mortality Relationship in São Paulo, Brazil’,International Journal of Epidemiology,vol. 32,no. 3, 2003, p. 392.
EM28BAFebr RGua Ory ED2012CHAPTER 3 PANELWomen, children, disaster and resilienceUnited Nations Economic and Social Commission forAsia and the Pacific and United Nations InternationalStrategy for Disaster Reduction,ProtectingDevelopment Gains: Reducing disaster vulnerabil-ity and building resilience in Asia and the Pacific,ESCAP and UNISDR, Bangkok, April 2010, p. 4,<http://reliefweb.int/sites/reliefweb.int/files/resources/4B7EEA9DF1CBE43E852577C800730881-ESCAP-ISDR-Asia-Pacific-Disaster-Report-2010.pdf>, accessed 6 October 2011; Government of theRepublic of the Philippines and others,Philippines:Typhoons Ondoy and Pepeng – Post-disaster needsassessment,26 November 2009, <http://sitere-sources.worldbank.orgINTPHILIPPINES/Resources/PDNAVol1MainReport.pdf>, accessed 30 September2011; Australian Aid Program in the Philippines,‘Building the Resilience and Awareness of MetroManila Communities to Natural Disasters and ClimateChange Impacts’, Program Design Document, Buildingthe Resilience and Awareness of Communities(BRACE) Program, April 2011; Otara, Rio Grace M.,and United Nations Children’s Fund in partnership withCouncil for the Welfare of Children, ‘Project Report onthe Registration and Family Tracing of Separated andUnaccompanied Children: Tropical Storm Ondoy andTyphoon Pepeng’, Quezon City, Philippines, October2010, pp. 22–23; Oxfam,Banyuhay: Mga kuwento nghamon at pagbangon ng kababaihan sa panahon ngOndoy,[New Life: Stories of Challenges and Recoveryby Women during Ondoy], Oxfam, Quezon City,Philippines, 2011.
.12 Hart, ‘Planning Cities’, p. 17
CHAPTER 41 Racelis, Mary, and Angela Desiree M. Aguirre,Making Philippine Cities Child Friendly: Voices ofchildren in poor communities,Innocenti Insight,Institute of Philippine Culture, Ateneo de ManilaUniversity, and United Nations Children’s FundInnocenti Research Centre, Florence, 2005.2 Hart, Roger, ‘Planning Cities with Children inMind: A background paper forThe State of theWorld’s Children 2012’,United Nations Children’s
References
79
15 Hart, ‘Planning Cities’, p. 25.16 World Health Organization,Global Status Reporton Road Safety: Time for action,WHO, Geneva,2009, p. 17.17 Ibid.; additional reference provided by the UNICEFLatin America and the Caribbean RegionalOffice: data published June 2011 by TransMilenioS.A., <www.transmilenio.gov.co/WebSite/Default.aspx>, accessed 18 September 2011.18 Quito, Ecuador; Cairo, Egypt; New Delhi,India; Port Moresby, Papua New Guinea;and Kigali, Rwanda.19Because I Am a Girl.20 World Health Organization, Prevention andControl of Noncommunicable Diseases:Implementation of the global strategy, Reportby the Secretariat EB 126/12, WHO, Geneva,26November 2009, p. 10.21 Reinehr, Thomas, et al., ‘Obesity in DisabledChildren and Adolescents: An overlooked groupof patients’,Deutsches Arzteblatt International,vol.107 no. 15, 2010, p. 268.,22 Hart, ‘Planning Cities’, p. 10.23 Ibid., p. 8.24 Ibid., p. 12.25 Evans, Gary W., ‘The Built Environment andMental Health’,Journal of Urban Health: Bulletinof the New York Academy of Medicine,vol. 80,no. 4, December 2003, p.545; Taylor, Andrea F.,Frances E. Kuo and William C. Sullivan, ‘Viewsof Nature and Self-Discipline: Evidence frominner city children’,Journal of EnvironmentalPsychology,vol.21, 2001, pp. 49–63; Kuo,Frances E., and Andrea Faber Taylor, ‘A PotentialNatural Treatment for Attention-Deficit/Hyperactivity Disorder: Evidence from a nationalstudy’,Research and Practice,vol.94, no. 9,September 2004, pp.1580–1586; Taylor, AndreaF Frances E. Kuo and WilliamC. Sullivan, ‘Coping.,with ADD: The surprising connection to greenplay settings’,Environment and Behavior,vol. 33,no. 1, January2001, pp.54–77; Wells, Nancy M.,‘At Home with Nature: Effects of “greenness”on children’s cognitive functioning’,Environmentand Behavior,vol. 32, no. 6, November 2000, pp.775–795; Bell, Anne C., and Janet E. Dyment,‘Grounds for Health: The intersection of greenschool grounds and health-promoting schools’,Environmental Education Research,vol. 14, no. 1,February2008, pp.77–90; Sharp, David, ‘GivingPeople More Green Space’,Journal of UrbanHealth: Bulletin of the New York Academy ofMedicine,vol. 84, no. 1, January2007 pp.3–4.,26 Wells, ‘At Home with Nature’, pp. 781–783.
28 United Nations Development Programme,‘Globalization and Cultural Choice’, Chapter 5inHuman Development Report 2004: Culturalliberty in today’s diverse world,UNDP New York,,2004, p. 99, <http://hdr.undp.org/en/media/hdr04_chapter_5.pdf>, accessed 19 September 2011.29 Qadeer, Mohammad, ‘What Is This Thing CalledMulticultural Planning?’,Bridge,vol. 2, no. 9,2009, pp. 10–11, extract at <http://canada.metropolis.net/pdfs/qadeer_extracted_plan_canada_e.pdf>, accessed 10 August 2011.30 OnePeople, Singapore, <www.onepeople.sg>,accessed 18 September 2011.31 Palfrey, John, and Urs Gasser,Born Digital:Understanding the first generation of digitalnatives,Basic Books, New York, 2008, p. 1.32 Menou, Michel J., ‘Information Behaviour of the“Google Generation” as a Factor in Sustainabilityfor Mexican Cities’,Aslib Proceedings,vol.62,no. 2,2010, p. 166.33 Gasser, Urs, Colin M. Maclay and John G. PalfreyJr.,Working towards a Deeper Understanding ofDigital Safety for Children and Young People inDeveloping Nations,Berkman Center for Internetand Society at Harvard University, Cambridge,Mass., June 2010, pp. 1, 9, 22.34Because I Am a Girl,p. 107; Take Back the Tech!,<www.takebackthetech.net>, accessed 8 June 2011.
2 Hailu, Degol, and Fábio Veras Soares, ‘CashTransfers in Africa and Latin America: Anoverview’, inPoverty in Focus,No. 15, editedby DegolHailu and Veras Soares, InternationalPoverty Centre, Brasilia, August 2008,<www.ipc-undp.org/pub/IPCPovertyInFocus15.pdf>,accessed 28September 2011.3 Georgetown University Hospital, PediatricKIDS Mobile Medical Clinic,<www.georgetownuniversityhospital.org/body_dept.cfm?id=1033>, accessed 28 September 2011.4 Scott, ‘Research to Action’.5 United Nations Children’s Fund,Progress forChildren: Achieving the MDGs with equity,No. 9,UNICEF New York, September 2011, p. 81.,6 Grünewald, Fran§ois, and Andrea Binder, with thesupport of Yvio Georges,Inter-agency Real-TimeEvaluation in Haiti: 3 months after the earthquake– Final report,Global Public Policy Institute andGroupe u.r.d., 31 August 2010.7 United Nations Children’s Fund Evaluation Office,‘Independent Review of UNICEF’s OperationalResponse to the January 2010 Earthquake inHaiti’, UNICEF 14 July 2011.,8 Human Settlements Programme, InternationalInstitute for Environment and Development,‘Building Better Cities with Children and Youth’,Environment and Urbanization Brief 6, IIED,London, October 2002, in Swart Kruger, Jill,with Louise Chawla, ‘We Know SomethingSomeone Doesn’t Know: Children speak out onlocal conditions in Johannesburg’,Environmentand Urbanization,vol. 14, no. 2, October 2002,pp.85–96.9 Hart, ‘Planning Cities’, pp. 15–18.10 Evans, ‘Built Environment and Mental Health’,p. 545; Taylor, Kuo and Sullivan, ‘Views of Natureand Self-Discipline’, pp. 49–63; Kuo and Taylor,‘Potential Natural Treatment’, pp. 1580–1586;Taylor, Kuo and Sullivan, ‘Coping with ADD’,pp. 54–77; Wells, ‘At Home with Nature’, pp.775–795; Bell and Dyment, ‘Grounds for Health’,pp. 77–90; Sharp, ‘Giving People More GreenSpace’, pp. 3–4.
27 Evans, ‘The Built Environment and MentalHealth’, p. 545; Hart, ‘Planning Cities’, p. 13; Krug,Etienne, et al., eds,World Report on Violence andHealth,World Health Organization, Geneva, 2002,p. 25,<www.who.int/violence_injury_prevention/violence/world_report/en/full_en.pdf>, accessed21 September 2011; Samms-Vaughan, MaureenE., Maria D. Jackson and Deanne E. Ashley,‘Urban Jamaican Children’s Exposure toCommunity Violence’,West Indian MedicalJournal,vol. 54, no. 1, January 2005, pp. 14–21,<http://caribbean.scielo.org/scielo.php?script=sci_arttext&pid=S0043-31442005000100004&lng=en&nrm=isosource%5B>, accessed 21 September2011; Seedat, S., et al., ‘Trauma Exposure andPost-traumatic Stress Symptoms in Urban Africanschools’,British Journal of Psychiatry,vol. 184,February 2004, pp. 169–175, <http://bjp.rcpsych.org/content/184/2/169.long>, accessed 21 September2011; Hart, ‘Planning Cities’, p. 13.
80
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012CHAPTER 4 PANELThe Child-Friendly Cities InitiativeUnited Nations Children’s Fund Innocenti ResearchCentre,Poverty and Exclusion among UrbanChildren,Innocenti Digest No. 10, UNICEF InnocentiResearch Centre, Florence, November 2002, <www.childfriendlycities.org/pdf/digest10e.pdf>, accessed14 October 2011; United Nations Population Fund,State of World Population 2007: Youth supplement– Growing up urban,UNFPA, New York, 2007 pp.,iii–iv, <www.unfpa.org/swp/2007/presskit/pdf/youth_swop_eng.pdf>, accessed 14 October 2011; UnitedNations Population Fund,State of World Population2007: Unleashing the potential of urban growth,ch. 2, ‘People in Cities: Hope countering desola-tion’, UNFPA, New York, 2007 <www.unfpa.org/,swp/2007/english/chapter_2/slums.html>, accessed14 October 2011; United Nations Children’s Fund,‘Child Friendly Cities: Examples of CFC initiatives’,<www.childfriendlycities.org/en/to-learn-more/examples-of-cfc-initiatives>, accessed 14 October2011; Buvinich, M., et al., ‘Achieving PolicyChange: The UNICEF Municipal Seal of Approvalin the Brazilian Semi-Arid Region as a strategy toreduce poverty and inequality’, Paper presentedat the Fourth International Conference, RethinkingPoverty: Making polices that work for children,NewYork, 21–23 April 2008, cited in Bernard vanLeer Foundation,Realising the Rights of YoungChildren: Progress and challenges,Early ChildhoodMatters No. 113, Bernard van Leer Foundation, TheHague, November 2009, <www.ecdgroup.com/pdfs/bvf-Realising-the-rights-of-young-children-progress-and-challenges.pdf>, accessed 14 October 2011.
CHAPTER 5 PANELThe paucity of intra-urban dataHaddad, Lawrence, Marie T. Ruel and James L.Garrett, ‘Are Urban Poverty and UndernutritionGrowing? Some newly assembled evidence’,WorldDevelopment,vol. 27 no. 11, November 1999,,p.1899; Harpham, ‘Urban Health in DevelopingCountries’, pp. 107–116;State of the World’sCities 2010/2011;Fotso, ‘Child Health Inequities inDeveloping Countries’, p. 10; Montgomery, ‘UrbanPoverty and Health in Developing Countries’, pp.397–425; Baker, Judy, and Nina Schuler, ‘AnalyzingUrban Poverty: A summary of methods andapproaches’, World Bank Policy Research WorkingPaper 3399, The World Bank, Washington, D.C.,September 2004, p. 17 <http://siteresources.,worldbank.org/INTURBANPOVERTY/Resources/analyzingurbanpoverty.pdf>, accessed28September 2011.
CHAPTER 51 Environmental Health Project,ImprovingtheHealth of the Urban Poor: Learning fromUSAID experience,Strategic Report 12, Officeof Health, Infectious Diseases and Nutrition,Bureau for Global Health, United States Agencyfor International Development, Washington,D.C., August 2004, <www.ehproject.org/PDF/Strategic_papers/SR12-UH%20ImproveHealth.pdf>,accessed 28 September 2011.
Statistical tablesEconomic and social statistics on the countries and territoriesof the world, with particular reference to children’swell-being .
Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .82General note on the data . . . . . . . . . . . . . . . . . . . . . . . . . . . . .82Child mortality estimates . . . . . . . . . . . . . . . . . . . . . . . . . . . .82Revisions to statistical tables . . . . . . . . . . . . . . . . . . . . . . . . .84Explanation of symbols . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .86Under-five mortality rankings . . . . . . . . . . . . . . . . . . . . . . . . .87
Regional Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .124Measuring human development:An introduction to Table 10 . . . . . . . . . . . . . . . . . . . . . . . 125
TABLES
1 Basic indicators . . . . . . . . . . . . . . . . . . . . . . . . . .882 Nutrition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .923 Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .964 HIV/AIDS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1005 Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1046 Demographic indicators . . . . . . . . . . . . . . . . . .1087 Economic indicators . . . . . . . . . . . . . . . . . . . . . 1128 Women . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1169 Child protection . . . . . . . . . . . . . . . . . . . . . . . . .12010 The rate of progress . . . . . . . . . . . . . . . . . . . . .12511 Adolescents . . . . . . . . . . . . . . . . . . . . . . . . . . . .13012 Equity – Residence . . . . . . . . . . . . . . . . . . . . . .13413 Equity – Household wealth . . . . . . . . . . . . . . .138
EM28BAFebr RGua Ory ED2012Statistical tables81
STATISTICAL TABLESOVERVIEWThis reference guide presents the most recent key statistics on child survival,development and protection for theworld’s countries, territories and regions in a single volume. Last year, for the first time,The State of the World’sChildren 2011included tables on Adolescents and Equity, the latter focusing on disparities by household wealth.TheState of the World’s Children 2012adds a second table on Equity, focusing on urban-rural disparities.The statistical tables presented in this volume help meet the demand for timely, reliable, comparable andcomprehensive data on the state of the world’s children. They also support UNICEF’s focus on progress andresults towards internationally agreed goals and compacts relating to children’s rights and development. UNICEFis the lead agency responsible for global monitoring of the child-related goals of the Millennium Declaration aswell as the Millennium Development Goals (MDGs) and indicators; the organization is also a key partner in theUnitedNations’ work on monitoring these targets andindicators.The numbers presented in this reference guide are available online at <www.unicef.org/publications> and<www.unicef.org/sowc2012>, and via the UNICEF global statistical databases at <www.childinfo.org>.Please refer to these websites for the latest tables and for any updates or corrigenda subsequenttoprinting.
The data presented in the following statistical tablesare derived from the UNICEF global databases, whichinclude only internationally comparable and statisti-cally sound data; these data are accompanied bydefinitions, sources and explanations of symbols. Inaddition, data from other United Nations organizationshave been used. The report draws on inter-agencyestimates and nationally representative householdsurveys such as Multiple Indicator Cluster Surveys(MICS) and Demographic and Health Surveys (DHS).Data presented in this year’s statistical tables gener-ally reflect information available as of July 2011.More detailed information on methodology and datasources is available at <www.childinfo.org>.
Some of the data presented here are subject to evolvingmethodologies (e.g., maternal mortality ratio) and revi-sions of time series data (e.g., immunization). For otherindicators, comparable data are unavailable from oneyear to the next. It is therefore not advisable to comparedata from consecutive editions ofThe State of theWorld’s Children.This report includes the latest population estimatesand projections fromWorld Population Prospects:The2010 revision(United Nations Department ofEconomic and Social Affairs, Population Division).Data quality is likely to be adversely affected forcountries that have recently suffered disasters, espe-cially where basic country infrastructure has beenfragmented or where major population movementshaveoccurred.
82
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
General note on the data
Child mortality estimates
Each year, inThe State of the World’s Children,UNICEF reports a series of mortality estimates forchildren – including the annual infant mortality rate,the under-five mortality rate and the number of under-five deaths – for at least two reference years. Thesefigures represent the best estimates available at thetime of printing and are based on the work of the Inter-agency Group for Child Mortality Estimation (IGME),which includes UNICEF the World Health Organization,(WHO), the United Nations Population Division andthe WorldBank.IGME mortality estimates are updated each yearthrough a process of detailed review of all newlyavailable data points that often results in adjustmentsto previously reported estimates. As a result, consecu-tive editions ofThe State of the World’s Childrenshould not be used for analysing mortality trends overtime. Comparable under-five mortality estimates forthe period 1970–2010 at the global and regional levelsare presented below.Country-specific mortality indicators for1970–2010,based on the most recent IGME estimates,arepresented in Table 10 (for the years 1970,1990, 2000and 2010) and are also available at <www.childinfo.org>and <www.childmortality.org>, the IGME website.
Under-five mortality rate (per 1,000 live births)UNICEF RegionAfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld19702292342152561871461941151188824156240139197520420918723515512817492101761913822212219801851941782141231161547783701512520511119851691811662019498137646758121081859719901601741561967786120555450109717088199515516815118965771044844488901558220001421541371755565893835377801387320051271381181594856763127296711236520091141241011464249692522246641125820101111219814341486724232366311057
Under-five deaths (millions)UNICEF RegionAfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorlda
EM28BAFebr RGua Ory ED201219703.73.11.31.61.210.45.35.01.20.60.316.13.316.619753.73.11.31.71.18.65.13.51.10.60.214.33.314.719803.83.31.41.81.07.45.02.40.90.50.212.93.413.219853.93.51.51.90.97.24.72.50.80.40.112.63.512.819904.03.71.62.00.76.64.42.20.60.40.111.83.512.019954.24.01.62.20.65.43.91.60.50.30.110.63.510.720004.24.01.62.20.54.53.31.20.40.20.19.43.39.6
20054.14.01.52.30.43.72.80.90.30.20.18.43.28.5
20093.93.81.42.30.43.32.60.70.20.10.17.73.07.8
20103.83.71.32.20.43.22.50.70.20.10.17.52.97.6
Multiple Indicator Cluster Surveys (MICS):UNICEFsupports countries in collecting statistically soundand internationally comparable data through MICS.Since 1995, nearly 230 surveys have been conductedinapproximately 100 countries and territories. Thefourth round of MICS, involving over 50countries, isunder way, with data collection expected to end in2011. MICS are among the largest sources of data formonitoring progress towards internationally agreeddevelopment goals for children, including the MDGs.Many of the MICS indicators have been incorporatedinto the statistical tables in this report. More informa-tion is available at <www.childinfo.org>.
Regional Classification:In the 2009 edition ofThe Stateof the World’s Children,UNICEF added two new regionalgroupings: Africa and Asia. In addition, the number ofcountries classified in the sub-Saharan Africa regionincreased with the inclusion of Djibouti and the Sudan.As a result, regional estimates for sub-Saharan Africapublished in previous issues ofThe State of the World’sChildrenmay not be comparable with those publishedin this issue. For details of the countries and territoriesincluded in all UNICEF regions, please refer to theRegional Classification, page 124.
Statistical tables
83
STATISTICAL TABLESRevisions to statistical tablesTABLE 1 . BASIC INDICATORSPrimary school net enrolment:The primary schoolnet enrolment ratio replaces the primary schoolnet enrolment/attendance ratio. This indicatoris the official MDG 2 indicator produced by theUnited Nations Educational, Scientific and CulturalOrganization (UNESCO) Institute for Statistics (UIS)based on administrative data collected by nationalschoolsystems.TABLE 2 . NUTRITIONUnderweight, stunting and wasting:Prevalence ofunderweight, stunting and wasting among childrenunder 5 years of age is estimated by comparing actualmeasurements with an international standard referencepopulation. In April 2006, WHO released the WHO ChildGrowth Standards to replace the widely used NationalCenter for Health Statistics/World Health Organization(NCHS/WHO) reference population, which was basedon a limited sample of children from the United States.The new standards are the result of an intensive studyproject involving more than 8,000 children from Brazil,Ghana, India, Norway, Oman and the United States.Overcoming the technical and biological drawbacksof the old reference population, the new standardsconfirm that children born anywhere in the worldand given the optimum start in life have the potentialto develop to within the same range of height andweight. Differences in children’s growth to age 5 aremore influenced by nutrition, feeding practices, envi-ronment and health care than genetics or ethnicity.estimates/en/index.html>. Owing to differences insource data and estimation methodology, theseprevalence estimates are not comparable to the aver-ages published in previous editions ofThe State ofthe World’s Childrenand may not be comparable toestimates for other regions in the currentpublication.Vitamin A supplementation:Emphasizing theimportance for children of receiving two annual dosesof vitamin A (spaced 4–6 months apart), this reportpresents only full coverage of vitamin A supplementa-tion. In the absence of a direct method to measure thisindicator, full coverage is reported as the lower cover-age estimate from rounds 1 and 2 in a given year.TABLE 3 . HEALTHWater and sanitation:The drinking water andsanitation coverage estimates in this report comefrom the WHO/UNICEF Joint Monitoring Programmefor Water Supply and Sanitation (JMP). These arethe official United Nations estimates for measuringprogress towards the MDG target for drinking waterand sanitation, based on a standard classification ofwhat constitutes coverage. The JMP estimates cover-age using a linear regression line fitted to data fromall available household sample surveys and censuses.Full details of the JMP methodology can be found at<www.childinfo.org> and <www.wssinfo.org>.Immunization:This report presents WHO andUNICEF estimates of national immunization cover-age. These are the official United Nations estimatesfor measuring progress towards the MDG indicatorfor measles-containing vaccine coverage. A moredetailed explanation of the process can be found at<www.childinfo.org/immunization_countryreports.html>.Regional averages for the six reported antigens arecomputed as follows:• For BCG, regional averages include only thosecountries where BCG is included in the nationalroutine immunization schedule.• For DPT, polio, measles, HepB and Hib vaccines,regional averages include all countries.• For protection at birth (PAB) from tetanus, regionalaverages include only the countries where maternaland neonatal tetanus is endemic.
In this report, all of the child anthropometry indica-tors are reported according to the WHO Child GrowthStandards. Owing to the differences between theold reference population and the new standards, aswell as to updates to the data time series, prevalenceestimates of child anthropometry indicators publishedin consecutive editions ofThe State of the World’sChildrenmay not be fully comparable.
UNICEF and WHO have initiated a process to harmonizeanthropometric data used for computation and estima-tion of regional and global averages and trend analysis.As part of this process, underweight and stuntingprevalences for the developing regions and the worldare derived from a model described in M.deOnis etal., ‘Methodology for Estimating Regional and GlobalTrends of Child Malnutrition’ (InternationalJournal ofEpidemiology,vol. 33, 12 November 2004, pp. 1260–1270)and are available online at <www.who.int/nutgrowthdb/
84
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
TABLE 4 . HIV/AIDSIn 2011, the Joint United Nations Programme onHIV/AIDS (UNAIDS) released new global and regionalHIV and AIDS estimates for 2010 that reflect keychanges in WHO HIV treatment guidelines for adults
and children and for prevention of mother-to-childtransmission of HIV as well as improvements inassumptions of the probability of HIV transmissionfrom mother to child and net survival rates for infectedchildren.In addition, there are also more reliable dataavailable from population-based surveys, expandednational sentinel surveillance systems and programmeservice statistics in a number of countries. Based onthe refined methodology, UNAIDS has retrospectivelygenerated new estimates of HIV prevalence, thenumber of people living with HIV and those needingtreatment, AIDS-related deaths, new HIV infections andthe number of children whose parents have died dueto all causes including AIDS for past years. Only newestimates should be used for trend analysis.The new HIV and AIDS estimates are includedin thistable for global and regional averages only and willalso be published in the forthcoming reportGlobalResponse to HIV/AIDS: Epidemic update and towardsuniversal access, 2011.The country-specific HIV/AIDSestimates in Table 4 refer to the year 2009.Afull set ofestimates will be available in early 2012.Overall, the global and regional figures publishedinThe State of the World’s Children 2012are notcomparable to estimates previously published. Moreinformation on HIV and AIDS estimates, methodologyand updates can be found at <www.unaids.org> or<www.childinfo.org>.
important at the primary level than at the secondarylevel. The secondary gross enrolment ratio is presentedin Tables 8 and 11 in slightly different formats than inprevious editions of this report.TABLE 6 . DEMOGRAPHIC INDICATORSPopulation annual growth rate and average annualgrowth rate of urban population:For the first time,the table includes a projection for 2010–2030. Theyear ranges now cover 1970–1990, 1990–2010 and2010–2030.TABLE 7 . ECONOMIC INDICATORSGNI per capita:The table now includes data on GNIper capita in purchasing power parity (PPP) US$alongside the previously published data, whichexpress GNI in US$ (exchange rate terms). Whileboth these indicators are widely used, GNI per capita(PPP US$) takes into account differences in pricelevels between countries to allow for a more accuratecomparison of living standards. These data are basedon the International Comparison Program (ICP), whichproduces internationally comparable price and volumemeasures for gross domestic product (GDP) and itscomponent expenditures. For more information,please see <http://go.worldbank.org/K520C6USR0>.Proportion of the population living below US$1.25per day:In 2008, the World Bank announced a newpoverty line that is based on revised estimates of PPPprice levels around the world. Table 7 reflects thisupdated poverty line and reports on the proportionof the population living below US$1.25 per day at2005prices, adjusted for PPP The new poverty thresh-.old reflects revisions to PPP exchange rates basedon the results of the 2005 ICP a worldwide statistical,operation involving some 180 countries. The revisionsreveal that the cost of living across the developingworld is higher than previously estimated. Owing tothe revisions, poverty rates for individual countriescannot be compared with those reported in previouseditions. More detailed information can be found at<www.worldbank.org>.TABLE 8 . WOMENEnrolment ratio: females as a % of males, using primaryand secondary gross enrolment ratio:Replacing ‘enrol-ment ratio: females as a % of males, using primary andsecondary net enrolment and attendance ratios’, thenew indicators are official MDG 3 indicators that moni-tor gender equality and the empowerment of women.The gross enrolment ratio is the preferred indicator incomparing the educational participation of girls and
TABLE 5 . EDUCATIONPre-primary gross enrolment ratio:For the first time,the table includes pre-primary education. Participationin pre-primary education promotes on-time commence-ment of primary school as well as efficient progressionthrough school.Survival rate to the last grade of primary school:Thesurvival rate to Grade 5 (percentage of primary schoolentrants reaching Grade 5) was replaced in 2008 bythe survival rate to the last grade of primary school(percentage of children entering the first grade ofprimary school who are expected to reach the lastgrade). The survival rate to the last grade became anofficial indicator for MDG 2 (universal primary educa-tion) in January 2008.
Secondary gross enrolment ratio:This indicator wasremoved because it is primarily used in comparison tothe net enrolment ratio to determine if there is a largepopulation of children enrolled at an inappropriateage. However, age-appropriate participation is more
EM28BAFebr RGua Ory ED2012
Statistical tables
85
STATISTICAL TABLESboys, as it takes into account all children participatingat a given level, regardless of age.Survival rate to the last grade of primary: females asa % of males:This highlights progression throughschool and is an official indicator for MDG 2. Forthe first time inThe State of the World’s Children,this indicator is being presented as ‘females as a% of males’, which adds a dimension of genderdisaggregation not included in previous editions.Maternal mortality ratio (adjusted):The table presentsthe ‘adjusted’ maternal mortality ratios for theyear 2008, as produced by the Maternal MortalityEstimation Inter-agency Group (MMEIG), composedof WHO, UNICEF the United Nations Population Fund,(UNFPA) and the World Bank, together with indepen-dent technical experts. To derive these estimates, theinter-agency group used a dual approach: makingadjustments to correct misclassification and under-reporting in existing estimates of maternal mortalityfrom civil registration systems, and using a modelto generate estimates for countries without reliablenational-level estimates of maternal mortality.These ‘adjusted’ estimates should not be comparedto previous inter-agency estimates, as the method-ological approach is not the same. A full report withcomplete country and regional estimates for the years1990, 1995, 2000, 2005 and 2008, as well as details onthe methodology, can be found at <www.childinfo.org/maternal_mortality.html>.TABLE 9 . CHILD PROTECTIONViolent discipline:Previous estimates used in UNICEFpublications and in MICS country reports prior to 2010were calculated using household weights that did nottake into account the last-stage selection of childrenfor the administration of the child discipline module inMICS surveys. (A random selection of one child aged2–14 is undertaken for the administration of the childdiscipline module.) In January 2010, it was decidedthat more accurate estimates are produced by usinga household weight that takes the last-stage selectioninto account. MICS 3 data were recalculated using thisapproach. All UNICEF publications produced after 2010,includingThe State of the World’s Children 2012,usethe revised estimates.TABLE 11 . ADOLESCENTSLower and upper secondary gross enrolment ratios:Introduced for the first time, these indicators aid theunderstanding of adolescent participation in second-ary school. Disaggregating the secondary level makesthe issue of dropout more evident.
Explanation of symbols
Because the aim of these statistical tables is to provide a broad picture of the situation of children and womenworldwide, detailed data qualifications and footnotes are seen as more appropriate for inclusion elsewhere.Sources and years for specific data points are available at <www.childinfo.org>.Symbols specific to a particular table are included in the table footnotes. The following symbols arecommon across all tables:–xy***#Data are not available.Data refer to years or periods other than those specified in the column heading. Such data are notincluded inthe calculation of regional and global averages.Data differ from the standard definition or refer to only part of a country. Such data are included in thecalculation of regional and global averages.Data refer to the most recent year available during the period specified in the column heading.Excludes China.For a complete list of countries and territories in the regions, subregions and country categories,seepage 124.
86
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
Under-five mortality rankingsThe following list ranks countries and territories in descending order of their estimated 2010 under-five mortalityrate (U5MR), a critical indicator of the well-being of children. Countries and territories are listed alphabetically inthe tables on the following pages.Under-5mortalityrate (2010)Countries and territoriesValue Rank
Under-5mortalityrate (2010)Countries and territoriesValue Rank
Under-5mortalityrate (2010)Countries and territoriesValue Rank
SomaliaMaliBurkina FasoSierra LeoneChadDemocratic Republic of the CongoHaitiAngolaCentral African RepublicGuinea-BissauAfghanistanNigerNigeriaBurundiCameroonMozambiqueGuineaCôte d’IvoireEquatorial GuineaBeninMauritaniaZambiaEthiopiaLiberiaSudan1TogoUgandaGambiaCongoMalawiDjiboutiRwandaPakistanComorosKenyaLesothoSao Tome and PrincipeZimbabweSwazilandYemenUnited Republic of TanzaniaSenegalGabonGhanaMyanmarIndiaTajikistanMadagascarEritreaPapua New GuineaSouth AfricaBhutanTurkmenistanTimor-LesteBolivia (Plurinational State of)Lao People’s Democratic RepublicUzbekistanCambodiaNepalKiribatiBangladeshBotswanaAzerbaijanMicronesia (Federated States of)NamibiaNauru1
18017817617417317016516115915014914314314213613513012312111511111110610310310399989392919187868585808078777675747466636362616157565655545452515049484846424040
123456789101112121415161718192021212324242427282930313133343535373739404142434345464648494951525254555557585960616163646565
IraqKyrgyzstanAlgeriaCape VerdeMoroccoIndonesiaDemocratic People’s Republic of KoreaKazakhstanTuvaluGuatemalaMongoliaSurinameGuyanaPhilippinesDominican RepublicNicaraguaSolomon IslandsTrinidad and TobagoIran (Islamic Republic of)Marshall IslandsParaguayHondurasJamaicaViet NamEgyptGeorgiaJordanLebanonNiueOccupied Palestinian TerritorySaint Vincent and the GrenadinesArmeniaBarbadosEcuadorPanamaSamoaBrazilColombiaPalauPeruRepublic of MoldovaAlbaniaChinaSaudi ArabiaTurkeyVenezuela (Bolivarian Republic of)BelizeFijiLibyaMexicoSri LankaBahamasEl SalvadorSaint LuciaSyrian Arab RepublicTongaTunisiaMaldivesMauritiusArgentinaRomaniaSeychellesVanuatuBulgariaThailandUkraine
393836363635333333323231302927272727262625242423222222222222212020202020191919191918181818181717171717161616161616151514141414131313
676869696972737373767678798081818181858587888890919191919191979898989898103103103103103108108108108108113113113113113118118118118118118124124126126126126130130130
DominicaRussian FederationThe former Yugoslav Republic of MacedoniaGrenadaKuwaitUruguayBahrainCosta RicaLatviaChileCook IslandsOmanAntigua and BarbudaBosnia and HerzegovinaMontenegroQatarSaint Kitts and NevisSlovakiaUnited StatesBrunei DarussalamLithuaniaSerbiaUnited Arab EmiratesBelarusCanadaCroatiaCubaHungaryMalaysiaMaltaNew ZealandPolandAustraliaEstoniaIsraelRepublic of KoreaSpainSwitzerlandUnited KingdomAndorraAustriaBelgiumCyprusCzech RepublicDenmarkFranceGermanyGreeceIrelandItalyMonacoNetherlandsPortugalFinlandJapanLuxembourgNorwaySingaporeSloveniaSwedenIcelandLiechtensteinSan MarinoHoly See
121212111111101010999888888877776666666665555555444444444444443333333222–
133133133136136136139139139142142142145145145145145145145152152152152156156156156156156156156156165165165165165165165172172172172172172172172172172172172172172186186186186186186186193193193–
Because of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to theUnitedNations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States are not yet available for most indicators.Aggregated data presented are for the Sudan pre-cession.
EM28BAFebr RGua Ory ED2012
Statistical tables
87
TABLE 1: BASIC INDICATORSUnder-5mortalityrankUnder-5mortality rate19902010Infant mortalityrate (under 1)19902010Annual no.NeonatalTotalAnnual no. of under-5deathsmortality population of birthsrate(thousands) (thousands) (thousands)2010201020102010gNI percapita(US$)2010LifePrimaryexpectancy Total adult school net% share ofat birthliteracy enrolmenthousehold income(years)ratio (%)rate (%)2000–2010*20102005–2010* 2007–2009* lowest 40% highest 20%
Countries and territories
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia(Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republicof the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFiji
55145611031521303145815156699514210810334291421391815615617217273617231133819891118194916523113
121195959122220518312113785916520719483712511620171511313111445181912317625294621901412118430
EM28BAFebr RGua Ory ED201254848197131761425113663615917391819869391012366443317049112272022161216151061784174650918103110878574611011316383088741715105111110122311779514484168481188717111254283617611938843845291069981617636189865533261123731122181914814246815235191247384222344144241511123229564133229,9303,7602,007194,9463997,49416,4698,38314,13819,59934,0174964,40111,22717,1141,341,33546,2957354,043204,65919,7384,40311,2581,10410,49324,34665,9665,550889689,92714,46581,1216,1937005,2541,34182,95086126332473,0238767132833187103831015450324516,4869142814207367343112131153482,873642612162991,88112626191162,6131914025501120381693202380231518213018001001246502066412311027101,7904,7906,8909,39031,180 x6,2405501607601,16041,950 x3,1604606009,9404,2605,5108202,310–6,5801,07013,7605,550 x30,460 x17,870a18058,9801,280 x4,9604,8604,5102,3403,36014,68034014,3603803,61066765373787355506351817448497973736157–795576797978184623481510963518335869487958–737573725161755969
11108691728145126981651726311813961981561721132052
209416892432627559993221714318171044178139
1491836416181420544616104820641711556
140365571442324468874181599161493510796
1031631398712184439149381744147344
45918141471132197427103283226
31,4123,20435,4688519,0828940,4123,09222,2688,3949,1883431,262148,6922739,59510,7123128,850726
1,385417141795269447303741825233,0383106122835015
1911260121010109001400110391
330 x4,0004,46041,130 x3,96010,6108,4503,09043,740 x46,7105,180d25,420 x640d6,03045,4203,7407501,920
487773–51–7674828171757569777080765667
–9673–709998100––100–9156–100––425391988490959829677871–85553499949374––96559910098–10067–––88846684936710030–
–859584–90–9397–86929989–9599100948895878795979864998992–8367–9596 z9387–98–579510099–––954598829795965737978492
222018 x–8–132218 x2220––22–232111 x18149189x11–14182116152013151724168813–121620––25 x–1523 x17–13132213––1823–
394342 x–62–514041 x3842––41–364159 x4653614365 x58–5147435251405649473148626853–554842––36 x–5136 x47–54544252––4339–
88
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
Under-5mortalityrank
Under-5mortality rate19902010
Infant mortalityrate (under 1)19902010
Annual no.NeonatalTotalAnnual no. of under-5deathsmortality population of birthsrate(thousands) (thousands) (thousands)2010201020102010
gNI percapita(US$)2010
LifePrimaryexpectancy Total adult school net% share ofat birthliteracy enrolmenthousehold income(years)ratio (%)rate (%)2000–2010*20102005–2010* 2007–2009* lowest 40% highest 20%
FinlandFranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People'sDemocratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia(Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibiaNauru
5513991352411319315218648301561242156852112411364172761456916456565
1452138892274510178159222181022551151124244956910718862191127340
EM28BAFebr RGua Ory ED201254102285103172736292615178626111151742432836135664040100163172151339147971311574131104080213844776166714679493242819657413252435851499522751314343267309250293221512353410–3122273948412399718212519393217226,2012,2524,2282,1713,9946,355363,32450720,71414,90128,40131615,370417543,4601,299113,423111352,75663131,95123,39147,9632,283101412465601541450356732663576571441117172,217306586238838306008025152000445630120001303700202311456201,01011,6209,0201,08019012,020 x136,540 x11,40079,5104403307,9004,27060018,350 x2,9901,0607,7409,330677372485675–7280665474775179–58737769–687472506562–2,700197,460 x1,8906,6902,850440a4,650–
18617243289117243172136761710797–8815619346728567172165172881869173356013668
799316547912213217822921066151–5819611585654691210386385799871572
347498224744113213015030165–246263352639454243223385491138
6768784077711175613512550104–45175815650378108315324864641359
23545720350392581922570–205248272231343202182955391033
22263115228251538401927–1241321714202229113172819619
5,36562,7871,5051,7284,35282,30224,39211,35910414,3899,9821,5157549,99307,6019,9843201,224,614239,87173,97431,6724,4707,41860,5512,741126,5366,18716,02640,5131002,7375,334
6179341665269577011824673905814266020399527,1654,3721,2671,12572154559511,0771533441,529249130
033613571014488045–5101,696151344301213413122015
47,17042,3907,7604402,70043,3301,24027,2405,5602,7403805403,270650–1,88012,99033,8701,3402,5804,530 x2,32040,99027,34035,0904,75042,1504,3507,4407802,010d880
8081625874806480767154487062–737482656973688081827383736757–7467
––8846100–6797–743952–49–8499–63928578––9986–9210087–9499
9699–7610010076100989674–99––97969897981008897979981100949983–939182949173––909797999194967791807694100––100889091–90–
2420 x161316221519–11171914 x8–821–191917–2016181425 x182113––211918–1018––18211618131717––17–127–18221715–4x–
3740 x485347374842–58464350 x63–6140–454545–4245425136 x454053––434543–5645––44395446524446––46–5664–44394852–78 x–
7310090905989–100–647492982692–578893––97–56559289–
Statistical tables
89
TABLE 3: BASIC INDICATORS1: HEALTHUnder-5mortalityrankUnder-5mortality rate19902010Infant mortalityrate (under 1)19902010Annual no.NeonatalTotalAnnual no. of under-5deathsmortality population of birthsrate(thousands) (thousands) (thousands)2010201020102010gNI percapita(US$)2010LifePrimaryexpectancy Total adult school net% share ofat birthliteracy enrolmenthousehold income(years)ratio (%)rate (%)2000–2010*20102005–2010* 2007–2009* lowest 40% highest 20%
Countries and territories
NepalNetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent andthe GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and TobagoTunisiaTurkeyTurkmenistan
97981933710842152126418614518681151–165113–78391861651184613013354241188111810852
27271294451392917276818104518060–1132–5296783811632391691472537498098
EM28BAFebr RGua Ory ED2012212028018757141743832718057–517–31783516631312551031627161856212311613670251416261593610847–926–44706731912634127872132396678191725315506121142722310841–414–275524145211104666132414144713812510274845142125218–310–142123925882432818910231091833216527,44812,4349,856875,8685,0865,4622,0305389,33150,133–46,07720,860–5251,1869,3807,66420,4116,87969,1222,0611,1246,0281041,34110,48172,7525,04225055954651113226455720174081,059–498378–10351127646519283822441933201791,29810900001234103900007058–26–03008121102190132464,8502,93050,670 x1,20017,200 x1,0505,8209,49034040,92016,22023,8601,030a6,100–31,6502,290–5,920 x2,60049,93070,3502,6407804,2104,5202,2204403,38015,3804,0709,5003,7007272–64745974–47817579675152–8175–704881827667747562577270747465
591721568112129118691142331039849871038015617214516510312613331145118
14181168311213149454712433339050785917152183737271632823
50462714314322322987192061251929648519141291816
9779521321261273636962726654055421511176302922992218
41452373881932087015174721152353741611959714
2833123240102–541992314914424298629510
29,95916,6134,3685,78815,512158,42314,8834,0392,782173,593203,5176,8586,45529,07793,26138,27710,6761,75948,1843,57321,486142,95810,62452174
724183641387556,332060134504,7410702071565942,3444059921478442211,68243813
351041008610031423011241166300313203800
49049,72029,050 x1,0803601,180–85,380b17,890 x1,0506,4606,9901,3002,9404,7102,05012,42021,860d19,8901,8107,8409,9105409,9804,970
688181745451–81737365–76627274687679788169746955–74
59––782961––958756–94609590951009595–989810071–––99–89865098924195–100––89–9891–9587––841009497515799997891100
–9999935463–99788166–97–869792969998999096949694939899929886759694–––9881–90–10095–908396100–9890938395–969995–
1521 x18 x122015–24––21–1112 x1112152017 x–21 x18211612–15 x–––14–1723271614 x24 x21––9–1917–11 x122320192311152116–16 x161616 x
5439 x44 x574349–37––42–5756 x5753504246 x5238 x45394958–49 x–––56–4637294949 x35 x39––63–4248–57 x563741443959504147–46 x474647 x
90
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
Under-5mortalityrank
Under-5mortality rate19902010
Infant mortalityrate (under 1)19902010
Annual no.NeonatalTotalAnnual no. of under-5deathsmortality population of birthsrate(thousands) (thousands) (thousands)2010201020102010
gNI percapita(US$)2010
LifePrimaryexpectancy Total adult school net% share ofat birthliteracy enrolmenthousehold income(years)ratio (%)rate (%)2000–2010*20102005–2010* 2007–2009* lowest 40% highest 20%
TuvaluUgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela(Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
732713015216541145136571261089040213724
571752122915511237739335112818378125
3399137576811521418237711180103
44106181889592063312837901095278
2763116550794412161957695166
14266432646237101232302735
1033,42545,4487,51262,03644,841310,3843,36927,44524028,98087,84824,05313,08912,57143,552
01,514493927571,8624,3015058775981,4679196003741,429
01417141333213101134696029143
–4903,010d38,54053047,14010,5901,2802,76011,5901,1001,060 x1,0704601,270
–546876805778776871747565495061
–7310090–73–989982959362719270
–92899810097929990–94–7392––
–1523–18 x18161519–1518181113 x–
–5137–44 x45464944–4945455556 x–
MEMORANDUMSudan and South Sudanδ
SUMMARY INDICATORS#AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East andNorth AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld160174156196
EM28BAFebr RGua Ory ED201211112198143991059711571766388333530391,020,650855,273398,968411,86435,63132,08714,19116,4423,8043,7091,3222,2411,4831,1921,48690557545553414867242323663110575662864143419671066131375219181954471401824331311113253423417,8793,649,3201,630,1732,019,147584,676404,582989,5085,621,340832,3306,856,7979,95566,07637,45228,62410,8455,82011,425120,61727,996134,7544153,1862,492694249136657,5162,9497,6142,7522,9131,2414,2867,8597,26340,8453,3046698,79671696572747080685970
6362675775806194919899805884
7876876688939195959496898090
1616161619182016121818171817
4949504844464548564543484647
7786120555450109717088
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Under-five mortality rate– Probability of dying between birth and exactly 5 years of age,expressed per 1,000 live births.Infant mortality rate– Probability of dying between birth and exactly 1 year of age,expressed per 1,000 live births.Neonatal mortality rate– Probability of dying during the first 28 completed days of life,expressed per 1,000 live births.gNI per capita– Gross national income (GNI) is the sum of value added by all resident producers, plus anyproduct taxes (less subsidies) not included in the valuation of output, plus net receipts of primary income(compensation of employees and property income) from abroad. GNI per capita is gross national incomedivided by midyear population. GNI per capita in US dollars is converted using the World Bank Atlas method.Life expectancy at birth– Number of years newborn children would live if subject to the mortality risksprevailing for the cross section of population at the time of their birth.Adult literacy rate– Number of literate persons aged 15 and above, expressed as a percentage of the totalpopulation in that age group.Primary school net enrolment ratio– Number of children enrolled in primary or secondary school whoareof official primary school age, expressed as a percentage of the total number of children of official primaryschool age. Because of the inclusion of primary-school-aged children enrolled in secondary school, thisindicator can also be referred to as a primary adjusted net enrolment ratio.Share of household income– Percentage of income received by the 20 per cent of households with thehighest income and by the 40 per cent of households with the lowest income.
MAIN DATA SOURCES
Under-five and infant mortality rates– Inter-agency Group for Child Mortality Estimation(UNICEF, World Health Organization, United Nations Population Division and the World Bank).Neonatal mortality rate– World Health Organization, using civil registrations, surveillance systems andhousehold surveys.Total population and births– United Nations Population Division.Under-five deaths– UNICEF.gNI per capita– The World Bank.Life expectancy– United Nations Population Division.Adult literacy rate and primary school enrolment ratio– UNESCO Institute for Statistics (UIS).Share of household income– The World Bank.
low-income country (GNI per capita is $1,005 or less).lower-middle-income country (GNI per capita is $1,006 to $3,975).upper-middle-income country (GNI per capita is $3,976 to $12,275).high-income country (GNI per capita is $12,276 or more).Data not available.Data refer to years or periods other than those specified in the column heading. Such data are not includedin the calculation of regional and global averages.z Data provided by Chinese Ministry of Education.The UIS data do not currently publish net enrolment ratesfor China.* Data refer to the most recent year available during the period specified in the column heading.
abcd–x
NOTES
Statistical tables
91
TABLE 2: NUTRITION% of children (2006–2010*) who are:% of under-fives (2006–2010*) suffering from:introduced tounderweightwastingstunting% of infants Early initiationbreastfed(WHO)(WHO)(WHO)with lowof breastfeeding exclusively solid, semi-solidor soft foodsbreastfedat age 2birthweight(%)moderatemoderate moderate(2006–2010*)(2006–2010*)(<6 months)(6–8 months) (20–23 months) & severesevere& severe& severeVitamin Asupplementationcoverage rate(6–59 months)2010full coverageΔ(%)% ofhouseholdsconsumingiodized salt(2006–2010*)
Countries and territories
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republicof the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFiji
–7x6––577–7x1011–22124x–14151065138–91611 x911–6x1322 x636x–13 x–7175x5–7x6105x1010118137x–14 x4x20 x10 x
–4350–55––28 x––32––43–21 x–5132596157 x2043––20–6520–73 x3934 x–4157–39 x––25–70––1843–67–74–5633–78 x–69 x57 x
–397–11 x––35––12––43–9x–10–496018 x2040––16697421–60 x233–2843–19 x–154–26––65 x
29 x54 y39 y–77 x––48 y––44 y––74 y–38 x––76 y6779 y29 x46 y70 y–––70 y82 y64 y–80 x55 y36–43 y70 y–78 x––54 y–47 y––31 x52–23 y–62 y77 x66 y72 y–43 x–54 x–
54 x3122–37 x–2823––16––91–4x–2792664010 x625–––794321–13 x4759––33–21 x–4937–16––37 x
33 x53–16 y–2y5––8––41–1x–4181341x112––26292816––2430–4y3–11 x–116––––19
12 x21–7y–0y1––2––12–1x–15310x4–––7875––813––1–3x––5––––4
9x94–8y–1y4––7––17–2x–28614x72––116117––1216–3y1–8x–18––––5
59 x1915–29 y–8y19––25––43–4x–2243342710 x317––35584036––4339–10 y13–30 x–640––––3243–31 y–18–2919 y–44 x–51 x–
96–––28–––––89 w––100––––100–24–91–––10073–89––068–––1884––100––––9983–95–––––044–84–
28 x7661–45––97 x––54––84 y–94 y––6796 x89 y62 x–96 y–1003498 x83 y49 y–756256 x–97––82 x––84 x–88 x––25 y59–0–19–7962 x–68 x–20 x–
92
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED201237–1–940 x5331–52 x–49 x40 x53–18–2123 x3554–62 x–88 x–24–23 y–76x66y–35 x–33 x–8–5y–2–11y–13 x–11 x–9–10 y–3–71y–15 x–12 x–
Countries and territories
% of children (2006–2010*) who are:% of under-fives (2006–2010*) suffering from:introduced tounderweightwastingstunting% of infants Early initiationbreastfed(WHO)(WHO)(WHO)with lowof breastfeeding exclusively solid, semi-solidor soft foodsbreastfedat age 2birthweight(%)moderatemoderate moderate(2006–2010*)(2006–2010*)(<6 months)(6–8 months) (20–23 months) & severesevere& severe& severe
Vitamin Asupplementationcoverage rate(6–59 months)2010full coverageΔ(%)
% ofhouseholdsconsumingiodized salt(2006–2010*)
FinlandFranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People'sDemocratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia(Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibia
115x–13 x14––4x–16131122 x196x183414 x7––54x15 x16916
EM28BAFebr RGua Ory ED201230––5344––––7258–6446–7381–1826––5434––––5172–4838–314621 x–70 y––58 y51 y––––89 y86 y–82 y30 y–77 y61 y––48––3541––––6177–6856–5347––31––1315 y–––––13131727––15 y–3––5x2x9x1823179––22y–––––3–310––3y––––1x1x2x5647––43y–––––4–1115––7y–2––3x4x10 x488––8125 x52 x637671––57 x19 x31 x372424––57 x35 x66 x84 y81 y72 y––65 x13 x15 x546528
4x––115–13–91112 x111925 x–109x4x289715–8x–12 x–1368––5
–––5366–52––5635554344–79––414456 x31–––62 x–396458––65
–––36––63––5048383341–30––463223 x25–––15 x–221732––32
–––3443 y–75 y––71 y32 y4359 y87 y–69 y––57 y75 y68 x51 y–––36 x–66 y39 y83 y––49 y
–––3117–44––46–654935–48––775058 x36–––24 x–111654––26
–––181–14––13 y21181118–8––4318–6–––2–2416––2
–––41–3–––7526–1––165–2–––––014––0
–––102–9––1y86510–1––2014–6–––2–257––3
–––2411–28––48 y40321829–29––4837–26–––4–81735––1848––3942 y––––5047171938––23 y–16––27 x7x23 x443529
–––100––93––3697100–21––––3480–––––––––62––9783–––97––––9596––99––97––––61––1009413
––36 x21100–32––764112113––––5162 y99 x28––––––9298––7684 y–92 x84–––––53501844 x79––23–91 x––83 x–212593–
Statistical tables
93
TABLE 2: NUTRITION% of children (2006–2010*) who are:% of under-fives (2006–2010*) suffering from:introduced tounderweightwastingstunting% of infants Early initiationbreastfed(WHO)(WHO)(WHO)with lowof breastfeeding exclusively solid, semi-solidor soft foodsbreastfedat age 2birthweight(%)moderatemoderate moderate(2006–2010*)(2006–2010*)(<6 months)(6–8 months) (20–23 months) & severesevere& severe& severeVitamin Asupplementationcoverage rate(6–59 months)2010full coverageΔ(%)% ofhouseholdsconsumingiodized salt(2006–2010*)
Countries and territories
NauruNepalNetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent andthe GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and TobagoTunisia
810–8–19 x6–14–7x–13––––17––9––1010 x76x12 x113x195
EM28BAFebr RGua Ory ED2012–88–45–23 x17 x–51–––752661 x––80–3444––4657 y50–8253–4187–51–51–34 x15 x–11–––7498x––76–244––4325 x15–5263–136–71 y–73 y–61 x39 x–73 y–––81 y15 y49 x––87 y–34 y––––15 x––78 y44–43 y61 y–74–20–42 x8x–50–––673531 x––84–1511––2534 x––3364–2215–––13–14 x1x–21–––12329––21–76––1015724517––3–––3–4x0x–7–––212–––4–11–––610154––––––11–9x4x–10–––4135––15–51––12753195––3
2721––92712––71232–10 x10 x68216x8x––6x8x66x811
7635––544238––––29–––475154––––65 x––68––
6753––312713––27–37––56246834––––46 x16 x–85––
65 y75 y––76 y65 y75 y––––36 y––76 y67 y80 y58 y––––18 x41 x–62 y––
6595––43–32––––55––721461 y34––––2x––84––
539––640 y23–––931 x–4y18 x3x422 y––––3x4x–11––
111––114 y9––––13 x––5x–1–––––1x1x–2––
113––116 y14–––714 x–1y5x1x17y––––5x4x–3––
2449––2247 y41–––1042 x–19 y43 x18 x2432 y––––10 x13 x–44–––––29–19 x7x–36–––334224––17–1131––283916115830––9
–91––79891––––87––14––––––––––92–––––41––––100––––––––85––38––33 w95––48100–––
––––97 x3297 x––86–17 x––9294 y91 x45 x––––60 x74 x35 x88 x–––––86–41 x32–58––––1–––92 y––52––79 x624794 x6032–28–
94
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
% of children (2006–2010*) who are:% of under-fives (2006–2010*) suffering from:introduced tounderweightwastingstunting% of infants Early initiationbreastfed(WHO)(WHO)(WHO)with lowof breastfeeding exclusively solid, semi-solidor soft foodsbreastfedat age 2birthweight(%)moderatemoderate moderate(2006–2010*)(2006–2010*)(<6 months)(6–8 months) (20–23 months) & severesevere& severe& severe
Vitamin Asupplementationcoverage rate(6–59 months)2010full coverageΔ(%)
% ofhouseholdsconsumingiodized salt(2006–2010*)
TurkeyTurkmenistanTuvaluUgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela(Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
114–1446–10 x8x951085–111131 x
3960–4241––49–606772–58305769–
4211 x356018––50–572640–1712 x613234
68 y54 x40 y80 y55 y––92 y–35 y45 y62 y–70 y76 x93 y82 y56 y
2237 x51546––51–283832–23–422035
28x216–––16–5x4–42043 x151027
02x04–––4–2x1–––19 x3210
17x36–––5–2x4–51015 x5316
1219 x1038–––42–15 x19–163158 x453240
–––––––99––94––95 w–924982
6987–9618 x––59––5323–9330 x77 x91 y11
MEMORANDUM
SUMMARY INDICATORS#AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld1313–13111827687–151615
EM28BAFebr RGua Ory ED201246455439454239454249–43474334334924343845294230–37423768698163575556547155–606860444654423169 **7644 **3322–56 **6155 **19201523112742104––18θ2516θ6748413 **155 **–––9 **89 **996119131962––101010
Sudan and South Sudanδ
383939402834471915––29θ4127θ
86868090–56 **5084 **–––66 **8866 **
555365–48745588–––716171
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Low birthweight– Percentage of infants weighing less than 2,500 grams at birth.Early initiation of breastfeeding– Percentage of infants who are put to the breast within one hour of birth.Exclusive breastfeeding (<6 months)– Percentage of children aged 0–5 months who were fed exclusivelywith breast milk in the past 24 hours.Introduction of solid, semi-solid or soft foods (6–8 months)– Percentage of children aged 6–8 monthswho received solid, semi-solid or soft foods in the past 24 hours.Continued breastfeeding at age 2 (20–23 months)– Percentage of children aged 20–23 months whoreceived breast milk in the past 24 hours.Underweight (WHO)– Moderate and severe: Percentage of children aged 0–59 months who are belowminus two standard deviations from median weight-for-age of the World Health Organization (WHO) ChildGrowth Standards; severe: Percentage of children aged 0–59 months who are below minus three standarddeviations from median weight-for-age of the WHO Child Growth Standards.Wasting (WHO)– Moderate and severe: Percentage of children aged 0–59 months who are below minustwo standard deviations from median weight-for-height of the WHO Child Growth Standards.Stunting (WHO)– Moderate and severe: Percentage of children aged 0–59 months who are below minustwo standard deviations from median height-for-age of the WHO Child Growth Standards.Vitamin A supplementation (full coverage)– The estimated percentage of children aged 6–59 monthsreached with two doses of vitamin A supplements.Iodized salt consumption– Percentage of households consuming adequately iodized salt(15 parts per million or more).
MAIN DATA SOURCES
Low birthweight– Demographic and Health Surveys (DHS), Multiple Indicator Cluster Surveys (MICS),other national household surveys, data from routine reporting systems, UNICEF and WHO.Breastfeeding– DHS, MICS, other national household surveys and UNICEF.Underweight, wasting and stunting– DHS, MICS, other national household surveys, WHO and UNICEF.Vitamin A supplementation– UNICEF.Iodized salt consumption– DHS, MICS, other national household surveys and UNICEF.
– Data not available.w Identifies countries with national vitamin A supplementation programmes targeted towards a reducedage range. Coverage figure is reported as targeted.x Data refer to years or periods other than those specified in the column heading. Such data are notincluded in the calculation of regional and global averages. Estimates from data years prior to 2001are notdisplayed.y Data differ from the standard definition or refer to only part of a country. Such data are included in thecalculation of regional and global averages.ΔFull coverage with vitamin A supplements is reported as the lower percentage of two annual coveragepoints (i.e., lower point between round 1 (January–June) and round 2 (July–December) of 2010).* Data refer to the most recent year available during the period specified in the column heading.** Excludes China.θModel-based estimate.
NOTES
Statistical tables
95
TABLE 3: HEALTH% of populationusing improveddrinking watersources2008Countries and territories% of populationusing improvedsanitationfacilities2008% of routineEPI vaccinesfinanced bygovernment2010total% under-fives withsuspected % under-pneumonia fives with1-year-old children immunized against:taken to an suspected%appropriate pneumoniaTBDPTPolio Measles HepB Hib newborns health care receivingprotectedprovider antibioticscorresponding vaccines:againstββλ2006–2010*BCg DPT1 DPT3 polio3 measles HepB3 Hib3 tetanusImmunization 2010% under-fives withdiarrhoeareceivingoral rehy-dration andcontinuedfeeding2006–2010*Malaria 2006–2010*%% of%under-fiveshouse- under- with feverholdsfivesreceivingwith at sleepinganti-least one undermalarialITNITNsdrugs
total urban rural total urban rural
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republic of the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFiji
48978310050–979610010080––8010010010099759286999597–100767261741008467509689929571–97809994100100
78968510060959898100100889810085100100100998499961009999–100958381921008592679998999195981009310096100100
39987910038–809310010071––7810099100100698867989084–10072715651998251447582739734–91689789100100
37989510057–909010010081100–531009310090126525956080–100114629471005434996557436301009523999110098
6098981008698919510010085100100561009110093248734997487–1003349675610065432398588150311009536999410099
30988810018–778010010077100–5210097100864549923937–1006461835993828483525530291009611988110097
210010010029–10066–––10010029100––100185––100100––3394096–––65––100––9010055–9921–
689999–93–9995––81––94–99–98979690979999959899939496–99745295998476959977919999––
86999999979998989793809999989599999994948795989998969899939292996471939996819099969598989999
66999599919894949283729999958698999683918090969895949596928480995459929988749099888596969999
66999599929996969283789799959099999683928090969999969494928380994763929988829099938196999999
62999599939899979476679499948599949869957993949994979492937993966246939988727699837095998798
66999596919894949283499899958696979683918090939696959596928417985459929988819099898597969699
66999598919894489283–989995860979683–8080–9995919596928480–545992–88819099908596969699
798790–75––––––909493–––88928974–929295–85949191–928660––798583––82––––
–7053––––57–––––37–90 x–713674519114 x50––3938 x6435––3226––6456 x48 x––35––––
–6059––––––––––––67 x–44–496473––––1526 x–38––3931–––––––19––––8842–43–57–5851–––5x–
–6324–––––––31––68–54 x–26426229537x–––4223 x–22––4723––5231 x39 x––45––––6737–33–55–19–36 x54 x–15 x–
––––28–––––––––––––25–––––––23525x4––1642––3x–8x––10–––––49–30––––––71–53–
––––18–––––1x–––––––20–––––––10454x13––1510–––9x6x––3–––––36–20–––––1x49–33–
––––29–––––1x–––––––54–––––––48170x58––5736–––63 x48 x––36–––––39–1–––––49 x13–10–
100 100 100 –––46 80 28 23 23 23100 100 100 100 100 10092 98 52 56 63 10––– –––86 87 84 83 87 7494 97 88 92 96 8499 100 98 94 97 9287 94 76 87 89 83––– –––61 74 57 14 52498 99 97 95 96 9438 98 26 12 298––– –––
96
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012210–2610010010075–10014–5–9885–909998999891739997699994679390999699979765999690999363908898889997923399948699997290889986999792399994869999688585997998969251999581949363–889884989792–99948699–639088988199–92–999486999177–79–877486887593–88948040–62–70–7367–44 x–19 x–
% of populationusing improveddrinking watersources2008Countries and territories
% of populationusing improvedsanitationfacilities2008
% of routineEPI vaccinesfinanced bygovernment2010total
total urban rural total urban rural
% under-fives withsuspected % under-pneumonia fives with1-year-old children immunized against:taken to an suspected%appropriate pneumoniaTBDPTPolio Measles HepB Hib newborns health care receivingprotectedprovider antibioticscorresponding vaccines:againstββλ2006–2010*BCg DPT1 DPT3 polio3 measles HepB3 Hib3 tetanusImmunization 2010
% under-fives withdiarrhoeareceivingoral rehy-dration andcontinuedfeeding2006–2010*
Malaria 2006–2010*%% of%under-fiveshouse- under- with feverholdsfivesreceivingwith at sleepinganti-least one undermalarialITNITNsdrugs
FinlandFranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People's Democratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia (Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibiaNauru
10010087929810082100–9471619463–861001008880–7910010010094100969559–999057991008568–––1004180100915610094499994–10076988147719290
100100959610010090100979889839871–951001009689989110010010098100989983–9999721001009779–––1007195100998110092521009695100971009877759990
1001004186961007499–9061519355–771001008471–5510010010089100919052–998551961008151–––100297799864410099479987––499660296988–
1001003367951001398978119218117–711001003152–7399100–83100989731–100935378–291797––100115696983610073269185–10050926917813350
1001003368961001899968934498524–801001005467–76100100–82100989727–100948682100402597––1001551961004510083509390–10064968338866050
10010030659310079797731198010–621001002136–6698100–84100979832–100933871–25496––10010579596321005399068––32865247917–
100–100–80–––10010024–100––63100100100–––100–100100–100–48–100855100100–6––100–5368010020–31110010030–80100–24–100–
––899596–9991–9981939875–9999–8797998096––95999596998798987292–958099–99–6797999786–99859998708999959990938899
9999699999979699999675929983–999998839499819896989999989993979899819783937598–989978979897909799829996909998979977938799
9999459891939499979457769559–989996728399659496969998989983919896748974836498–959974939496767694649995859996949974908399
9999449688959499949453739559–989996709399699494969998989883959888768974917198–959972869497737695639995859996939973908399
9890559794969399959351619559–999993748999739098908894989986899899649353856498–969667939697637397679995809997909870887599
–424594959094959794577695––98––3783996494969699–989983919996748974836498–949474939597768697649993889996909874908399
98974598679494839794577695––989996––––94939599–989683919896748874836498–9598749394–777692649995709996909974–8399
––7591––86––8590789770–94––87859580–––80–87–78–95–80––8391––––7687879585––879588––––89839383–
––48 x6974 x–51––64 x42 x526431–56––696693 x82–––75 x–757156––6232–74 x6662––––4252––38––45––––63 x89 x38 x6566 x–69
–––6156 x–24––––35203–54––13––82–––52 x–793250––4552–––––––––30–––––24––––71 x57 x–22––47
––44 x3837 x–45–––38 x532843 x–49––3354–64–––39 x–324843––2249––4847––––4927–6338––32––––47 x64 x46 x4765 x4868
––7050––33–––853–––––––3–––––––––56–––45–––47––––5760––85––12–––––––31–54–
––5549––28–––536–––––––3–0x–––––––47–––41–––26––––4657––70––––––––––23–34–
–––63––43–––7451–5–1––81–1x–––––––23–––8–––67––––2031–––––21–––––––37–20–
EM28BAFebr RGua Ory ED2012
Statistical tables
97
TABLE 3: HEALTH% of populationusing improveddrinking watersources2008Countries and territories% of populationusing improvedsanitationfacilities2008% of routineEPI vaccinesfinanced bygovernment2010total% under-fives withsuspected % under-pneumonia fives with1-year-old children immunized against:taken to an suspected%appropriate pneumoniaTBDPTPolio Measles HepB Hib newborns health care receivingprotectedprovider antibioticscorresponding vaccines:againstββλ2006–2010*BCg DPT1 DPT3 polio3 measles HepB3 Hib3 tetanusImmunization 2010% under-fives withdiarrhoeareceivingoral rehy-dration andcontinuedfeeding2006–2010*Malaria 2006–2010*%% of%under-fiveshouse- under- with feverholdsfivesreceivingwith at sleepinganti-least one undermalarialITNITNsdrugs
total urban rural total urban rural
NepalNetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent and the GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and TobagoTunisiaTurkeyTurkmenistan
88100100854858100100918890–9340868291100991009890–96659998–––89–6999–4910010099–3091–10090–93691001008970100
93100100989675100100919295–97879990931009910010096–98779998–––8997929910086100100100–6799–10098–97921001009494100
87100100683942100100917787–83336661871001001008885–89629998–––88–5298–26–10099–978–10088–8161100100846199
31100–5293210010089–45–6945706876901001001007972875496––100–26–5192–13100100100–2377–10091–8455100100969489
51100–633436100100919772967571908180961001001008588935096––100–3010069969724100100100985284–10088–9061100100969592
27100–3742810010084–29–5141403669801001001007454705596–96100–19–3888–6–99100–665–10092–6653100100959482
39100100411471100100––10009059100100–100100–4858100–25100100100100–6–100–100––100–450100–10057–100––0––95
94––98837699–999995–9779929590949699969899967591979091–9998809999999998–852986––99––9823–908299
859995998077999998999099988096978999999896939999929898999795989880979996989998855573–9999–99959998899599
829793987069999396998849945690938799989794909797809597998792989870919990979996794563–9799–88899896809399
839793997579999397998848946188928696979895979698809097998692989870919989979996784967–9799–88899895839599
869691997171999398978675955594948898969998979598829995996193929860959982959895684665–9599–89949690829498
82–9098706699–959888809456989385989797949898978096979987929898708999909699–79–56–9799–8889––849398
–97899870–99949699886694569893–999797–63––809697998792989870919990–999679–45–9799–868998948093–
81––818469–––9184––61858575–––––––85–––––––88––85–––856477––86–9386––94–91
43––58 x4745––65 x–69––63–6850––––60 x––28–––––75–47 x93 x–46–––731365 x––58–7473––7764 x8493 x71––7459–83
25––––23––––50––––5142–––––––13––––––––57 x–27–––2332–––––3724––7141 x6574 x4541–34––50
37––49 x3425––––37–––––60––––48 x––––––––––43 x71 x–57––––7–––67–2822––3422 x4645 x6324––622225
––––7642––––0–––––––––––––82–––––61–60––37–––4912–53–5––4––––––4156–––––
––––6429––––––––––––––––––70–––––56–29––26–––4011–25–3–3x1––––––4157–––––
0––2x–49––––3–––––0x–––––––11–––––8–9––30–––198–36–0––1–––2x––634–––––
98 99 98 9669 86 63 5060 87 41 12100 100 100 9694 98 93 9294 99 84 8599 100 96 90– 97– 98
98
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED20129576249892969799964039692647597–100890100–––98719499–9896999875979996989799957292999098969695729299919896969866849992979799907292999098949689–929990–9658–8181––9690–
% of populationusing improveddrinking watersources2008Countries and territories
% of populationusing improvedsanitationfacilities2008
% of routineEPI vaccinesfinanced bygovernment2010total
total urban rural total urban rural
% under-fives withsuspected % under-pneumonia fives with1-year-old children immunized against:taken to an suspected%appropriate pneumoniaTBDPTPolio Measles HepB Hib newborns health care receivingprotectedprovider antibioticscorresponding vaccines:againstββλ2006–2010*BCg DPT1 DPT3 polio3 measles HepB3 Hib3 tetanusImmunization 2010
% under-fives withdiarrhoeareceivingoral rehy-dration andcontinuedfeeding2006–2010*
Malaria 2006–2010*%% of%under-fiveshouse- under- with feverholdsfivesreceivingwith at sleepinganti-least one undermalarialITNITNsdrugs
Tuvalu97 98 97 84Uganda67 91 64 48Ukraine98 98 97 95United Arab Emirates100 100 100 97United Kingdom100 100 100 100United Republic of Tanzania54 80 45 24United States99 100 94 100Uruguay100 100 100 100Uzbekistan87 98 81 100Vanuatu83 96 79 52Venezuela (Bolivarian Republic of) ––– –Viet Nam94 99 92 75Yemen62 72 57 52Zambia60 87 46 49Zimbabwe82 99 72 44
88 8138 4997 9098 95100 10032 21100 99100 99100 10066 48––94 6794 3359 4356 375518
236–––18–100––100282019055
99849598–99–999981929465899090
99839694989899989978909394999499
89609094969195959968789387828390
89559194989493959967749488668490
85559494939292959852799873918490
89608494–9192959959788887828375
896081949791939599–786387828375
–85–––83–––73508766907674
–73–––71––68–72 x83–684390
–47––––––56––55384716–
–39–––50––284351 x6548563556
–47–––64–––––19–642718
–33–––64–––––––501728
–60–––59–––––3–342454
MEMORANDUMSudan and South Sudanδ576452 34
SUMMARY INDICATORS#AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld
65 8560 8359 8761 8286 9387 9686 9588 9693 9794 98100 10084 9462 8087 96
EM28BAFebr RGua Ory ED2012524747467682838180889876547841 5531 4436 5527 3580 9049 6335 5760 6680 8689 9399 10052 6836 5061 76322428216640265555829840314546413149–84 **90–99––76 **2377 **85848583929288979696–90849086858980959085969697989088917977807291847694939595848085817979789284759693969584808678757971908577959396938478857774787189705194909466757875596177464816227925785387342807983778486 **8784 **84––84 **8384 **535158427666 **6666 **55––61 **5161 **
3531–286223 **18––––30 **–30 **
363743324041 **3757 **–––39 **4639 **
44445140––––––––47–
34344030––––––––37–
39393045–6 **71 **–––19 **3419 **
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
% of population using improved drinking water sources– Percentage of the population using any of thefollowing as their main drinking water source: drinking water supply piped into dwelling, plot, yard or neighbor’s yard;public tap or standpipe; tube well or borehole; protected dug well; protected spring; rainwater; bottled water plus oneof the previous sources as their secondary source.% of population using improved sanitation facilities– Percentage of the population using any of the followingsanitation facilities, not shared with other households: flush or pour-flush latrine connected to a piped seweragesystem, septic tank or pit latrine; ventilated improved pit latrine; pit latrine with a slab; covered pit; composting toilet.government funding of EPI vaccines– Percentage of EPI vaccines that are routinely administered in a country toprotect children and are financed by the national government (including loans).EPI– Expanded programme on immunization: The immunizations in this programme include those against tuberculosis(TB); diphtheria, pertussis (whooping cough) and tetanus (DPT); polio; and measles, as well as vaccination of pregnantwomen to protect babies against neonatal tetanus. Other vaccines, e.g., against hepatitis B (HepB), Haemophilusinfluenzae type b (Hib) or yellow fever, may be included in the programme in some countries.BCg– Percentage of live births who received bacille Calmette-Guérin (vaccine against tuberculosis).DPT1– Percentage of surviving infants who received their first dose of diphtheria, pertussis and tetanus vaccine.DPT3– Percentage of surviving infants who received three doses of diphtheria, pertussis and tetanus vaccine.Polio3– Percentage of surviving infants who received three doses of the polio vaccine.Measles– Percentage of surviving infants who received the first dose of the measles-containing vaccine.HepB3– Percentage of surviving infants who received three doses of hepatitis B vaccine.Hib3– Percentage of surviving infants who received three doses of Haemophilus influenzae type b vaccine.Tetanus– Percentage of newborns protected at birth against tetanus.% under-fives with suspected pneumonia taken to an appropriate health care provider– Percentage ofchildren (aged 0–4 years) who were suspected of having pneumonia in the two weeks preceding the survey and whowere taken to an appropriate health care provider.% under-fives with suspected pneumonia receiving antibiotics– Percentage of children (aged 0–4 years) whowere suspected of having pneumonia in the two weeks preceding the survey and who were receiving antibiotics.% under-fives with diarrhoea receiving oral rehydration and continued feeding– Percentage of children(aged 0–4 years) who had diarrhoea in the two weeks preceding the survey and who received oral rehydrationtherapy (a packet of oral rehydration salts, recommended home-made fluids or increased fluids) and continued feeding.
Malaria:% of households with at least one ITN– Percentage of households with at least one insecticide-treated mosquito net.% under-fives sleeping under ITNs– Percentage of children (aged 0–4 years) who slept under an insecticide-treatedmosquito net the night prior to the survey.% under-fives with fever receiving antimalarial drugs– Percentage of children (aged 0–4 years) who were illwith fever in the two weeks preceding the survey and received any antimalarial medicine. This indicator refers toantimalarial treatment among all febrile children, rather than among confirmed malaria cases, and thus should beinterpreted with caution. For more information, please refer to <www.childinfo.org/malaria_maltreatment.php>.
MAIN DATA SOURCES
Use of improved drinking water sources and improved sanitation facilities– UNICEF and World HealthOrganization (WHO) Joint Monitoring Programme for Water Supply and Sanitation.government funding of vaccines– As reported by governments on UNICEF and WHO Joint Reporting Form.Immunization– UNICEF and WHO.Suspected pneumonia care seeking and treatment– Demographic and Health Surveys (DHS), Multiple IndicatorCluster Surveys (MICS) and other national household surveys.Diarrhoea treatment– DHS, MICS and other national household surveys.Malaria prevention and treatment– DHS, MICS, Malaria Indicator Surveys (MIS) and other national household surveys.
NOTES
– Data not available.x Data refer to years or periods other than those specified in the column heading. Such data are not includedin the calculation of regional and global averages. Estimates from data years prior to 2000 are not displayed.βCoverage for DPT1 should be at least as high as DPT3. Discrepancies where DPT1 coverage is less than DPT3 reflectdeficiencies in the data collection and reporting process. UNICEF and WHO are working with national and territorialsystems to eliminate these discrepancies.λWHO and UNICEF have employed a model to calculate the percentage of births that can be considered as protectedagainst tetanus because pregnant women were given two doses or more of tetanus toxoid (TT) vaccine. Themodel aims to improve the accuracy of this indicator by capturing or including other potential scenarios wherewomen might be protected (e.g., women who receive doses of TT in supplemental immunization activities). A fullerexplanation of the methodology can be found at <www.childinfo.org>.* Data refer to the most recent year available during the period specified in the column heading.** Excludes China.
Statistical tables
99
TABLE 4: HIV/AIDSMother-to-childPaediatricPrevention amongtransmissioninfectionsyoung people (aged 15–24)Estimated numberof people (all ages)HIV% who have% who usedEstimatedEstimated number Estimated numberliving with HIV,prevalencecomprehensive condom at lastadult (agedof women (aged of children (aged2009 (thousands)among youngknowledge of higher-risk sex,15–49) HIV15+) living with 0–14) living withpeople (%), 2009HIV, 2005–2010*2005–2010*lowhighprevalenceHIV, 2009HIV, 2009total male female male female male female(%), 2009 estimate estimate estimate(thousands)(thousands)Children(aged 0–17)orphaned byAIDS, 2009estimate(thousands)OrphansChildren(aged 0–17)orphaned due toall causes, 2009estimate(thousands)Orphanschoolattendanceratio2005–2010*
Countries and territories
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republicof the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFiji
––0.1–2.0–0.50.10.10.30.13.1–<0.11.40.30.22.31.20.20.2–24.8––0.11.23.30.55.30.3–4.73.40.40.10.50.13.4–0.33.4<0.10.1–<0.1––0.22.5–0.90.4<0.10.85.00.81.2–0.1
––18–200–1102201547–621714560<1.012–320––41101806361068–13021040740160<0.577–10450<1.07–2––514–57371134202510–<1.0
––13–160–882151233–521311452<1.09–300460–3911604254053–11017032540120<0.268–8390<1.06–2–430410–492882514188–<0.5
––24–250–14022520511–832018669216–350810–51401909067083–140300511,000210<0.587–1351019–2–560618–66501744263312–<1.0
––5–110–36<1.06524–2<1.084332<0.54–170––156903532021–671101223050<0.140–3220<0.52–<1.0––17–321121111133–<0.2
––––22–––––––––––––5–––16–––1728–54––1723––––8––––––––––––––––23–––
––<0.1–1.1–0.2<0.10.10.20.12.2–<0.11.00.1<0.11.30.50.10.1–8.5––<0.10.61.50.12.70.1–1.61.70.2–0.2<0.11.9–0.21.1<0.10.1–<0.1––0.11.3–0.50.2<0.10.33.50.30.2–0.1
––0.1–0.6–0.3<0.10.10.3<0.11.4–<0.10.9<0.1<0.10.70.30.10.1–5.2––<0.10.51.00.11.60.1–1.01.00.2–0.2<0.11.2–0.20.7<0.10.1–<0.1–
––<0.1–1.6–0.2<0.10.10.20.13.1–<0.11.10.1<0.11.80.7<0.10.1–11.8––<0.10.82.10.13.90.1–2.22.50.1–0.1<0.12.6–0.11.5<0.10.1–<0.1–
–22––32––15––5––18––––35–28––––15––45––3626–––––22––28–––––––––34–18––––33–
–3613–25––23––5––8–34–4016212444–––1719305032–361710––24–8––18–54––815–18–41–527–––20–
–55–––––86––31–––––––45–49––––70––84––7960–––––38––53–––––––51–70––––––50–
–25–––––––––––––––502862–71–––576425–62–564128––45–20––39–71–––6–26–44––––––28–
––––140–––––––––––––30–––93–––140200–330––140120–––<0.151––––––––––––––––419–––
––550–1,500–6304680281907–4,800215047631021320–130––947706106301,20045–370670140–82022220–361,1004486–92––5147–1902101,7001504524019–23
––––85––––––––84––––90–––––––61 p858391––96117––85–88––83–––––74–––77––––––90–
100
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012––0.1 0.10.8 1.9––0.3 0.70.2 0.2<0.1 <0.10.4 0.31.9 5.00.2 0.40.3 0.2––0.1 0.1
Countries and territories
Mother-to-childPaediatricPrevention amongtransmissioninfectionsyoung people (aged 15–24)Estimated numberof people (all ages)HIV% who have% who usedEstimatedEstimated number Estimated numberliving with HIV,prevalencecomprehensive condom at lastadult (agedof women (aged of children (aged2009 (thousands)among youngknowledge of higher-risk sex,15–49) HIV15+) living with 0–14) living withpeople (%), 2009HIV, 2005–2010*2005–2010*lowhighprevalenceHIV, 2009HIV, 2009total male female male female male female(%), 2009 estimate estimate estimate(thousands)(thousands)
Children(aged 0–17)orphaned byAIDS, 2009estimate(thousands)
OrphansChildren(aged 0–17)orphaned due toall causes, 2009estimate(thousands)
Orphanschoolattendanceratio2005–2010*
FinlandFranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People'sDemocratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia(Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibia
0.20.70.123.61.5––0.10.30.211.00.5<0.11.00.1–0.71.00.3––<0.1–0.111.50.613.1
99429037––1<1.024920100<0.176<0.5–149220––<0.5–261,400240180
EM28BAFebr RGua Ory ED201266326032––<1.0<1.01983083<0.161<0.5–1161801312531043––21301,000120<0.196<0.5–1712280––<1.0–341,50029021043116019––<0.5<0.5747011<0.140<0.1–4359––<0.2–87608195–––286–––––120–––––––––––––130–160.20.10.19.90.5––<0.10.10.14.90.1<0.10.4<0.1–0.40.30.2––<0.1–0.15.90.34.00.10.20.15.40.3––<0.10.10.13.10.1<0.10.2<0.1–0.40.30.20.20.1<0.114.20.7––<0.10.10.16.8<0.1<0.10.5<0.1–0.30.20.1–––2927––––2642––––3914–––––––34–62–––3921––––2342–35y15–275––––3130–363265–––6822–––––58––––22––––––6614–––––40––15–9–––
0.10.45.22.00.10.11.80.1–0.81.32.51.21.9–0.8<0.10.30.30.20.2–0.20.20.31.7<0.1–0.16.3––0.3
315046184672609–6279226120–393<1.02,40031092–78140328–131,500––10
212037123562307–4765183110–262<0.52,10020074–56110216–91,300––7
3190552657530011–8295269140–514<1.02,800460120–9101804510–191,600––16
<1.04825102121403–204112367–12<1.0<0.28808826–2248103–8760––3
––3–––27–––92–12–––––––––––––––180–––
<0.10.22.41.6<0.10.10.90.1–0.40.71.40.70.9–0.3<0.10.10.1<0.1<0.1–0.10.1<0.10.9<0.1–0.12.9––0.1
0.10.21.40.9<0.10.10.50.1–0.50.40.80.60.6–0.3<0.10.10.10.1<0.1–0.10.1<0.11.0<0.1–0.11.8––0.1
<0.10.13.52.4<0.1<0.11.30.1–0.30.92.00.81.3–0.2<0.10.10.1<0.1<0.1–0.1<0.1<0.10.7<0.1–0.24.1––0.1
––––––34––2423–4740––––3615 y–––––––––55–––
–––3915–28––2217155434–30––2010y–3–––60–13y2248––20
––––––46–––37–7843––––37––––––––––64–––
–––54––28–––26475629–24––22––––––––––40––56
––183––160–––5910–––––––––––––––––1,200––––––13052––––11650––59––4<0.1––––––670–70
45<0.16472683801,10073–38044011030440–150130231,0004,7001,200–398<0.173<0.1–4202,600––1402203270200340––5249101,00045076903–120191,500––67–6502,1001,600120
–––87––76–––73109–86–108––72––84––––––––––––––9885––––7497––92––66 p––––96 p––83–100
––<0.5–191,200200150
––––<0.1 <0.1––0.1 0.13.1 8.60.3 0.32.3 5.8
–––––––81
–––66–44–64
Statistical tables
101
TABLE 3: HEALTH4: HIV/AIDSMother-to-childPaediatricPrevention amongtransmissioninfectionsyoung people (aged 15–24)Estimated numberof people (all ages)HIV% who have% who usedEstimatedEstimated number Estimated numberliving with HIV,prevalencecomprehensive condom at lastadult (agedof women (aged of children (aged2009 (thousands)among youngknowledge of higher-risk sex,15–49) HIV15+) living with 0–14) living withpeople (%), 2009HIV, 2005–2010*2005–2010*lowhighprevalenceHIV, 2009HIV, 2009total male female male female male female(%), 2009 estimate estimate estimate(thousands)(thousands)Children(aged 0–17)orphaned byAIDS, 2009estimate(thousands)OrphansChildren(aged 0–17)orphaned due toall causes, 2009estimate(thousands)Orphanschoolattendanceratio2005–2010*
Countries and territories
NauruNepalNetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent andthe GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and TobagoTunisia
–––––0.90.1–1.60.1<0.1<0.1–0.717.8–0.4<0.1–1.025.90.10.4–0.21.3––3.2–1.5<0.1
–––––595–493<0.5<1.0–345,600–1303–4180818–9530––120–152
EM28BAFebr RGua Ory ED2012–––––504–403<0.5<0.5–255,400–1202–3170613–6420––99–112–––––697–634<0.5<1.0–485,900–1504–52001124–13660––150–193–––––321–281<0.1<0.2–153,300–32<1.0–110036–3210––67–5<1.0––––––––3–––––330–––––14–––––––11––––––––0.50.1–1.0<0.1<0.1<0.1–0.59.0–0.1<0.1–0.511.0<0.10.2–<0.1––––––0.30.1–0.6<0.1<0.1<0.1–0.44.5–0.2<0.1–0.66.5<0.10.2–<0.1––––––0.70.1–1.5<0.1<0.1<0.1–0.613.6–0.1<0.1–0.415.6<0.10.1–<0.1––6–43–24––28–––35–––––––54–––13––20–––––3–43–1942–17–––294–––––4158––71446271215–54––––64–52––22–––26–––––––91–––––––––––– ––– ––1.5 0.9 2.2– ––0.9 1.0 0.7<0.1 <0.1 <0.1
–0.40.20.10.20.83.6–0.1–0.10.1–0.90.90.30.4<0.10.10.6<0.1<0.10.40.11.02.9––
–642237613,300–4–198–2034137592742<0.2101216980170––
–511725562,900–3–<1.079–1430105862032<0.171012840140––
–803239663,600–5–1120–363916100133453<0.21316201,200190––
–207<1.02281,700–1–<0.528–6184183813<0.135548088––
––––––360–––––––3––––––––––22––
–0.20.1<0.10.10.42.0–<0.1–<0.10.1–0.30.60.20.2<0.1<0.10.2<0.1<0.10.1<0.1–1.6––
–0.20.1<0.10.10.21.2–<0.1–<0.10.1–0.40.30.20.2<0.1<0.10.3<0.1<0.10.10.10.21.3––
–0.1<0.1<0.10.10.52.9–<0.1–<0.1<0.1–0.30.80.10.1<0.1<0.10.2<0.1<0.10.1<0.10.31.9––
1044–––1633–––––––––––––––39 y––54––
1328–––1322––––3––––1921––––42y––51––
1778–––3749–––––––50–––––––76––40––
10––––18 y36–––––––35–3313––––60––26–––––54–3674–10–––17––––––4973–––––70–50–51–
–––––572,500––––––––––––––––––130–––––––19––15–––––1,900–––––69–––––––66–––
–650823612097012,000–35–414,200–532601505501,900440581428079290–690–––––––52094–320175412–6303,400–<0.1340–1210063<0.1–2201,400––240–25130
–––––67117––––––––––––––––––82–––––––83––62––––78––––––99––––93–7594–––
102
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
Mother-to-childPaediatricPrevention amongtransmissioninfectionsyoung people (aged 15–24)Estimated numberof people (all ages)HIV% who have% who usedEstimatedEstimated number Estimated numberliving with HIV,prevalencecomprehensive condom at lastadult (agedof women (aged of children (aged2009 (thousands)among youngknowledge of higher-risk sex,15–49) HIV15+) living with 0–14) living withpeople (%), 2009HIV, 2005–2010*2005–2010*lowhighprevalenceHIV, 2009HIV, 2009total male female male female male female(%), 2009 estimate estimate estimate(thousands)(thousands)
Children(aged 0–17)orphaned byAIDS, 2009estimate(thousands)
OrphansChildren(aged 0–17)orphaned due toall causes, 2009estimate(thousands)
Orphanschoolattendanceratio2005–2010*
TurkeyTurkmenistanTuvaluUgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela(Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
<0.1––6.51.1–0.25.60.60.50.1––0.4–13.514.31.1
5––1,200350–851,4001,2001028––280–9801,200260
3––1,100300–661,300930818––220–8901,100210
6––1,300410–1101,5001,7001246––350–1,1001,300330
1––610170–2673031038––81–490620140
–––150–––160–––––––120150–
<0.1––3.60.2–0.12.80.20.2<0.1–
<0.1 <0.1––––2.3 4.80.2 0.3––0.2 0.11.7 3.90.3 0.20.3 0.2<0.1 <0.1–––0.1–8.96.91.3
––613843––43–––––––41––
–5393245––48––3115–442y3853–
––44 y5571––49–––––68–3968–
–––3868––46––61––––3342–
–––1,200–––1,300–––––––6901,000–
1,200––2,700810–4903,0002,10049780––1,400–1,3001,4002,000
–––9698––90–––––––9295–
– –0.1 0.1– –6.6 4.25.1 3.30.9 0.5
Sudan and South Sudanδ
SUMMARY INDICATORS#AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld3.94.87.12.80.20.20.20.20.40.70.40.92.00.8
23,30023,20016,4006,5004004,8002,5002,3001,6001,5002,20030,00010,10034,000
EM28BAFebr RGua Ory ED201221,90021,90015,6006,1003004,3002,2001,9001,4001,3001,90028,2009,30031,60024,60024,50017,3007,1004905,3002,9002,6001,9001,7002,70031,50010,70035,20011,80011,8008,4003,3001601,60090072059050056014,1004,90015,1003,1003,1002,2009003018011069571823,4001,6003,4001.92.23.21.40.10.10.10.10.20.40.10.51.00.41.11.31.90.80.10.10.10.10.20.40.20.30.60.32.73.24.52.10.10.10.10.10.20.40.10.61.40.633353930–32 **34––––32 **30–24263420–19**1724**–––20**2221**51515447–40 **38–––––––
MEMORANDUM
33333731–22 **22––––27 **30–
15,00015,00010,1004,7002001,1005805407308611016,9007,40017,100
57,60055,10026,60026,4005,70073,20043,00030,6009,8006,6004,400145,00041,700153,000
92928994–74 **73––––81 **85–
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Estimated adult HIV prevalence– Percentage of adults (aged 15–49) living with HIV as of 2009.Estimated number of people living with HIV– Estimated number of people (all ages) living with HIV as of 2009.Estimated number of women living with HIV– Estimated number of women (aged 15+) living with HIV as of 2009.Estimated number of children living with HIV– Estimated number of children (aged 0–14) living with HIVas of 2009.HIV prevalence among young people– Percentage of young men and women (aged 15–24) living with HIVas of 2009.Comprehensive knowledge of HIV– Percentage of young men and women (aged 15–24) who correctlyidentify the two major ways of preventing the sexual transmission of HIV (using condoms and limitingsex to one faithful, uninfected partner), who reject the two most common local misconceptions about HIVtransmission and who know that a healthy-looking person can be HIV-positive.Condom use at last higher-risk sex– Percentage of young men and women (aged 15–24) who say theyused a condom the last time they had sex with a non-marital, non-cohabiting partner, of those who have hadsex with such a partner during the past 12 months.Children orphaned by AIDS– Estimated number of children (aged 0–17) who have lost one or both parentsto AIDS as of 2009.Children orphaned due to all causes– Estimated number of children (aged 0–17) who have lost one orboth parents due to any cause as of 2009.Orphan school attendance ratio– Percentage of children (aged 10–14) who have lost both biologicalparents and who are currently attending school as a percentage of non-orphaned children of the same agewho live with at least one parent and who are attending school.
MAIN DATA SOURCES
Estimated adult HIV prevalence– Joint United Nations Programme on HIV/AIDS (UNAIDS),Report on the Global AIDS Epidemic,2010.Estimated number of people living with HIV– UNAIDS,Report on the Global AIDS Epidemic,2010.Estimated number of women living with HIV– UNAIDS,Report on the Global AIDS Epidemic,2010.Estimated number of children living with HIV– UNAIDS,Report on the Global AIDS Epidemic,2010.HIV prevalence among young people– UNAIDS,Report on the Global AIDS Epidemic,2010.Comprehensive knowledge of HIV– AIDS Indicator Surveys (AIS), Demographic and Health Surveys (DHS),Multiple Indicator Cluster Surveys (MICS) and other national household surveys; HIV/AIDS Survey IndicatorsDatabase, <www.measuredhs.com/hivdata>.Condom use at last higher-risk sex– AIS, DHS, MICS and other national household surveys, HIV/AIDSSurvey Indicators Database, <www.measuredhs.com/hivdata>.Children orphaned by AIDS– UNAIDS,Report on the Global AIDS Epidemic,2010.Children orphaned due to all causes– UNAIDS estimates, 2010.Orphan school attendance ratio– AIS, DHS, MICS and other national household surveys; HIV/AIDS SurveyIndicators Database, <www.measuredhs.com/hivdata>.
– Data not available.y Data differ from the standard definition or refer to only part of a country. Such data are includedin the calculation of regional and global average.p Proportion of orphans (aged 10–14) attending school is based on small denominators(typically 25–49 unweighted cases).* Data refer to the most recent year available during the period specified in the column heading.** Excludes China.
NOTES
Statistical tables
103
TABLE 5: EDUCATIONyouth (15–24 years)literacy rate (%)2005–2010*Countries and territoriesmalefemalePre-primary schoolparticipationPrimary school participationSecondary school participationNumber per 100gross enrolment gross enrolment Net enrolment Net attendance Survival rate to lastNet enrolment Net attendancepopulationratio (%)ratio (%)ratio (%)ratio (%)primary grade (%)ratio (%)ratio (%)20102007–2010*2007–2010*2007–2010*2005–2010* 2006–2009* 2005–2010* 2007–2010*2005–2010*admin.surveymobileInternetphonesusersmale female male female male female male femaledatadatamale female male female
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republicof the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFiji
–9994–81–99100––100–10074–100––65809910094971009847778989–9772549999978687–9872100100100–10069–––95978895989210056–
–9989–66–99100––100–10077–100––43689910097991009733768677–9957399999988578–9961100100100–10062–––97978295988610033–
41142927747185142125101146991251244612810811362805472801181041091413514584271752323116649422943865761449941372171241914590102871245741238116
44513811080363776733643554703279143142052641504612148230224534375536373601553690189747402427156574115
–592310045627131849823–5910–98123411414715166590813913267160415447522712–7045810581110–4973109399823594613954–
–57239735677336829924–5910–971224314147151765938031013277162515647512613–7045610580107–49731113510222616113954–
1231211118914110311797107999610310893–9810412412910810810811113210610283149120122991021041051091111201251231091108195104106104–989858113114117103117845310110795
831171049011497116100106989510310597–10010312011411010711010812310710174144113106989474741041151201141161161096695103105103–83995111198118991138044999894
–869683–92–9297–86919986–949999–8795868696969868989097–8477–9699 z9391–98–6295–99–––9447–829697955839968692
–849484–88–9498–85939893–9699100–90958888949899601008786–8257–9599 z9384–99–5295–99–––9742–839994965634978192
66 x9097–77––99––74–86 x––93–95659197978695––49728482––5656––9031 x86–9659––––9978–67–8792 y90–61 x69 x–45–
40 x9196–75––98––72–87 x––94–95589397988895––44708677––4748––9231 x87–9651––––9972–66–9093 y87–60 x64 x–45–
––93–––96––9898919867–999395–9084–––969464605469–8647–––––70–9461999595100–76996489–––7663739838–
90 x10093–83 x––100––100–99 x80–100–98899496100–88––89829287––6294 x––9519 x93––90–––––75–92–78–99––––84–
38––68–89768687–91838740–––62–4669–56788884181036–––13–83–71––76––918295–––89288852596654–3288––
15––72–87858988–94879143–––68–4969–6485918113832–––8–86–77––82––948396–––92209163606456–2391––
18 x8457–21––93––83–77 x––95–583454788936 x74––1782939––1220––7310 x39–59 y32––––9835–45–5671 y70–23 x23 x–30–
6x8265–17––95––82–85 x––97–602356758944 x80––1562637––912––7911 x40–65 y22––––9828–37–6873 y70–22 x21 x–23–
104
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
youth (15–24 years)literacy rate (%)2005–2010*Countries and territoriesmalefemale
Pre-primary schoolparticipationPrimary school participationSecondary school participationNumber per 100gross enrolment gross enrolment Net enrolment Net attendance Survival rate to lastNet enrolment Net attendancepopulationratio (%)ratio (%)ratio (%)ratio (%)primary grade (%)ratio (%)ratio (%)20102007–2010*2007–2010*2007–2010*2005–2010* 2006–2009* 2005–2010* 2007–2010*2005–2010*admin.surveymobileInternetphonesusersmale female male female male female male femaledatadatamale female male female
FinlandFranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People'sDemocratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia(Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibia
89100988670100–100–668798994797–719699––95–87789691
79100999881100–100–648699993199–649898––97–72649595
EM28BAFebr RGua Ory ED2012
––9971100–8199–896878–74–9399–881009985––10092–9910092–99100
––9760100–7999–845464–70–9599–74999980––10098–9910094–99100
15610010786731277110811712640397440–1251201096192917610513313511395107123621016192
8780792782944331112308–11659589136706754268038342193820
67109–31561116968972912–86––4087985349386–10110085–384052–7718
67108–327011072691023012–88––4186995451426–1079988–353951–7618
98109–8810810410610111011797–104––11610098–12310311110411010495102971091141149695
97108–9110810310510110411083–102––1169998–1191029410511210392102971091111199495
9699–74––7699989879–99––96969897––93969610082–939983–949184939271––87979799899497849081749399––––9293–88
9699–78––77100999569–98––98969894––8297979979–9510084–9391
––94 x4094–74–––55899148–87––8598–91–––97–999972––91
––94 x4595–75–––48869352–90––8198–80–––98–999875––93
100––61959873––6563–83––769899–8094––99100–100–99––9596679692–46–8298–494296–779183419694––94–78367083
–––9398–81–––967910085––––95––93–––99––10096––9965–93 x84 x–––––8981–9996––77––––9797–60100 x89
9598––––4891934135–––––9288–69–488885947598808751––7939827122––879182232666–37795117–72––79––164949
96100––––4491853922–––––9189–68–389187957999838748––8033857936––809385242471–23825415–74––85––145060
––34 x3989–42–––27277018–35––5957 y–46–––89–859540––8839–61 x2614––––2719–5238––21––––838439 x215847
––36 x3488–42–––17207921–43––4959 y–34–––93–899542––9132–68 x4014––––2820–6324––17––––888536 x205962
6510268323917299147143402012115648109779928125749118510031167
7683140148062912255283630325312080105249407
158977–107–97778910–69104410442–97111––573070–7–
158776–113–101758710–73105410738–99113––612953–7–
11710010410596–10898100162118951141039891101100117110–110113112121117113
1069710210486–1109610115812194108869990108100116111–110111103108115111
81949076––9297981009494957092807995100––––8888–92
81–97 x8732––––7876–8262––56–97––949791829091
77–97 x9128––––8079–8455––59–97––969888809193
Statistical tables
105
TABLE 5: EDUCATIONyouth (15–24 years)literacy rate (%)2005–2010*Countries and territoriesmalefemalePre-primary schoolparticipationPrimary school participationSecondary school participationNumber per 100gross enrolment gross enrolment Net enrolment Net attendance Survival rate to lastNet enrolment Net attendancepopulationratio (%)ratio (%)ratio (%)ratio (%)primary grade (%)ratio (%)ratio (%)20102007–2010*2007–2010*2007–2010*2005–2010* 2006–2009* 2005–2010* 2007–2010*2005–2010*admin.surveymobileInternetphonesusersmale female male female male female male femaledatadatamale female male female
NauruNepalNetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupiedPalestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent andthe GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and Tobago
–87––855278––999879–976599989710010098–999710077–––99–959974999968100–100––97–10097–9992––961009899–8599100
–77––892365––999861–967099979810010098–1009810077–––100–969756999948100–100––98–10099–9995––931009899–68100100
60311161156525550113–16659711852892100861201421321058911516633161103121917662188671291363414410810567100–11283–170621141245786101105534152141
67918310128093–6317043124342562516984404043800
96–989255317–973437––65–357248658354117757591178467
93–989556312–983338––66–357249668353117747689178268
90–1081011186995–99798592100111–1011091119711410710594100971509598
96–1061021165584–99798377103107–98109109971111051039399971519795
––9999936066–99788272–98–869791969998100919694959293
––99100944860–99778160–97–869893961009899909695979593
–86––77 x4465––91 x–70–––879688 x––––84––84––
–82––84 x3160––92 x–62–––899689 x––––85––87––
–62––4867––9998–60–87–78837598–9499959595–6793
–95––56 x8898–––––––––9590 x––––100––76–––––84–93100–94––––85–––––9274––100100991009189–98
––8795–1329–95828336–63–58–5592–65987980––85–85––3070–8995–––9132–––94–––319886708868–––––
––8897–822–95878129–69–62–6694–96948082––92–95––3576–9199–––9229–––97–––269882697777–––––
–46––35 x1345––––35–––81 x7455 x––––82––5–––51 y–30–2081–31–––29 y12–––––5631––638977794352–84
–38––47 x943––––29–––80 x7370 x––––85––5–––70 y–31–1687–25–––30 y8–––––6741––637484784841–90
106
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012070194116414107079705012–6712–328908421122152051249784310749–1151107––9486––64–129––81–1001049109224–7–81794810353–1251111––9284––65–131––81–100103989326–8–81111101921311018298105––1029910942103–10897–116112971041251049289116119–1061039994132978597107––102981062399–10797–111104961031201009089109111–102––91–88749693–––9881–89–10095–91829699–99919384––97––93–85769695–––9880–90–10096–908496100–96899482––94–88 y–86–5899–62–––63 y18–––––9583––8799 y98977191–98–89 y–85–5998–64–––69 y15–––––9486––8696 y98937387–98–––75935898––9998100––––9999–687299–9399–97–69–93
youth (15–24 years)literacy rate (%)2005–2010*Countries and territoriesmalefemale
Pre-primary schoolparticipationPrimary school participationSecondary school participationNumber per 100gross enrolment gross enrolment Net enrolment Net attendance Survival rate to lastNet enrolment Net attendancepopulationratio (%)ratio (%)ratio (%)ratio (%)primary grade (%)ratio (%)ratio (%)20102007–2010*2007–2010*2007–2010*2005–2010* 2006–2009* 2005–2010* 2007–2010*2005–2010*admin.surveymobileInternetphonesusersmale female male female male female male femaledatadatamale female male female
MEMORANDUMSudan and South Sudanδ89
83
EM28BAFebr RGua Ory ED2012
TunisiaTurkeyTurkmenistanTuvaluUgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela(Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
9899100–9010094–78–98100949897968298
9697100–8510097–76–100100949996726799
106856325381191451304790132761199617546386041
3740225132378851179432083628117120
–18––121029580335786265880––––
–17––13999481345787265674––––
109101––121971061061059811593111105–94113–78
10798––122981051061059911291105102–76112–70
–96––91899810096919991–94–8091––
–94––94899710097939989–94–6694––
95 x 93 x94 y 92 y9999––83827076––––7982––––100100808291 x95758190 y93 x95648292 y
9594––529897–74–94987192––53–
–95 x100–72100––91 x––1008882 x9873878290
–77––22858292–876693–67–––––
–70––21858495–897391–75–––––
–65 y84–1785––26––913830 x7848384517 y
–57 y84–1785––24––903643 x8027364522 y
28
29
56 y
52 y
86
SUMMARY INDICATORS#AfricaSub-Saharan AfricaEastern andSouthern AfricaWest and Central AfricaMiddle Eastand North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld79777973939285999799100917592
70677261
53454248
1310813
19182215
18172113
10410411497
9695
80788770
77748763
70677066
67657061
63615169
878682909293 **93––––91 **8291 **
363032296563–66718290613165
302428205848–68768192492555
353126365457 **5564 **7082–53 **2953 **
332824325150 **4666 **7578–48 **2549 **
10885
878672999799100856687
9067597498124106703478
222083034367621429
23484750695581411346
22484750695480411346
101112–11011999102110106109
94109–1121159810210698105
90–––959496908191
85–––959397887889
8386 **8396 **9392–81 **6881 **
7883 **7996 **9392–79 **6679 **
90––79 **8896–73 **6176 **
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
youth literacy rate– Number of literate persons aged 15–24 years, expressed as a percentage of the total populationin that group.Pre-primary school gross enrolment ratio– Number of children enrolled in pre-primary school, regardless of age,expressed as a percentage of the total number of children of official pre-primary school age.Primary school gross enrolment ratio– Number of children enrolled in primary school, regardless of age,expressed as a percentage of the total number of children of official primary school age.Primary school net enrolment ratio– Number of children enrolled in primary or secondary school who are of officialprimary school age, expressed as a percentage of the total number of children of official primary school age. Becauseof the inclusion of primary-school-aged children enrolled in secondary school, this indicator can also be referred to as aprimary adjusted net enrolment ratio.Primary school net attendance ratio– Number of children attending primary or secondary school who are of officialprimary school age, expressed as a percentage of the total number of children of official primary school age. Becauseof the inclusion of primary-school-aged children attending secondary school, this indicator can also be referred to as aprimary adjusted net attendance ratio.Survival rate to last primary grade– Percentage of children entering the first grade of primary school whoeventually reach the last grade of primary school.Mobile phones– The number of active subscriptions to a public mobile telephone service, including the number ofprepaid SIM cards active during the past three months.Internet users– The estimated number of Internet users out of the total population. This includes those using theInternet from any device (including mobile phones) in the last 12 months.Secondary school net enrolment ratio– Number of children enrolled in secondary school who are of officialsecondary school age, expressed as a percentage of the total number of children of official secondary school age.Secondary net enrolment ratio does not include secondary-school-aged children enrolled in tertiary education owingto challenges in age reporting and recording at that level.
Secondary school net attendance ratio– Number of children attending secondary or tertiary school who are ofofficial secondary school age, expressed as a percentage of the total number of children of official secondary schoolage. Because of the inclusion of secondary-school-aged children attending tertiary school, this indicator can also bereferred to as a secondary adjusted net attendance ratio.All data refer to official International Standard Classifications of Education (ISCED) for the primary andsecondary education levels and thus may not directly correspond to a country-specific school system.
MAIN DATA SOURCES
youth literacy– UNESCO Institute for Statistics (UIS).Mobile phone and Internet use– International Telecommunications Union, Geneva.Pre-primary, primary and secondary enrolment– UIS. Estimates based on administrative data from nationalEducation Management Information Systems (EMIS) with United Nations population estimates.Primary and secondary school attendance– Demographic and Health Surveys (DHS), Multiple Indicator ClusterSurveys (MICS) and other national household surveys.Survival rate to last primary grade– Administrative data: UIS; survey data: DHS and MICS. Regional and globalaverages calculated by UNICEF.
NOTES
– Data not available.x Data refer to years or periods other than those specified in the column heading. Such data are not included in thecalculation of regional and global averages. Estimates from data years prior to 2000 are not displayed.y Data differ from the standard definition or refer to only part of a country. Such data are included in the calculationof regional and global averages.z Data provided by Chinese Ministry of Education. The UIS data do not currently publish net enrolment ratesforChina.* Data refer to the most recent year available during the period specified in the column heading.** Excludes China.
Statistical tables
107
TABLE 6: DEMOGRAPHIC INDICATORSPopulation(thousands)2010Countries and territoriesunder 18% ofAverage annualTotalgrowth rate ofCrude birthLife expectancy fertility populationurban population (%)rate urbanizedrateat birthunder 5 1970–1990 1990–2010 2010–2030α1970 1990 2010 1970 1990 2010 1970 1990 2010 201020101970–1990 1990–2010 2010–2030αPopulation annualgrowth rate (%)Crude deathrate
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republic of the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFijiFinlandFrance
16,78189511,6891510,1672812,1067745,1141,5342,4329629155,938601,7792,1761314,4532604,24069578559,4901241,2558,5763,7615,5609,2616,9201932,0695,8464,669322,16315,9393561,89581,4149,4078122,4032451,843
5,5462083,44743,37883,3862261,458386795269314,70715515616371,506711,23516522515,156373732,9551,1851,4923,0551,885516512,0061,21981,5964,49812262323632,96921056964548
0.42.23.13.92.8-0.31.51.71.50.11.72.14.22.30.40.60.22.22.63.12.30.93.52.23.50.22.42.31.62.91.21.22.42.51.61.72.23.02.9-1.02.64.20.41.01.10.3
4.4-0.11.72.43.11.81.1-0.71.30.51.21.54.71.70.3-0.30.42.53.11.32.0-0.71.91.32.3-0.82.82.02.02.41.01.82.03.11.30.81.72.62.60.72.12.3-0.10.31.80.1
2.60.11.01.42.40.80.70.01.10.10.81.01.41.00.1-0.40.21.72.51.11.5-0.40.80.61.3-0.72.81.61.01.90.80.91.82.50.70.21.02.32.10.41.02.1-0.3-0.10.80.1
29816–27–959137672397128262320713107923202019715232210991814–721107712
2266–23–8871176310811115171411977412171912147917176761112–413117712
1665–14–897975369141041277101363151214814851616675911–41212771010161010–655715812107109
523349–52–232320152926384722161542484746234635361648444245174143462936384743–33521529191635481549–4242414339471547341417
522532–53–222115112724293616141237473836153524291247464442143941472321273738–27411217191221501242–3029323247411448291313
441320–42–1715149201520201111112540202692415191043342236112135451412203835–16341010121114431229–2221232037361231221113
356753–37–667071706566644269717166404146665559677141444446735342446263614853–67446970737062447343–5858505740437143607072
427267–41–726877756569725975717672495359676466737149465653776549517469685656–76537274777271477551–6869626647486947667577
487773–51–767482817175756977708076566766765373787355506351817448497973736157–79557679797869487958–7375737251617559698081
6.31.52.3–5.4–2.21.71.91.42.21.92.52.21.61.41.82.85.32.43.31.12.81.82.01.55.94.32.64.51.72.44.66.01.91.62.44.94.5–1.84.41.51.51.51.52.05.81.93.8–2.62.52.72.35.24.51.74.22.71.92.0
2352668859309264896852848928447597524235674961877671261120588161392889477528627564515875707460358776676967436440226917528585
2.92.84.44.77.3-0.32.02.31.50.22.03.04.57.1-0.32.70.31.96.28.04.02.811.83.63.81.46.87.20.46.41.35.33.95.42.13.83.34.94.5-0.53.95.91.92.03.61.02.12.50.57.22.13.94.42.42.92.53.81.14.52.61.50.8
5.51.62.92.15.31.01.4-0.91.50.61.01.74.73.51.80.30.42.94.15.12.90.43.72.13.0-0.45.94.84.34.21.33.42.34.51.63.72.12.63.31.93.33.50.20.42.10.01.14.20.52.3-0.22.72.71.82.13.84.1-0.94.11.90.71.2
4.41.41.71.23.42.00.90.41.30.61.41.21.52.91.40.10.32.63.72.92.10.81.60.91.8-0.35.44.52.92.91.01.72.94.50.81.61.43.62.81.11.73.30.50.01.20.40.84.00.52.00.61.61.82.21.43.44.70.13.61.40.50.8
6,83935,0561,214379223,6705,22230,2642,4243192,51824840,3802991,08713,754
108
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED20121,70411,84832611361,0541,4709,0086171078617811,932902993,9741.72.90.26.20.02.32.72.31.81.32.70.72.61.70.40.60.93.00.42.3-0.21.61.71.80.73.12.5-0.82.70.80.40.50.42.40.31.80.11.01.11.40.72.32.3-0.21.80.50.20.47211020–1112161325211121810115191214–6698201613186109
Population(thousands)2010Countries and territoriesunder 18
% ofAverage annualTotalgrowth rate ofCrude birthLife expectancy fertility populationurban population (%)rate urbanizedrateat birthunder 5 1970–1990 1990–2010 2010–2030α1970 1990 2010 1970 1990 2010 1970 1990 2010 201020101970–1990 1990–2010 2010–2030αPopulation annualgrowth rate (%)Crude deathrate
GabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People's Democratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia (Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibiaNauruNepalNetherlandsNew Zealand
63918587728791525613,5223,46710,9773,5331,98358635106,9542,1674,9401,658726240303654,2601,237003,3209661,8194918124447,309 127,97977,787 21,57920,9946,14915,7325,1881,1143582,36373510,2752,90296124720,4715,4312,7308164,7251,64119,8176,66436108382811,9545952,6056833851151,2823229702741,9896812,257716726281661082910,3313,3057,8632,71510,2062,828106268,2662,91279192051,6055133518439,633 11,0954913729212971463910,8363,02211,8493,87614,9373,9569892864112,8743,5063,5539341,086312
2.83.70.70.12.70.70.12.51.62.60.02.10.93.00.01.12.32.23.22.80.92.30.31.20.83.61.23.72.55.12.02.20.60.92.32.03.91.50.80.62.73.62.63.21.81.04.22.81.22.42.21.32.70.82.41.82.03.01.72.40.70.9
2.42.9-1.10.22.50.60.42.42.72.00.21.7-2.62.2-0.21.11.71.31.53.01.22.50.30.70.23.0-0.22.71.61.41.02.0-0.81.81.43.21.91.1-0.51.43.02.32.21.82.90.60.72.81.01.50.70.71.10.21.32.71.02.40.62.30.51.3
1.82.4-0.7-0.22.00.10.12.32.32.00.31.1-0.11.7-0.21.01.10.80.72.80.91.40.00.2-0.31.50.82.41.41.91.11.1-0.40.50.82.51.00.7-0.41.12.73.21.41.02.80.21.12.00.40.90.70.01.20.00.82.10.61.40.41.40.20.9
202691217891530261218–1511716151612117108711915–61118119172316–9122124721309–187109–15317251615–2189
11139111198921221013–7147118879610775910–381313710214–1110161859218–11657–105821119–1398
99111181065131769–5136875666107941011–37614716114–14861354158–10756–61061598–687
345119144717284449463739–471521384042452226173619512651–4931421433434949–1713485233504916–47294341–441047484043–441722
384717113910283946462537–381217312634381422102610362342–2131421426364626–1513454828414916–41222834–321130432738–391317
27381283210193239381827–2710152218173516219189252238–1824231115283923–101235442017469–34132025–231220381726–241115
473867714972645234375647–526974495251587172716872616252–6760467065494152–7170444164443470–47636162–566952395053–437471
615371755777696244436155–666978586262677576777179706759–7266546969594268–7175514770614475–56697166–617664435761–547775
625874806480767154487062–737482656973688081827383736757–7467677372485675–7280665474775179–58737769–687472506562–688181
3.34.91.61.44.21.52.24.05.25.12.33.3–3.11.42.12.62.11.74.72.12.91.42.31.43.12.64.7–2.32.72.71.51.83.25.22.6–1.51.64.76.02.61.86.31.3–4.51.62.33.5–2.51.72.34.92.03.2–2.71.82.2
8658537451613949353029521005268933044716662926852677959224498353368872748781467853020724036957241427823100626158383438100198386
6.77.11.40.13.81.30.33.24.45.70.13.90.94.70.51.43.65.14.83.81.42.60.52.11.74.91.76.54.35.82.04.61.32.64.74.26.01.12.41.05.36.94.57.14.21.05.27.81.53.42.41.13.93.74.18.32.44.11.76.41.21.2
3.55.0-1.30.24.20.81.23.33.92.30.04.70.13.40.01.32.53.22.62.71.62.60.41.00.53.40.03.72.81.40.55.8-1.02.04.73.92.10.3-0.61.74.35.04.14.05.00.92.03.00.81.90.10.61.61.42.25.72.54.00.66.01.51.3
2.03.4-0.20.13.20.71.53.33.93.31.62.7-0.12.70.31.12.51.71.33.01.51.50.50.70.21.81.54.42.21.91.93.5-0.20.73.13.41.31.8-0.11.44.25.72.03.04.60.31.83.11.01.22.20.41.90.31.73.82.43.00.44.10.51.0
EM28BAFebr RGua Ory ED2012
Statistical tables
109
TABLE 6: DEMOGRAPHIC INDICATORSPopulation(thousands)2010Countries and territoriesunder 18% ofAverage annualTotalgrowth rate ofCrude birthLife expectancy fertility populationurban population (%)rate urbanizedrateat birthunder 5 1970–1990 1990–2010 2010–2030α1970 1990 2010 1970 1990 2010 1970 1990 2010 201020101970–1990 1990–2010 2010–2030αPopulation annualgrowth rate (%)Crude deathrate
NicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent and the GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and TobagoTunisiaTurkeyTurkmenistanTuvaluUgandaUkraineUnited Arab Emirates
2,3978,61177,90711,1142,02190873,22771,2053,1122,57310,44738,9707,0961,94627010,0037593,93325,9765,170175535826789,8256,2822,113432,9021,1111,0413422484,77218,086–8,1896,154–1765481,9241,4448,9183,05017,325
6783,08526,569030362028221,41823459627402,90911,2541,933517912,3722151,0798,1171,8315159222233,1452,0815651497023127699801,6675,041–2,5211,893–481575573762,4948714,361
2.72.92.7-3.90.43.14.73.21.42.42.72.72.52.80.80.77.41.61.00.70.63.2-0.51.40.90.61.22.35.12.80.81.62.11.90.80.73.33.02.5–0.71.6–0.43.30.30.43.32.92.2
1.73.42.4-2.30.73.32.02.21.51.92.52.11.52.10.00.46.60.6-1.0-0.4-0.22.01.31.20.10.61.31.82.72.70.11.01.92.60.20.32.81.71.5–0.80.9–1.31.60.50.72.51.31.0
1.13.42.4-1.60.72.61.31.50.91.22.01.51.01.5-0.1-0.21.50.2-0.6-0.3-0.22.50.90.70.10.50.41.71.72.4-0.20.31.90.80.10.12.22.80.4–0.40.5–0.71.00.50.31.61.40.3
142622–10131615–817714981169109920–91110–1315249–295910132414–99–9181091110108232077141611–1697
72419–115510–51067710102610111232–677–1051310–255101011208–97–7101195858181467688–17133
51314–9447–5855610102513121412–675–84912–16510961515–97–714108467981168658–12171
465646–17504943–37443742391721363218211451–394039–41475118–47231817455138–2031–374914164740382442493627393937–491537
375644–14453840–26353330331511241619141445–282532–38364415–44191511404529–1020–234314123639191743423121272635–501326
244940–12331827–2030242025119131012101241–181725–31223711–3991010324421–1118–182912102328121138322715171822–451113
543842–74565153–65466553617067666165686944–646155–55524168–35687069544053–7263–634874736060606640456565545058–507162
644146–77687161–72566866657174747268696833–716965–61695372–39767173574562–7770–675978787163737146537069696363–477072
745451–81737365–76627274687679788169746955–747272–64745974–47817579675152–8175–704881827667747562577270747465–546876
2.67.15.5–1.94.52.33.4–2.54.03.02.53.11.41.32.31.31.51.41.55.4–2.02.13.9–3.72.84.81.6–5.01.31.31.44.26.32.5–1.52.3–2.33.41.91.52.93.31.61.46.24.13.91.62.02.12.4–6.11.41.7
5717503879747336837513617749616196834757731932284920946282425655381005550193762–7714–69218574562634592843231467705050136984
3.25.74.9-2.00.94.28.74.22.23.04.84.03.44.71.61.77.64.52.92.11.45.8-0.42.42.40.83.24.27.44.12.02.73.91.92.42.35.44.42.9–1.40.8–1.87.60.41.63.92.23.92.03.44.51.2-0.53.84.32.34.05.71.410.4
2.24.04.1-1.41.23.82.53.02.53.51.63.32.02.10.01.56.81.2-1.00.0-0.28.20.90.91.00.41.53.53.03.10.71.42.72.60.00.24.32.92.4–1.0-0.4–2.01.20.60.73.20.41.70.53.64.30.62.92.02.32.11.64.1-0.57.4
1.85.03.7-0.11.02.91.72.71.41.83.82.31.42.40.30.61.50.50.70.60.04.52.22.01.11.30.32.61.93.40.51.43.10.80.50.64.54.21.2–0.72.1–1.22.10.70.52.42.41.80.54.63.22.02.71.31.42.01.45.1-0.11.9
4536032,796463363,01223,1091,804418,4718,0231,515
110
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED201211219386314958686,41350616,4652,3764211.01.02.80.61.12.42.12.61.13.10.410.30.42.12.50.40.51.21.51.60.43.2-0.67.10.02.91.80.70.00.80.91.00.52.9-0.61.7
Population(thousands)2010Countries and territoriesunder 18
% ofAverage annualTotalgrowth rate ofCrude birthLife expectancy fertility populationurban population (%)rate urbanizedrateat birthunder 5 1970–1990 1990–2010 2010–2030α1970 1990 2010 1970 1990 2010 1970 1990 2010 201020101970–1990 1990–2010 2010–2030αPopulation annualgrowth rate (%)Crude deathrate
United KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela (Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
13,07622,96475,2019199,94010710,17025,98112,4016,9375,86620,281
3,7668,01021,6502462,738332,9267,1864,0572,4121,6926,391
0.13.11.00.52.72.73.12.03.33.23.52.9
0.42.81.00.41.52.51.91.33.52.50.92.5
0.63.00.80.31.02.21.20.72.73.11.72.1
1218910101471824171319
111591078581217914
910897555616139
154816213642374151494846
144416183536293052443741
124114152130211738462933
724771696352644840495545
765175736763716656476153
805778776871747565495061
1.95.52.12.12.43.92.51.85.26.33.34.4
802682923626933032363840
0.27.51.10.93.14.83.92.55.64.56.15.3
0.54.51.50.60.94.02.43.45.62.12.34.5
0.84.91.00.41.84.21.42.64.54.33.13.7
MEMORANDUMSudan and South Sudanδ
SUMMARY INDICATORS#AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld477,383419,324192,994205,670156,4441,151,806612,649539,157195,71395,544203,0081,953,940389,2582,201,180155,135138,07562,19869,37247,524316,151175,146141,00453,46128,01557,212563,545122,520633,9332.72.82.82.73.02.02.31.82.21.00.72.22.51.82.42.52.52.62.11.31.81.01.40.20.61.52.41.32.12.32.22.41.50.81.20.40.90.20.41.12.10.92020192216131710101010132212151615188911771199159111312145787611981084647474744384036372017394733414443453427332327181329432635373540241823141914122134204644474252564961606671554359525051486364596868687663516557545553716965727470806859704.54.94.65.42.82.22.71.82.21.81.72.64.22.540373044593930467964774529504.34.64.64.64.33.93.83.93.21.91.03.84.82.63.53.93.64.12.83.02.73.22.10.30.92.94.12.23.33.63.53.72.12.02.61.71.20.60.72.13.81.7
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Crude death rate– Annual number of deaths per 1,000 population.Crude birth rate– Annual number of births per 1,000 population.Life expectancy at birth– Number of years newborn children would live if subject to the mortality risksprevailing for the cross section of population at the time of their birth.Total fertility rate– Number of children who would be born per woman if she lived to the end of herchildbearing years and bore children at each age in accordance with prevailing age-specific fertility rates.% of population urbanized– Percentage of population living in urban areas as defined according to thenational definition used in the most recent population census.
EM28BAFebr RGua Ory ED2012MAIN DATA SOURCESNOTES– Data not available.αBased on medium-fertility variant projections.
Child population– United Nations Population Division.Crude death and birth rates– United Nations Population Division.Life expectancy– United Nations Population Division.Total fertility rate– United Nations Population Division.Urban population– United Nations Population Division. Growth rates calculated by UNICEF based on datafrom United Nations Population Division.
Statistical tables
111
TABLE 7: ECONOMIC INDICATORSgNI per capita (US$)US$Countries and territories2010PPP US$2010gDP per capitaaverage annualgrowth rate (%)1970–1990 1990–2010Average% of populationannual rate below internationalof inflationpoverty line of(%)US$1.25 per day1990–20102000–2009*% of central governmentexpenditure (2000–2009*)allocated to:health education defenceODA ODA inflowinflow in as a % ofmillions recipientUS$gNI20092009Debt serviceas a % ofexports of goodsand services19902009
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republic of the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFijiFinland
330 x4,0004,46041,130 x3,96010,6108,4503,09043,740 x46,7105,180d25,420 x640d6,03045,4203,7407501,9201,7904,7906,8909,39031,180 x6,2405501607601,16041,950 x3,1604606009,9404,2605,5108202,310–6,5801,07013,7605,550 x30,460 x17,870a18058,9801,280 x4,9604,8604,5102,3403,36014,68034014,3603803,61047,170
970 x, e8,8408,130 e–5,43015,380 e15,1505,45038,510 x39,4109,220–33,530 x1,620–14,02037,8405,970 e1,5105,0704,5608,97013,91010,92048,760 x13,2101,2603902,0402,19037,280 x3,6707601,18013,8907,5709,0001,1803,280–10,880 e1,65018,710–30,160 x23,620
–-0.7 x1.6––8.3 x-0.7–1.52.4–1.9-1.3 x0.41.7–2.22.90.3–-1.1–8.22.3-2.2 x3.4 x1.41.1–3.42.0–-1.3-1.01.56.61.90.1 x3.1–0.7-1.9–3.95.9 x–
–5.41.5–4.21.72.16.12.3 x1.85.51.02.8 x3.50.8 x4.51.61.91.25.31.58.9 x3.51.5-0.4 x3.32.4-1.66.3 x0.61.94.2-0.72.93.49.21.5-0.40.7–2.6-1.02.92.6 x2.1 x2.5
–14123x22728513x25333x43x122215775x9545x403124x42336651448–125264x4x6
–17x–54–11––1––50–0–12 x472614031 x4–157812810–216362116164654–1240––0x
–4x4x–––5–14161x1696–3168x–89–5x6x–107x2x–3x9–––1509x–4–20–16–6x17––0––10–416––1619x3x
–2x24 x–––5–1094x201614–4320 x–1324–26 x6x–517 x15 x–12 x2–––17220 x–4–24–9–12 x9
–4x17 x–––3–6212 x3138–335x––6–8x3x–514 x23 x–10 x6–––51013 x–10–––4–4x4––3––4–63––5176x4x
6,070358319–2396128528––232––1,2271298–28683125726415280338––1,084549722649–196237561801,1321,0605128381092,366169116––672,354–1623612020992527732145–3,82071–
–30–0106––1––1–0––1094220––144173–1312900095–0110––––23–141000010––132–
––62–7–30––––––17–––57–31–419–19641–18–582201039231–2126––––––––47271814–––339–
–5––8–1718––1––3–4–123x–97123–185x817–4––22320–2x–98–––––––610935514–––32–
112
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012–31040,1402,460 x8,580 e8,700 e9,2705,9106,390 e23,810540 e19,5001,0104,49037,180–-2.32.0–4.7 x2.11.34.1-1.9––1.5 x–0.72.9–-3.11.5-1.4 x1.73.91.72.72.619.2-1.5 x5.02.91.22.6–23423x2115741214 x19742–59–19–4525––039––––10––13–1118––7518 x10 x
gNI per capita (US$)US$Countries and territories2010PPP US$2010
gDP per capitaaverage annualgrowth rate (%)1970–1990 1990–2010
Average% of populationannual rate below internationalof inflationpoverty line of(%)US$1.25 per day1990–20102000–2009*
% of central governmentexpenditure (2000–2009*)allocated to:health education defence
ODA ODA inflowinflow in as a % ofmillions recipientUS$gNI20092009
Debt serviceas a % ofexports of goodsand services19902009
FranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People's Democratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia (Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibiaNauruNepal
42,3907,7604402,70043,3301,24027,2405,5602,7403805403,270650–1,88012,99033,8701,3402,5804,530 x2,32040,99027,34035,0904,75042,1504,3507,4407802,010d8801,01011,6209,0201,08019012,020 x136,540 x11,40079,5104403307,9004,27060018,350 x2,9901,0607,7409,3302,700197,460 x1,8906,6902,850440a4,650–490
34,44013,1901,2704,98038,1701,60027,3607,560 e4,610 e9801,0803,530 e1,110–3,730 e19,28028,6303,5604,30011,420 x3,32032,74027,80031,0907,430 e34,7905,77010,6101,6103,510 e–2,1802,30016,36014,1701,91033016,330 x, e–17,88063,85098085014,3605,4801,02023,070 x–2,00013,67015,0103,420 e–3,70012,7104,560920–6,580–1,200
2.20.20.7–2.3-2.01.34.2 x0.2–0.1-1.6––0.83.03.22.14.7-2.3–2.81.92.8-1.33.42.5 x–1.2-5.3-6.8 x––3.4–2.5-4.2–2.2–2.7-2.3-0.14.0–0.26.5–-1.03.2 x1.6–1.6––1.9-1.0 x1.4-2.1 x–1.0
1.3-0.90.12.71.32.42.62.91.31.2-1.72.5-1.1 x–1.62.92.24.92.62.7 x-2.2 x4.71.80.90.70.82.53.90.31.22.0 x0.54.34.52.42.21.72.9 x3.0 x3.52.9-0.21.03.24.9 x2.72.6 x-1.10.93.51.50.32.2 x3.13.7 x2.44.38.2 x2.1–1.9
268741265379181115 x–1311561522 x13 x35315-14581035x372218783618 x1x223132643x53x4861321x257x31724 x10–7
–53415–30––1743498x55–230–421924–––0–0020––2340–4384––0–68740251––21–331–220360–49 x–55
–––5207x7x10 x–––––––1121217–16 x131462x1067x–512–102x9–––11136–6x8–13––95––6–3x–3––7
–––7122 x11 x17 x–––––––89348–14 x1611176x16726 x–811–127x18–––61015–23 x19–13––1625––9–18 x–13––18
–––1745x8x––––––––3013710–3x16424x1966x–67–311 x4–––315–11 x6–2–––3––9–13 x–23––9
–78128908–1,583–483762151461731,120–457––2,3931,049932,791–––150–7612981,77827–315420–64112350539–––44577214433985–59287156185121–372759122,01335732624855
–1199–10–81–––––3––0005–––1–30615–77–26780––––170311–3292045–92121–3–7
–417––21–2121821–5–30––25311––––20–18–26–––8––4–––––32231248––24616––––182117––12
––76–3–812103x2x2–5––517–––––24–4794––916–14211––29–––572x–––315––4–101–––4
EM28BAFebr RGua Ory ED2012
Statistical tables
113
TABLE 7: ECONOMIC INDICATORSgNI per capita (US$)US$Countries and territories2010PPP US$2010gDP per capitaaverage annualgrowth rate (%)1970–1990 1990–2010Average% of populationannual rate below internationalof inflationpoverty line of(%)US$1.25 per day1990–20102000–2009*% of central governmentexpenditure (2000–2009*)allocated to:health education defenceODA ODA inflowinflow in as a % ofmillions recipientUS$gNI20092009Debt serviceas a % ofexports of goodsand services19902009
NetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent and the GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and TobagoTunisiaTurkeyTurkmenistanTuvalu
49,72029,050 x1,0803601,180–85,380b17,890 x1,0506,4606,9901,3002,9404,7102,05012,42021,860d19,8901,8107,8409,9105409,9804,9704,8502,93050,670 x1,20017,200 x1,0505,8209,49034040,92016,22023,8601,030a6,100–31,6502,290–5,920 x2,60049,93070,3502,6407804,2104,5202,2204403,38015,3804,0709,5003,700–
42,59028,050 x2,610 e7002,160–57,130–24,410 x2,78010,760 e12,940 e2,390 e5,4308,9403,93019,02024,710–29,0103,34014,05019,1901,18013,170 e8,520 e8,260 e4,300 e–1,91023,900 x1,85011,23020,470 e83054,70023,14026,9702,210 e–10,280–31,5505,070–7,610 x, e4,89039,60049,1804,8702,0608,24010,8303,570 e7904,630 e24,000 e8,14014,5807,160 e–
1.60.8-3.7-2.1-1.4–3.2–3.33.0–0.3-0.73.1-0.60.6–2.6–6.2–0.9 x–1.26.3 x5.3 x3.3–––-1.4-0.7–2.9-0.55.6–––-0.80.1–1.93.0–-2.2 x3.01.81.22.0–4.7––-0.6–0.52.52.0––
2.01.91.9-0.21.9–2.1-2.4 x2.0 x1.7-0.2 x3.2-0.20.13.02.04.41.6–4.2-0.62.82.12.32.21.03.63.0––0.4 x1.11.51.81.13.93.73.3-1.0–1.3–2.14.1–1.5 x1.62.20.91.6-0.12.9
2218420–44x4x103x2810107114–44147561032263x–4x424 x51717127–8–410–48 x8217783
––164364––––23–1036 x56230–––21077–21 x–––29–340053–0x0––17––7–16 x63––22211
141713 x–––15–71–187x7x1321315–115127–––12–18––3169–82015––––16––8402x214––––653––
111716 x–––5–152–1622 x22 x7191114–15763–––16–9––14108–18412––––010––20639x420––––131910––
336x–––5–3313––4x11 x–533–111512––––––––763–2433––––318––85524 x98––––348––
––7744701,6599–3,0262122,7813566414148442310––––245––9346413177–31–1,01860823437–––2066621,075––704–15758––245409-771932174994074741,3624018
EM28BAFebr RGua Ory ED20121.0-0.5 x0.01.65.03.52.35.1–245x46544695–03739–4x3325 x–
––1391––––21805100––––4––1915616–16–81423–––43–0–2–2––0802–18120100–
––21222––––16–33712623–––––0–93235–28–14–78–––1025 x–––10––5––20–14––82–2227––
––132x1––––10–51251114––––1128184188133–15–3x2862–––4–4––10––2––3x15712–13 x4x–940––
114
THE STATE OF THE WORLD’S CHILDREN 2012
gNI per capita (US$)US$Countries and territories2010PPP US$2010
gDP per capitaaverage annualgrowth rate (%)1970–1990 1990–2010
Average% of populationannual rate below internationalof inflationpoverty line of(%)US$1.25 per day1990–20102000–2009*
% of central governmentexpenditure (2000–2009*)allocated to:health education defence
ODA ODA inflowinflow in as a % ofmillions recipientUS$gNI20092009
Debt serviceas a % ofexports of goodsand services19902009
UgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela (Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
4903,010d38,54053047,14010,5901,2802,76011,5901,1001,060 x1,0704601,270
1,2306,580–36,5801,42047,02013,8903,090 e4,450 e11,9502,9102,320 x1,370–2,020
––-4.9 x2.0–2.10.9–1.1 x-1.6––-2.3-0.40.1
3.60.40.5 x2.12.41.82.02.26.80.36.01.5 x0.6-3.23.6
8726x31421683-3331017 x29028
290––68–046–4131864––
–37x15 x–247––844x13 x8x1x
–617 x4x–38––211422 x14 x24 x8x
–330 x7x–194––5–19 x4x7x28 x
1,786668––2,934–51190103673,7445001,2697372,289
121––14–011604211–5
47–––25–31–222–413194
134––3–20–1x6233–6
MEMORANDUMSudan and South Sudanδ
SUMMARY INDICATORS#
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
gNI per capita– Gross national income (GNI) is the sum of value added by all resident producers plus anyproduct taxes (less subsidies) not included in the valuation of output plus net receipts of primary income(compensation of employees and property income) from abroad. GNI per capita is gross national incomedivided by midyear population. GNI per capita in US dollars is converted using the World Bank Atlas method.gNI per capita (PPP US$)– GNI per capita converted to international dollars taking into accountdifferences in price levels (purchasing power) between countries. Based on data from the InternationalComparison Program (ICP).gDP per capita– Gross domestic product (GDP) is the sum of value added by all resident producers plusany product taxes (less subsidies) not included in the valuation of output. GDP per capita is gross domesticproduct divided by midyear population. Growth is calculated from constant price GDP data in local currency.% of population below international poverty line of US$1.25 per day– Percentage of the populationliving on less than US$1.25 per day at 2005 prices, adjusted for purchasing power parity. The new povertythreshold reflects revisions to purchasing power parity (PPP) exchange rates based on the results of the2005 ICP. The revisions reveal that the cost of living is higher across the developing world than previouslyestimated. As a result of these revisions, poverty rates for individual countries cannot be compared withpoverty rates reported in previous editions. More detailed information on the definition, methodology andsources of the data presented is available at <www.worldbank.org>.ODA– Net official development assistance.Debt service– Sum of interest payments and repayments of principal on external public and publiclyguaranteed long-term debts.
EM28BAFebr RGua Ory ED2012MAIN DATA SOURCESa:b:c:d:–x
AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld
1,4831,1921,4869052,7522,9131,2414,2867,8597,26340,8453,3046698,796
2,8092,1452,7501,6045,2325,5783,2717,47211,13313,28838,0095,8051,37410,740
0.90.00.3-0.5-0.24.52.15.61.4–2.42.5-0.22.4
2.12.01.91.82.46.94.57.41.62.31.64.83.22.6
2431382296753055216528
42494552327401664–265025
–––––121–6193–15
–––––536–648–5
–––––111310–91210–11
41,77939,11020,17516,48413,38823,85714,1879,6697,5447,113–85,72939,90788,559
3434201000–080
18181222–17211620––191218
5452–55516––959
gNI per capita– The World Bank.gDP per capita– The World Bank.Rate of inflation– The World Bank.% of population below international poverty line of US$1.25 per day– The World Bank.Expenditure on health, education and defence– International Monetary Fund.ODA– Organisation for Economic Co-operation and Development.Debt service– The World Bank.
low-income country (GNI per capita is US$1,005 or less).lower-middle-income country (GNI per capita is US$1,006 to US$3,975).upper-middle-income country (GNI per capita is US$3,976 to US$12,275).high-income country (GNI per capita is US$12,276 or more).Data not available.Data refer to years or periods other than those specified in the column heading. Such data arenotincluded in the calculation of regional and global averages.e Estimate is based on regression; other PPP figures are extrapolated from the 2005 ICPbenchmarkestimates.* Data refer to the most recent year available during the period specified in the column heading.
NOTES
Statistical tables
115
TABLE 8: WOMENLifeexpectancy:females asa % of males2010Delivery care coverage (%)Maternal mortality ratio†Survival rateEnrolment ratios:Antenatal careAdult literacy females as a % of males to last gradecoverage (%)2008Skilledof primary: Contraceptiverate:prevalence At least At least attendant Institutionalfemales as a Primary Secondary females asLifetime riska % of males(%)% of malesgERgERonce four times at birthdelivery C-section 2006–2010* 2008of maternal2005–2010* 2007–2010* 2007–2010* 2006–2009*2006–2010*2006–2010*2006–2010*reported adjusted death: 1 in:
Countries and territories
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republicof the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFijiFinland
101108104–106–11010910610710910910210210911810710410710610710797110106110104106104104106111107106108105111105104–106104110105106108110107106105–108108105114105108115106108109
–9779–70101100100––99–9884–100––54599197101100979959848380–8961521009410086––100709910098–10073–––100937794937210043––
679794101819499103100999910098104–10210097881019910297931011008997948610093717095104100929410799811009899100–851018999861019697968399919999
49101102108–1001141039696103103104112–10297108–99981021051111029674728283981185641103107110––113106–10499101101–561037310611310396102–7110377107105
94 x101100–97 x––100––100–102 x103–100–1029510598100––––105979999––9298 x––102121 x99––96–––––94–101–103–100––––107––
236961–6x–78 x5571 x–5145 x–53–73 x75 x34176661365381––1722512974 x61 x19558857926 x44 x44 x8013–78––69 x17–23–7373 x6073–8x–15 x35 x–
369789–8010099 x9998–77981005310099 x–9484978699949899–8599898210098 x6953–929775 x86 x1009085–10099–10086–921009984 x749486 x70 x–28 x100100 x
–67––––89 x71 x92–45––23––––617772–7391––18 x–27 x60 x9972 x–23––89–75 x–8645 x–100––9445–7x–9558 x6678–41 x–12 x––
249995–4710098100––88999727100100–9574657110095971001005460716310078 x4423100999862 x83 x989957100100–10010074–931009898 x799665 x28 x1006x99–
13 x9795–46–999999–78––23–100 x–887863681009498100100516054619978 x56161009695–82 x–9954–100100–9574–87–98857285–26 x–5x–100
–19–––––1831245––12–2218–41219––50–291x–2x2x2611 x–2–2734–3x–21 y6x–––201372112–4226 x2825–3x–1–16
1,600 x21––––5527––24––190–1–57400260 x310320075–5310620 x460670 x–545401,100 x173276380 x780 x–21540 x1443–277550–550 x–160615559––7670 x34 x–
1,40031120–610–7029853849193406415594410200180919058211356097029060012948501,200263885340580–4447014531082506705300–1001408211028028012470268
111,700340–29–6001,9007,40014,3001,2001,0002,2001101,1005,10010,900330431701509,3001808602,0005,8002825110355,60035027142,0001,5004607139–1,100445,2001,4006,6008,5002302410,90093–32027038035073725,300401,3007,600
116
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
Countries and territories
Lifeexpectancy:females asa % of males2010
Delivery care coverage (%)Maternal mortality ratio†Survival rateEnrolment ratios:Antenatal careAdult literacy females as a % of males to last gradecoverage (%)2008Skilledof primary: Contraceptiverate:prevalence At least At least attendant Institutionalfemales as a Primary Secondary females asLifetime riska % of males(%)% of malesgERgERonce four times at birthdelivery C-section 2006–2010* 2008of maternal2005–2010* 2007–2010* 2007–2010* 2006–2009* 2006–2010*2006–2010*2006–2010*reported adjusted death: 1 in:
FranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People'sDemocratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia (Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibiaNauruNepalNetherlands
10411510697104107–117107105100106103104106–106109107102–112107107104105102–102105
EM28BAFebr RGua Ory ED201277100921158686–100–91839510052103–789497––101–64599499–65–91979810090–10298101981039995841019910810098101–999892909898106–9981102111138––871001039488107–659810589102106––1071018679102117120–98105–104 x109 x–––––10688–101101––94––––99102–88100 x101–99–38 x–58 x4711––––4041–358–45976 x73––553963 x1641553648693592 x96 x927993–100 x–869279 x9970100 x8175–9680–1009768 x9280959544––––7066––––4957 x–8535–7716 x–86––––31 x53 x73704029–2010098 x6246100–100100 x4454999549–866198 x9592–10010063 x5564819719–17––5937–––100 x355498 x9545100854898 x80––9810061 x5823819918100
109103104110106103106104111106107110104–107111104105105105111106106107107109104118104–102113
–9262100–8398–875557–84–100100–68939081––99112–9310092–9799
99–10410010099100949486–99––10099100–97998410110199971001011009810498100
101–96–9589951019359–101––1279910388999575106102991041001049890111103101
––98102–100–––9992100100––––99––97–––100––100100––99
71 x33 x18 x53–2476 x54549x144332–65––546179 x5089 x––69 x54 x59514622 x–48
100 x94 x9898100 x90–1009388939285–92––759398 x84100 x–99 x99–991009210010097
–63 x–90–78–––5070–54–81––518294 x–––68 x––94–47–––
–86 x57100–57–995146449226–67100–537997 x80100 x––98–99100446510099
–85 x5598–57––5239428925–67––474696 x65100–99 x97100 x9910043––97
216x–24297––162––3–1331179740 x2125–4015–19–6––––––74–––2923x–322–93x–43––17–5x2x–138314
–520 x730 x52–450––130980 x41086630––19–25023025 x84–––95 x–193749056 x–64410 x32–1,200990––9–50081029140 x460–74 x69022 x54––4713130500320 x450–280 x–
82604004873502–1106801,000270300–11013523024030753758965945530–981580202653099064–131744051031378308–5503685––6515110550240180–3809
6,600110491,30011,1006631,800–210261815093–2405,5009,4001401901,50030017,8005,10015,20045012,20051095038–4,500450493,6002,0006220540–5,8003,80045361,2001,200229,200–411,600500––7304,00036037180160–807,100
Statistical tables
117
TABLE 8: WOMENLifeexpectancy:females asa % of males2010Delivery care coverage (%)Maternal mortality ratio†Survival rateEnrolment ratios:Antenatal careAdult literacy females as a % of males to last gradecoverage (%)2008Skilledof primary: Contraceptiverate:prevalence At least At least attendant Institutionalfemales as a Primary Secondary females asLifetime riska % of males(%)% of malesgERgERonce four times at birthdelivery C-section 2006–2010* 2008of maternal2005–2010* 2007–2010* 2007–2010* 2006–2009* 2006–2010*2006–2010*2006–2010*reported adjusted death: 1 in:
Countries and territories
New ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent andthe GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and TobagoTunisiaTurkeyTurkmenistanTuvaluUganda
EM28BAFebr RGua Ory ED2012–100–909063971015794–100––96–9897–9898––861009693981011019610499102––9999975596–99100–9593991009696981041131041128679103105––1011008446105–104––1289099969987109–––98–96100–99––––97–––––109102––1001001014829–382412 x41–8–––351560 x–6668–4649––54378010093–989787 x98–87–97 x100 x742697––99–9097100 x–88899994848799969692999794–58–72–40 x––56–––65687––93––97––6449809981–829752 x99–42–100100703391 x––99–9082––96831001002960989895911009842–81–79–62 x99–25100 x––85989 x––98–8880––787399977363100998289100–781019594–969897––10198–53–10710889––841009999–102–95 x100–10314 x221523 x436073483124–5555––687483 x6747992267–9789 x90989341
105109102103–106105107103–10710710610711011210899109111110119105–107106109–104103104106–103106111109104106103–108109–11098105106104110110106103105108111106106114–102
–1003569––949058–998998891011009698–999910089––
101988088–100100988410397–971009899979998989910010110297
1041136077–98107967998108–1059910910010414796102999795108103
–126 x102100–––––––––98107 x––––100––106––
–72181523 x88 x502427215232797451–67–8068 x70 x805254–
–904658100–9999611009679969591–100 x100–98 x94 x–9810099
–781545–––862888–55919378––––89 x76 x–35––
–743339100–9999391008953828462100 x100 x100–1009910069100100
–741735––979934–8852858444––––9998 x–69––
232012–1615147–––3320102131–329x19 x–3x–––13–5–3x19–2–24–6–21 x–2624––12–3026–24–2–––21373x73
–67650550–––17250–60730130931602–––452117750 x–––29 x–160–400 x957 x860–1010–1,000400 x––39–180590––65 x8612 x4560–140––29 x12–440
14100820840–7–20260–7125095989467818322739540––––––244108–97096181001,200410–639–1004205104664489370350–55602377–430
3,8003001623–7,600–1,60093–5209431037032013,3009,8004,4004,7002,0002,7001,90035––––––1,300467,500–2110,00013,3004,10023014100–11,4001,100–4007511,4007,6006104301,2007,3004467–1,1008601,900500–35
118
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
Lifeexpectancy:females asa % of males2010
Delivery care coverage (%)Maternal mortality ratio†Survival rateEnrolment ratios:Antenatal careAdult literacy females as a % of males to last gradecoverage (%)2008Skilledof primary: Contraceptiverate:prevalence At least At least attendant Institutionalfemales as a Primary Secondary females asLifetime riska % of males(%)% of malesgERgERonce four times at birthdelivery C-section 2006–2010* 2008of maternal2005–2010* 2007–2010* 2007–2010* 2006–2009* 2006–2010*2006–2010*2006–2010*reported adjusted death: 1 in:
UkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela(Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
11810210510310711011010610810510510297106
100102–85–10199961009556769476
1009910010010197989597–8099–90
981011027810111399109109––––88
100––100 x––100105107 x99959610798
67–84347978 x6538–802841598
99100–88–96998494 x9147949064
75––43–90–––29 x14 x6057–
99100–49–1001007495 x8836476649
99100–50––978095 x6424486519
10–2653134–––10 x9x355
160–4501334211505769370 x5907301,100
261012790242730–6856210470790750
3,0004,2004,700232,1001,7001,400–54085091384232
MEMORANDUMSudan and South Sudanδ
SUMMARY INDICATORS#
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Life expectancy– Number of years newborn children would live if subject to the mortality risks prevailingfor the cross section of population at the time of their birth.Adult literacy rate– The number of persons aged 15 years and over who can both read and write withunderstanding a short, simple statement about everyday life, expressed as a percentage of the totalpopulation in that age group.Primary gross enrolment ratio (gER)– Total enrolment in primary school, regardless of age, expressedas a percentage of the official primary-school-aged population.Secondary gross enrolment ratio (gER)– Total enrolment in secondary school, regardless of age,expressed as a percentage of the official secondary-school-aged population.Survival rate to last primary grade– Percentage of children entering the first grade of primary schoolwho eventually reach the last grade (survey data).Contraceptive prevalence– Percentage of women (aged 15–49) in union currently using contraception.Antenatal care coverage– Percentage of women (aged 15–49) attended at least once during pregnancyby skilled health personnel (doctors, nurses or midwives) and the percentage attended by any provider atleastfour times.Skilled attendant at birth– Percentage of births attended by skilled heath personnel(doctors, nurses ormidwives).Institutional delivery– Percentage of women (aged 15–49) who gave birth during the two years precedingthe survey and delivered in a health facility.Caesarean section (C-section)– Percentage of births delivered by Caesarean section. (C-section ratesbetween 5 per cent and 15 per cent expected with adequate levels of emergency obstetric care.)Maternal mortality ratio– Number of deaths of women from pregnancy-related causes per 100,000livebirths during the same time period. The ‘reported’ column shows country-reported figures that are not adjustedfor under-reporting and misclassification. Maternal mortality ratio values have been rounded according to thefollowing scheme: <100, no rounding; 100–999, rounded to nearest 10; and >1,000, rounded to nearest 100.Lifetime risk of maternal death– Lifetime risk of maternal death takes into account both the probability ofbecoming pregnant and the probability of dying as a result of that pregnancy, accumulated across a woman’sreproductive years.
† The maternal mortality data in the column headed ‘reported’ refer to data reported by national authorities. The data in the column headed ‘adjusted’ refer to the 2008 United Nations inter-agency maternal mortality estimates that werereleased in late 2010. Periodically, the United Nations Inter-agency Group (WHO, UNICEF, UNFPA and the World Bank) produces internationally comparable sets of maternal mortality data that account for the well-documented problems ofunder-reporting and misclassification of maternal deaths, including also estimates for countries with no data. Please note that owing to an evolving methodology, these values are not comparable with previously reported maternal mortalityratio ‘adjusted’ values. Comparable time series on maternal mortality ratios for the years 1990, 1995, 2000, 2005 and 2008 are available at <www.childinfo.org>.
EM28BAFebr RGua Ory ED2012MAIN DATA SOURCESNOTES
AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld
104104104104105105104105109113107105104106
76768170818668949898100867590
929295879398–1019799100969396
8479887092978810510896100968297
99991019999100 **100––––99 **10099 **
30233616456651787469–613363
78788971777970929695–807381
49475145–52 **4679 **87––56 **4056 **
53504950756648909097–664667
48464847585943798793–594160
5333191492238–2814515
––––––––––––––
59064055072017020029088853414290590260
363138261902101106004801,7004,30012037140
Life expectancy– United Nations Population Division.Adult literacy– UNESCO Institute for Statistics (UIS).Primary and secondary school enrolment– UIS.Survival rate to last primary grade– Multiple Indicator Cluster Surveys (MICS) and DemographicandHealth Surveys (DHS).Contraceptive prevalence– MICS, DHS and other nationally representative sources;United Nations Population Division.Antenatal care coverage– MICS, DHS and other nationally representative sources.Skilled attendant at birth– MICS, DHS and other nationally representative sources.Institutional delivery– MICS, DHS and other nationally representative sources.C-section– DHS and other nationally representative sources.Maternal mortality ratio (reported)– Nationally representative sources, including household surveysand vital registration.Maternal mortality ratio (adjusted)– World Health Organization (WHO), UNICEF, United NationsPopulation Fund (UNFPA) and the World Bank.Lifetime risk of maternal death– WHO, UNICEF, UNFPA and the World Bank.
– Data not available.x Data refer to years or periods other than those specified in the column heading. Such data are notincluded in the calculation of regional and global averages. Estimates from data years prior to 2000 arenotdisplayed.y Data differ from the standard definition or refer to only part of a country. Such data are included in thecalculation of regional and global averages.* Data refer to the most recent year available during the period specified in the column heading.** Excludes China.
Statistical tables
119
TABLE 9: CHILD PROTECTIONChild labourChild marriage2000–2010*2000–2010*total male female married by 15 married by 18Female genital mutilation/cuttingBirth1997–2010*registration2000–2010*prevalenceattitudestotalwomenadaughtersbsupport for the practicecJustificationof wife beating2002–2010*malefemaleViolent discipline++2005–2010*total male female
Countries and territories
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republicof the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFijiFinland
13 y125y–24–7y4y––7y–513–5–40461826 y59y3y––38193931–3y47483–9y2725–535–––––42–8–10875y28––53––
17 y146y–22–8y–––8y–618–6–39471828 y711 y4y––39193931–4y44443–12 y2624–636–––––36–8–12787y28––59––
9y94y–25–5y–––5y–38–4–42451924 y47y2y––36193830–3y49522–6y2825–334–––––
–00––––0––1––32–0––8630–11––53311–32135––6–7––8–––––
39102––––10––12––66–7––3426226–36––48182336–186172––23–33––35–––––
69999–29–91 y96––94––10–––9460100741007291 y––64606670–9149999–978381 y––55–100 y––
––––––––––––––––––13–––––––73––1––2644–––––––36–––––
––––––––––––––––––2–––––––25––1––7––––––––9–––––
––––––––––––––––––1–––––––11––7––1438–––––––20–––––
–36–––––31––58––36––––14––––––––––––16 y–––––––––––––––––––8––––––52 y––
–3068––––22––49––36–––124768165––––71–5556–17––––––76––65–––––76–––4–39 y––71–81––
–7588–––––––75––––84–71–––38––––83––93––8984–––––––91–––––92–72–83–92 y–––––72 y–
–7889–––––––79––––87–71–––40––––84––93––9085–––––––91–––––92–73–85–––––––––
–7187–––––––71––––80–71–––36––––82––93––8784–––––––91–––––91–71–82–––––––––
120
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED201210028–89–7890999932––7––48–8–7853y28––46––8–2–14425–20–24––39–5–40221725–47–49––––93–––91––89–74––––49–––24 y––63–38––––37–––54––49––––
Countries and territories
Child labourChild marriage2000–2010*2000–2010*total male female married by 15 married by 18
Female genital mutilation/cuttingBirth1997–2010*registration2000–2010*prevalenceattitudestotalwomenadaughtersbsupport for the practicec
Justificationof wife beating2002–2010*malefemale
Violent discipline++2005–2010*total male female
FranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People'sDemocratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia(Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibiaNauruNepal
11–72321––––28 y26––36––16–5––1810822–––34 y
10–82521––––29 y25––33––18–6––1912921–––30 y
EM28BAFebr RGua Ory ED2012
––2518–34––21 y25571621–16––127y–11–––6––226––4
––2020–34–––26551722–16––128y–12–––7––227––4
––2917–34–––24601619–15––126y–9–––5––225––3
–1173–5––820746–11––184–3–––1–116––1
–343617–25––3563222030–39––4722–17–––9–10726––10
–895592–71–––43249381–94––4153–95–––89––996092–94
––78––4–––9650–––––––––––––––––27–––
––64––1–––5739–––––––––––––––––––––
––71––2–––6934–––––––––––––––––9–––
–––––22–––––––––––5116 y–––––––––44––––––4830––––3016 y–14 y–––––––––––––41–22
––747–37–––86401829–16––5431 y–59–––6–90 y1053––3881––3759––––3228–31 y87–––––––20116436–35–23
––8767–90––––8276––––––––86–––89––54–81 y–5474–––94––––––––––––––––8163––––––
––8670–91––––8279––––––––87–––90––57–––5875–––94––––––––––––––––8364––––––
––8763–89––––8174––––––––84–––87––51–––4972–––94––––––––––––––––7961––––––
13–62121––––27 y26––38––15–5
–––211––––149–015–615–5
––111938––––4850–455–2635–23
72––454y––––80––9381–9656––
––––58––––––––85––72––––––––––––
–––––––––––––69––66––––––––––––
–––––––––––––76––53––––––––––––
––178824–––38 y
–––0317–2210
––451652–92751
––989885 y3172678335
Statistical tables
121
TABLE 9: CHILD PROTECTIONChild labourChild marriage2000–2010*2000–2010*total male female married by 15 married by 18Female genital mutilation/cuttingBirth1997–2010*registration2000–2010*prevalenceattitudestotalwomenadaughtersbsupport for the practicecJustificationof wife beating2002–2010*malefemaleViolent discipline++2005–2010*total male female
Countries and territories
NetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent andthe GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and TobagoTunisiaTurkeyTurkmenistanTuvalu
–––8–224–48––––49–––––69––41086447–1–3y––
–––8–245–49––––45–––––79––598
EM28BAFebr RGua Ory ED2012
––154329––––––7y–1534 y––3y––161–35––
––184329––––––10 y–1731 y––4y––201–36––
––114329––––––4y–1236 y––3y––121–35––
––103617––7–7––2–32––––1––1––
––417539––19–24––21182014––––19––13––
––8132 y30––96 y–27––––9383––––98––82––
–––230 y–––––––––––––––––––––
–––130 y–––––––––––––––––––––
–––322–––––––––––––––––––––
––––30–––––––––––––––22 y––––––46–22––––58–––65–––––––41––––––81––––––73
––147043––––––––––14––––21––48–––61–20–656–65–––6976 y–––53 y–1338–––74 y–218653–8–2538 y70
–––––––95––––––––––––––––––––––––75–92–––72 y––––––86–––8978–72–93–77––––
––––––––––––––––––––––––––––––––75–92––––––––––87–––9080–77–94–78––––
––––––––––––––––––––––––––––––––74–93––––––––––85–––8875–67–93–77––––
–––7–214–48––––54–––––59––3118
–––5–101–19–––381––2–31––313
–––34–396–48–––22456––12–195––131320
–48–75–5599–51–––80392 y––97–9730––958899
–––––28––91––––98––––––––––––
–––––20––33––––46––––––––––––
–––––18––66––––65––––––––––––
7444–1–3y––
5449–1–2y––
036–2–31–
41925–8–147–
945578–96–949650
––4––––––
––0y––––––
––2––––––
122
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
Child labourChild marriage2000–2010*2000–2010*total male female married by 15 married by 18
Female genital mutilation/cuttingBirth1997–2010*registration2000–2010*prevalenceattitudestotalwomenadaughtersbsupport for the practicec
Justificationof wife beating2002–2010*malefemale
Violent discipline++2005–2010*total male female
UgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela(Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
25 y7––21 y–8y––8162341 y–13
27 y8––23 y–8y––9152142 y–14
24 y7––19 y–8y––6162440 y–12
120––7––09–1119412
4610––37––727–1032423034
21100––16––10026928822143833
1–––15––––––23 y1–89
––––3––––––20 y––43 y
––––6––––––41 y––45
6011––38––59 y––––49––
704––54––70––64–6249–
–70––––––78 y–9495–––
–76––––––––9595–––
–65––––––––9295–––
MEMORANDUMSudan and South Sudanδ
SUMMARY INDICATORS#
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Child labour– Percentage of children 5–14 years old involved in child labour at the moment of the survey. Achild is considered to be involved in child labour under the following conditions: children 5–11 years old who,during the reference week, did at least one hour of economic activity or at least 28 hours of household chores,or children 12–14 years old who, during the reference week, did at least 14 hours of economic activity or atleast 28 hours of household chores.Child marriage– Percentage of women 20–24 years old who were first married or in union before they were15 years old and percentage of women 20–24 years old who were first married or in union before they were18 years old.Birth registration– Percentage of children less than 5 years old who were registered at the moment of thesurvey. The numerator of this indicator includes children whose birth certificate was seen by the intervieweror whose mother or caretaker says the birth has been registered.Female genital mutilation/cutting–(a) Women:percentage of women 15–49 years old who havebeen mutilated/cut;(b) daughters:percentage of women 15–49 years old with at least one mutilated/cutdaughter;(c) support for the practice:percentage of women 15–49 years old who believe that the practiceof female genital mutilation/cutting should continue.Justification of wife beating– Percentage of women and men 15–49 years old who consider a husbandto be justified in hitting or beating his wife for at least one of the specified reasons, i.e., if his wife burns thefood, argues with him, goes out without telling him, neglects the children or refuses sexual relations.Violent discipline– Percentage of children 2–14 years old who experience any violent discipline(psychological aggression and/or physical punishment).
EM28BAFebr RGua Ory ED2012
AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld
293233341012**1310**85–17**2917**
303335331112**1311**95–17**3017**
29323135912**1210**74–16**2816**
11121114414 **183 **81–12 **1712 **
343835411839 **4618 **2911–35 **4735 **
443835417544 **3672 **9196–51 **3151 **
47414233––––––––––
2727–24––––––––––
2823–22––––––––––
–384529–44 **49––––43 **39–
57585957–48 **5236 **–27–49 **5548 **
––––90–––––––––
––––––––––––––
––––––––––––––
MAIN DATA SOURCES
Child labour– Multiple Indicator Cluster Surveys (MICS), Demographic and Health Surveys (DHS) and othernational surveys.Child marriage– MICS, DHS and other national surveys.Birth registration– MICS, DHS, other national surveys and vital registration systems.Female genital mutilation/cutting– MICS, DHS and other national surveys.Justification of wife beating– MICS, DHS and other national surveys.Violent discipline– MICS, DHS and other national surveys.
– Data not available.y Data differ from the standard definition or refer to only part of a country. Such data are included in thecalculation of regional and global averages.++A more detailed explanation of the methodology and the recent changes in calculating these estimates canbe found in the General Note on the Data, page 86.* Data refer to the most recent year available during the period specified in the column heading.** Excludes China.
NOTES
Statistical tables
123
Regional ClassificationAverages presented at the end of eachof the 13 statistical tables are calculatedusing data from the countries andterritories as classified below.AfricaSub-Saharan Africa; NorthAfrica(Algeria, Egypt, Libya, Morocco,Tunisia)Sub-Saharan AfricaEastern and Southern Africa; Westand Central Africa; Djibouti; Sudan1Eastern and Southern AfricaAngola; Botswana; Burundi; Comoros;Eritrea; Ethiopia; Kenya; Lesotho;Madagascar; Malawi; Mauritius;Mozambique; Namibia; Rwanda;Seychelles; Somalia; South Africa;SouthSudan1; Swaziland; Uganda;UnitedRepublic of Tanzania;Zambia;ZimbabweMalaysia; Marshall Islands; Micronesia(Federated States of); Mongolia;Myanmar; Nauru; Niue; Palau; PapuaNewGuinea; Philippines; Republic ofKorea; Samoa; Singapore; SolomonIslands; Thailand; Timor-Leste; Tonga;Tuvalu; Vanuatu; VietNamLatin America and CaribbeanAntigua and Barbuda; Argentina;Bahamas; Barbados; Belize; Bolivia(Plurinational State of); Brazil; Chile;Colombia; Costa Rica; Cuba; Dominica;Dominican Republic; Ecuador; ElSalvador; Grenada; Guatemala; Guyana;Haiti; Honduras; Jamaica; Mexico;Nicaragua; Panama; Paraguay; Peru;Saint Kitts and Nevis; Saint Lucia; SaintVincent and the Grenadines; Suriname;Trinidad and Tobago; Uruguay; Venezuela(BolivarianRepublic of)
is no established convention forthe designation of ‘developed’ and‘developing’ countries or areas in theUnitedNations system.Afghanistan; Algeria; Angola; Antiguaand Barbuda; Argentina; Armenia;Azerbaijan; Bahamas; Bahrain;Bangladesh; Barbados; Belize; Benin;Bhutan; Bolivia (Plurinational State of);Botswana; Brazil; Brunei Darussalam;Burkina Faso; Burundi; Cambodia;Cameroon; Cape Verde; Central AfricanRepublic; Chad; Chile; China; Colombia;Comoros; Congo; Cook Islands; CostaRica; Côte d’Ivoire; Cuba; Cyprus;Democratic Republic of the Congo;Democratic People’s Republic of Korea;Djibouti; Dominica; DominicanRepublic;Ecuador; Egypt; El Salvador; EquatorialGuinea; Eritrea; Ethiopia; Fiji; Gabon;Gambia; Georgia; Ghana; Grenada;Guatemala;Guinea; Guinea-Bissau;Guyana; Haiti; Honduras; India; Indonesia;Iran (Islamic Republic of); Iraq; Israel;Jamaica; Jordan; Kazakhstan; Kenya;Kiribati; Kuwait; Kyrgyzstan; Lao People’sDemocraticRepublic; Lebanon; Lesotho;Liberia; Libya; Madagascar; Malawi;Malaysia; Maldives; Mali; MarshallIslands; Mauritania; Mauritius; Mexico;Micronesia (FederatedStatesof);Mongolia; Morocco; Mozambique;Myanmar; Namibia; Nauru; Nepal;Nicaragua; Niger; Nigeria; Niue; OccupiedPalestinian Territory; Oman; Pakistan;Palau; Panama; Papua New Guinea;Paraguay; Peru; Philippines; Qatar;Republic of Korea; Rwanda; Saint Kittsand Nevis; Saint Lucia; SaintVincentand the Grenadines; Samoa; Sao Tomeand Principe; Saudi Arabia; Senegal;Seychelles; Sierra Leone; Singapore;Solomon Islands; Somalia; South Africa;South Sudan1; Sri Lanka; Sudan1;Suriname; Swaziland; Syrian ArabRepublic; Tajikistan; Thailand; Timor-Leste;Togo; Tonga; Trinidad and Tobago; Tunisia;Turkey; Turkmenistan; Tuvalu; Uganda;United Arab Emirates; United RepublicofTanzania; Uruguay; Uzbekistan;Vanuatu; Venezuela (Bolivarian Republicof); VietNam; Yemen; Zambia; Zimbabwe
West and Central AfricaBenin; Burkina Faso; Cameroon; CapeVerde; Central African Republic; Chad;Congo; Côte d’Ivoire; Democratic Republicof the Congo; Equatorial Guinea; Gabon;Gambia; Ghana; Guinea; Guinea-Bissau;Liberia; Mali; Mauritania; Niger; Nigeria;Sao Tome and Principe; Senegal;SierraLeone; Togo
Middle East and North AfricaAlgeria; Bahrain; Djibouti; Egypt; Iran(Islamic Republic of); Iraq; Jordan; Kuwait;Lebanon; Libya; Morocco; OccupiedPalestinian Territory; Oman; Qatar; SaudiArabia; Sudan1; Syrian Arab Republic;Tunisia; United Arab Emirates; YemenAsiaSouth Asia; East Asia and PacificSouth AsiaAfghanistan; Bangladesh; Bhutan; India;Maldives; Nepal; Pakistan; SriLankaEast Asia and PacificBrunei Darussalam; Cambodia; China;Cook Islands; Democratic People’sRepublic of Korea; Fiji; Indonesia; Kiribati;Lao People’s Democratic Republic;
124
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012CEE/CISAlbania; Armenia; Azerbaijan; Belarus;Bosnia and Herzegovina; Bulgaria;Croatia; Georgia; Kazakhstan; Kyrgyzstan;Montenegro; Republic of Moldova;Romania; Russian Federation; Serbia;Tajikistan; The former Yugoslav Republicof Macedonia; Turkey; Turkmenistan;Ukraine; UzbekistanIndustrialized countries/territoriesIndustrialized countries/territories aredefined as those not included in theUNICEF Regional Classification.Andorra; Australia; Austria; Belgium;Canada; Cyprus; Czech Republic;Denmark; Estonia; Finland; France;Germany; Greece; Holy See; Hungary;Iceland; Ireland; Israel; Italy; Japan;Latvia; Liechtenstein; Lithuania;Luxembourg; Malta; Monaco;Netherlands; New Zealand; Norway;Poland; Portugal; San Marino; Slovakia;Slovenia; Spain; Sweden; Switzerland;United Kingdom; United StatesDeveloping countries/territoriesDeveloping countries/territoriesare classified as such for purposesof statistical analysis only. There
Measuring human developmentAn introduction to Table 10
Least developed countries/territoriesLeast developed countries/territoriesare those countries and territoriesclassified as such by the United Nations.Afghanistan; Angola; Bangladesh;Benin; Bhutan; Burkina Faso; Burundi;Cambodia; Central African Republic;Chad; Comoros; Democratic Republicof the Congo; Djibouti; Equatorial Guinea;Eritrea; Ethiopia; Gambia; Guinea;Guinea-Bissau; Haiti; Kiribati; LaoPeople’s Democratic Republic; Lesotho;Liberia; Madagascar; Malawi; Mali;Mauritania; Mozambique; Myanmar;Nepal; Niger; Rwanda; Samoa; Sao Tomeand Principe; Senegal; Sierra Leone;Solomon Islands; Somalia; South Sudan1;Sudan1; Timor-Leste; Togo; Tuvalu;Uganda; United Republic of Tanzania;Vanuatu; Yemen; ZambiaIf development is to be measured using acomprehensive and inclusive assessment,it is necessary to appraise human as wellas economic progress. From UNICEF’spoint of view, there is a need for anagreed method of measuring the level ofchild well-being and its rate of change.The under-five mortality rate (U5MR)is used in Table 10 (pp. 126–129) as theprincipal indicator of such progress. In1970, around 16.6 million children weredying every year. In 2010, by comparison,the estimated number of children whodied before their fifth birthday stood at7.6 million – highlighting a significantlong-term decline in the global numberofunder-five deaths.it is much more difficult for a wealthyminority to affect a nation’s U5MR, andthis indicator therefore presents a moreaccurate, if far from perfect, pictureof the health status of the majority ofchildren and of society as a whole.The speed of progress in reducingU5MR can be assessed by calcul-ating its average annual rate of reduction(AARR). Unlike the comparison of absolutechanges, AARR reflects the fact that thelower limits to U5MR are approached onlywith increasing difficulty.As lower levels of under-five mortalityare reached, the same absolute reduc-tion represents a greater percentagereduction. AARR therefore shows a higherrate of progress for a 10-point reduction,for example, if that reduction happensat a lower level of under-five mortality. A10-point decrease in U5MR from 100 to90 represents a reduction of 10 per cent,whereas the same 10-point decreasefrom 20 to 10 represents a reduction of50 per cent. (A negative value for thepercentage reduction indicates an increasein U5MR during the period specified.)When used in conjunction with grossdomestic product (GDP) growth rates,U5MR and its rate of reduction can there-fore give a picture of the progress beingmade by any country, territory or region,over any period of time, towards thesatisfaction of some of the most essentialhuman needs.As Table 10 shows, there is no fixedrelationship between the annual reduc-tion rate of U5MR and the annual rate ofgrowth in per capita GDP. Such compari-sons help shed light on the relationshipbetween economic advances andhumandevelopment.Finally, the table gives the total fertilityrate for each country and territory and thecorresponding AARR. It is clear that manyof the nations that have achieved signifi-cant reductions in their U5MR have alsoachieved significant reductions in fertility.
1
Because of the cession in July 2011 of theRepublic of South Sudan by the Republic ofthe Sudan, and its subsequent admissionto the United Nations on 14 July 2011,disaggregated data for the Sudan andSouth Sudan as separate States are not yetavailable for most indicators. Aggregateddata presented are for the Sudan pre-cession, and these data are included in theMiddle East and North Africa region as wellas in all other categories according to theregional classification described on page 124.
EM28BAFebr RGua Ory ED2012U5MR has several advantages as a gaugeof child well-being:• First, U5MR measures an end result ofthe development process rather than an‘input’ such as school enrolment level,per capita calorie availability or numberof doctors per thousand population – allof which are means to an end.• Second, U5MR is known to be theresult of a wide variety of inputs: forexample, antibiotics to treat pneumonia;insecticide-treated mosquito nets toprevent malaria; the nutritional well-being and health knowledge of mothers;the level of immunization and oralrehydration therapy use; the availabilityof maternal and child health services,including antenatal care; income andfood availability in the family; the avail-ability of safe drinking water and basicsanitation; and the overall safety of thechild’senvironment.• Third, U5MR is less susceptible to thefallacy of the average than, for example,per capita gross national income (GNI).This is because the natural scale doesnot allow the children of the rich tobe one thousand times more likely tosurvive, even if the human-made scaledoes permit them to have one thousandtimes as much income. In other words,
Statistical tables
125
TABLE 10: THE RATE OF PROGRESSgDP per capitaaverage annualUnder-5Average annual rateTotalAverage annual rateUnder-5Reduction Reductiongrowth rate (%)mortality rateof reduction (%)Θfertility rateof reduction (%)Θmortalitysincesincerank1970 1990 2000 2010 1970–1990 1990–2000 2000–2010 1990–2010 1990 (%)Θ2000 (%)Θ1970–1990 1990–2010 1970 1990 2010 1970–1990 1990–2010
Countries and territories
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia(Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republicof the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopiaFijiFinland
1110869172814512698165172631181396198156172113205255145611031521303145815156699514210810334291421391815615617217273617231133819891118194916523113186
314–181–––70–2129–318423447–24–259285225–127129–39286226–21422151227248821101062221505872235–40–––24416–54127139237161–––2475416
209 151 14941 29 1868 49 36954243 200 16126 15827 20 1455 33 2096596493 67 4622 17 1617 12 10143 86 4818 17 2017 146106444 27 17178 143 115139 89 561211959591222205183121137859165207194837125116201715113131114451819123176252946219014121184307821096369211911641031486461761901133271041041313148897758548481971317614251136636159173918198693910123664433
2.0–4.9–––4.8–4.25.9–1.78.02.54.8–4.4–1.93.63.1–3.83.9–2.91.71.1–2.25.14.71.60.97.34.15.32.91.35.37.22.2–5.6–––1.52.9–5.83.64.94.64.8–––1.52.94.1
3.33.53.35.91.95.53.05.14.14.13.32.63.55.10.61.95.14.92.24.53.96.4-4.94.92.90.50.71.11.6-0.82.92.5-0.60.95.53.73.21.81.14.32.70.24.93.74.56.9-2.50.04.11.51.34.14.56.96.02.24.24.82.72.75.6
0.14.83.12.22.26.33.65.01.84.13.80.61.85.8-1.68.54.14.62.24.64.22.26.96.42.54.80.81.47.00.80.02.51.00.92.06.13.51.91.13.72.61.92.94.15.65.65.60.64.11.52.24.25.07.67.52.34.29.62.93.02.9
1.74.13.24.12.15.93.35.12.94.13.51.62.75.5-0.55.24.64.82.24.54.04.31.05.72.72.60.81.34.30.01.42.50.20.93.74.93.31.91.14.02.71.03.93.95.16.31.60.34.11.51.74.24.87.36.82.34.27.22.82.84.2
2956475634694864445651274166-1165606135605558196842411422581253941653634931205541195454647127656262956627774365776424357
13827202047303917333161744-18573337203734205047223881350802210918453017113123172533434343633142034395353203462252625
–-0.7 x1.6––8.3 x-0.7–1.52.4–1.9-1.3 x0.41.7–2.22.90.3–-1.1–8.22.3-2.2 x3.4 x1.41.1–3.42.0–-1.3-1.01.56.61.90.1 x3.1–0.7-1.9–3.95.9 x––-2.32.0–4.7 x2.11.34.1-1.9––1.5 x–0.72.9
–5.41.5–4.21.72.16.12.3 x1.85.51.02.8 x3.50.8 x4.51.61.91.25.31.58.9 x3.51.5-0.4 x3.32.4-1.66.3 x0.61.94.2-0.72.93.49.21.5-0.40.7–2.6-1.02.92.6 x2.1 x2.5–-3.11.5-1.4 x1.73.91.72.72.619.2-1.5 x5.02.91.22.6
7.74.97.4–7.3–3.13.22.72.34.63.56.56.93.12.32.26.36.76.76.62.96.65.05.82.26.66.85.96.22.26.96.06.54.05.55.67.16.3–5.07.92.04.02.62.0
8.03.24.7–7.2–3.02.51.91.53.02.63.74.51.71.91.64.56.75.84.91.74.72.83.51.76.86.55.75.91.75.35.86.72.62.33.15.65.4–3.26.31.71.82.41.8
6.31.52.3–5.4–2.21.71.91.42.21.92.52.21.61.41.82.85.32.43.31.12.81.82.01.55.94.32.64.51.72.44.66.01.91.62.44.94.5–1.84.41.51.51.51.5
-0.22.12.3–0.1–0.11.21.92.42.21.52.82.12.91.01.71.70.00.71.52.61.72.92.41.1-0.20.20.20.21.51.30.1-0.12.14.32.91.20.8–2.31.20.94.20.40.62.6-0.71.20.9–2.92.71.62.3-0.20.30.4-0.21.50.3
1.23.73.7–1.4–1.51.9-0.20.31.61.71.93.50.61.4-0.72.41.24.41.92.02.72.12.70.70.82.04.01.40.04.01.10.51.71.91.30.60.8–2.71.70.70.92.51.10.91.0-0.62.5–1.52.02.32.80.61.70.72.61.2-0.3
EM28BAFebr RGua Ory ED2012181 17064106 9115 1241 2733 2047 2234 16152 12193 61135141 10623 1743
4.0 2.4 2.06.22.17.4–6.26.35.96.25.76.62.16.84.51.97.11.76.2–3.53.74.44.05.96.21.97.13.41.75.81.93.8–2.62.52.72.35.24.51.74.22.71.9
126
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
gDP per capitaaverage annualUnder-5Average annual rateTotalAverage annual rateUnder-5Reduction Reductiongrowth rate (%)mortality rateof reduction (%)Θfertility rateof reduction (%)Θmortalitysincesincerank1970 1990 2000 2010 1970–1990 1990–2000 2000–2010 1990–2010 1990 (%)Θ2000 (%)Θ1970–1990 1990–2010 1970 1990 2010 1970–1990 1990–2010
FranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People'sDemocratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia(Federated States of)MonacoMongoliaMontenegroMoroccoMozambiqueMyanmarNamibiaNauruNepal
551399135241131931521864830156124215685211241136417276145691645656559
214–60175274139––2217732955266371279821885109––––182281171113–252
EM28BAFebr RGua Ory ED20121452138892274510178159222181022551151124244988 5417 1029 22127 85169 10327 176212753102 62167 9211647 15213 1788637 26116 11119 1529 171.9–2.33.40.95.6––5.10.52.05.64.81.94.53.32.86.34.0––––3.71.22.12.2–2.95.02.12.7-3.63.05.15.13.54.74.42.84.97.71.83.23.20.72.35.24.95.32.84.05.04.611.05.45.15.06.06.111.41.82.93.50.42.45.31.52.26.54.94.22.72.86.20.05.24.93.72.70.24.04.98.04.44.94.74.45.59.61.83.03.40.62.45.31.44.16.04.14.42.42.63.00.05.26352424556280596361596785304549103865255670565838414506539412433393767424039454568162530421411420483835242446040–3.4–2.5-4.2–2.2–2.7-2.3-0.14.0–0.26.5–-1.03.2 x1.656 49 42954107 61 3218 13886 55 36219 177 135112 87 6673 74 4040 40 40141 84 501.35.95.63.34.52.12.5-0.10.05.2–1.6––1.9-1.0 x1.4-2.1 x–1.0
17243289117243172136761710797–8815619346728567172165172881869173356013668
18–285–2618538–171317–82224–154431618816519611523–3362181028415115458–
99316547912213217822921066151–5819611585654691210386385799871572
5488 74128 9833 225499 748415 1149 32175 130177 15047 30109 165––37 241164286 6354 3544 2643 3974756430 245329 2244 33111 8565 4913 1152 38
3.5–2.7–5.32.15.4–3.91.6–1.12.0–4.94.14.92.53.35.54.64.7–6.02.45.54.91.92.12.96.8–
5.90.62.53.55.92.14.93.44.62.71.73.43.3–4.55.54.12.94.53.90.72.55.45.12.41.82.72.6-1.12.91.43.3
2.21.72.74.12.22.96.93.14.33.01.74.5-4.1–4.36.16.93.14.35.31.05.63.44.12.25.12.82.92.72.81.73.1
4.11.12.63.84.12.55.93.24.52.81.73.9-0.4–4.45.85.53.04.44.60.84.14.44.62.33.52.72.70.82.91.63.2
562041535639694859432955-9–596867455960155658603750424214442747
201623332025502735261536-51–35455027354194329332040242523251527
2.20.20.7–2.3-2.01.34.2 x0.2–0.1-1.6––0.83.03.22.14.7-2.3–2.81.92.8-1.33.42.5 x–1.2-5.3-6.8 x–
1.3-0.90.12.71.32.42.62.91.31.2-1.72.5-1.1 x–1.62.92.24.92.62.7 x-2.2 x4.71.80.90.70.82.53.90.31.22.0 x0.54.34.52.42.21.72.9 x3.0 x3.52.9-0.21.03.24.9 x2.72.6 x-1.10.93.51.50.32.2 x3.13.7 x2.44.38.2 x2.1–1.9
2.54.76.12.62.07.02.44.66.26.86.15.65.8–7.32.03.05.55.56.57.43.83.82.55.52.17.93.58.1–7.24.96.01.95.15.86.77.6–2.32.07.37.34.97.26.92.0–6.84.06.76.9–7.62.47.16.66.16.5–6.1
1.85.26.12.21.45.61.43.85.66.76.62.65.4–5.11.82.23.93.14.86.02.03.01.32.91.65.82.86.0–2.63.96.21.93.14.96.54.8–2.01.66.36.83.56.17.12.1–5.92.33.45.0–4.11.94.06.23.45.2–5.2
2.03.34.91.61.44.21.52.24.05.25.12.33.3–3.11.42.12.62.11.74.72.12.91.42.31.43.12.64.7–2.32.72.71.51.83.25.22.6–1.51.64.76.02.61.86.31.3–4.51.62.33.5–2.51.72.34.92.03.2–2.7
1.8-0.50.00.91.91.12.50.90.60.1-0.53.80.3–1.70.61.61.72.81.51.03.21.23.23.11.51.61.11.5–5.11.2-0.10.02.40.80.12.3–0.71.10.80.41.60.8-0.1-0.2–0.72.73.41.7–3.11.22.80.32.81.1–0.8
-0.62.31.11.7-0.21.5-0.32.71.71.31.40.72.4–2.51.30.12.01.95.31.2-0.30.1-0.51.20.73.20.51.2–0.61.84.01.32.82.21.13.2–1.5-0.31.50.61.46.30.62.3–1.31.81.91.8–2.50.62.91.22.72.4–3.2
Statistical tables
127
TABLE 3: HEALTH10: THE RATE OF PROGRESSgDP per capitaaverage annualUnder-5Average annual rateTotalAverage annual rateUnder-5Reduction Reductiongrowth rate (%)mortality rateof reduction (%)Θfertility rateof reduction (%)Θmortalitysincesincerank1970 1990 2000 2010 1970–1990 1990–2000 2000–2010 1990–2010 1990 (%)Θ2000 (%)Θ1970–1990 1990–2010 1970 1990 2010 1970–1990 1990–2010
Countries and territories
NetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent andthe GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogoTongaTrinidad and TobagoTunisiaTurkeyTurkmenistanTuvalu
97981933710842152126418614518681151–165113–7839186165118461301335424118811181085273
97––97179275–6736127––102–––2975––1751318119–102
EM28BAFebr RGua Ory ED201227271294451392917276818104518060–1132–529678381163222 2123 205287 8026 18119 7513714 14233 174431285335 27180 18078 57––7523 17––40 31114 78436523 1693 6318 136.4––0.26.93.4–6.91.36.1––4.1–––4.84.3––3.03.14.15.7–5.8––1.92.81.86.64.6––2.01.68.80.85.51.68.01.91.76.94.16.92.50.0-2.6–4.53.3–2.6-1.75.62.95.02.25.88.94.91.72.21.55.66.22.82.60.51.49.20.83.74.66.20.02.92.94.15.12.60.03.1–3.43.0–2.53.82.91.83.63.93.32.96.41.92.21.75.68.72.82.91.31.59.00.84.63.17.11.02.34.94.16.02.60.00.3–3.93.2–2.61.04.22.44.33.14.55.95.61.82.21.65.67.52.82.72226831560467618376356704005–5547–4019573858465969673036276778434251360831374602525334023027–2926–233225173032282547172016435824253.3–––-1.4-0.7–2.9-0.55.6–––-0.80.1–1.93.0–-2.2 x3.01.81.22.0–4.7––-0.6–0.52.52.0––
1721568112129118691142331039849871038015617214516510312613331145118
1621159328251–16–196173–681517416486366679526864402137163
81168311213149454712433339050785917152183737271632823
647643 27218 143186 14329 225331 22229101 8725 1926 2074 6135 2541 1940 29106741386526 1927 1423 12177 9116818 16
3.53.24.20.30.8–2.9–7.11.7–3.62.62.03.71.93.87.46.69.43.02.72.01.34.75.0
2.94.54.63.61.4-7.35.93.77.62.12.82.42.03.66.43.95.37.64.82.93.53.21.6-0.85.62.5
4.11.54.74.22.62.85.13.48.91.52.72.61.93.47.73.25.15.64.91.83.16.66.56.76.91.2
3.53.04.63.92.0-2.35.53.68.31.82.82.51.93.57.13.65.26.64.82.43.34.94.12.96.31.8
5045605433-576751813042393250765165736238496256447130
3314373423244029591424231829542840433817274848495011
1.60.8-3.7-2.1-1.4–3.2–3.33.0–0.3-0.73.1-0.60.6–2.6–6.2–0.9 x–1.26.3 x5.3 x
2.01.91.9-0.21.9–2.1-2.4 x2.0 x1.7-0.2 x3.2-0.20.13.02.04.41.6–4.2-0.62.82.12.32.21.03.63.0––0.4 x1.11.51.81.13.93.73.3-1.0–1.3–2.14.1–1.5 x1.62.20.91.6-0.12.91.0-0.5 x0.01.65.03.52.35.1–
2.43.16.97.46.5–2.57.97.36.6–5.36.25.76.36.32.23.06.94.52.62.92.08.1–6.16.06.1–6.57.37.42.4–5.93.22.52.36.97.25.6–2.94.3–5.76.92.02.17.66.95.63.15.97.15.93.56.65.56.3–
1.62.14.87.86.4–1.96.57.26.0–3.04.84.53.84.32.01.54.21.62.41.91.97.0–3.43.04.8–5.45.86.62.1–5.71.82.01.55.96.63.7–1.32.5–2.75.72.01.55.35.22.12.15.36.34.62.43.63.04.3–
1.82.22.67.15.5–1.94.52.33.4–2.54.03.02.53.11.41.32.31.31.51.41.55.4–2.02.13.9–3.72.84.81.6–5.01.31.31.44.26.32.5–1.52.3–2.33.41.91.52.93.31.61.46.24.13.91.62.02.12.4–
2.22.01.9-0.30.1–1.50.90.10.5–2.81.21.22.51.90.43.32.55.20.32.10.30.7–2.93.61.2–0.91.10.50.6–0.12.91.02.00.80.42.1–3.82.8–3.60.90.11.61.81.44.91.90.50.61.21.83.03.01.9–
-0.6-0.23.00.50.7–-0.21.95.72.8–1.01.02.12.11.62.00.73.10.92.51.61.11.4–2.71.81.1–1.93.71.61.4–0.71.62.20.21.60.22.0–-0.40.4–0.82.70.20.23.02.31.52.0-0.82.20.92.03.01.93.0–
– 39 16 12– 169 104 55217 147 124 10344 25 20 1653 37 32 27182 49 28 16200 80 43 18– 98 74 56– 57 44 33
128
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
gDP per capitaaverage annualUnder-5Average annual rateTotalAverage annual rateReduction ReductionUnder-5growth rate (%)mortality rateof reduction (%)Θfertility rateof reduction (%)Θsincesincemortalityrank1970 1990 2000 2010 1970–1990 1990–2000 2000–2010 1990–2010 1990 (%)Θ2000 (%)Θ1970–1990 1990–2010 1970 1990 2010 1970–1990 1990–2010
UgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela(Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
2713015216541145136571261089040213724
193 175 14432 21 1891 22 122197208 155 13023 11955 23 17– 77 63102 39 23
991375768115214
0.52.17.14.21.53.74.4–4.83.2–3.9-0.12.21.2
1.91.56.12.51.82.03.02.05.32.83.82.51.5-3.90.9
3.73.35.43.45.41.24.41.95.03.34.22.63.53.61.0
2.82.45.72.93.61.63.72.05.13.04.02.52.5-0.11.0
43386844512752326445554039-318
312842294211351739283423293010
––-4.9 x2.0–2.10.9–1.1 x-1.6––-2.3-0.40.1
3.60.40.5 x2.12.41.82.02.26.80.36.01.5 x0.6-3.23.6
7.12.16.62.36.82.22.96.56.35.47.47.57.47.4
7.11.94.41.86.21.92.54.24.93.43.68.76.55.2
6.11.41.71.95.52.12.12.43.92.51.85.26.33.3
0.00.62.01.20.40.70.72.21.22.23.6-0.70.71.80.5
0.71.34.6-0.10.6-0.31.02.81.21.73.42.50.22.31.5
62 33 25 18– 51 35 23280 128 100 77179 183 157 111120 78 115 80158 125 114 103
MEMORANDUMSudan and South Sudanδ6.6 6.0 4.4
SUMMARY INDICATORS#
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Under-five mortality rate– Probability of dying between birth and exactly 5 years of age, expressedper 1,000live births.Reduction since 1990 (%)– Percentage reduction in the under-five mortality rate (U5MR) from 1990 to 2010.The United Nations Millennium Declaration in 2000 established a goal of a two-thirds (67 per cent) reductionin U5MR from 1990 to 2015. This indicator provides a current assessment of progress towards this goal.gDP per capita– Gross domestic product (GDP) is the sum of value added by all resident producers plus anyproduct taxes (less subsidies) not included in the valuation of output. GDP per capita is gross domestic productdivided by midyear population. Growth is calculated from constant price GDP data in local currency.Total fertility rate– Number of children who would be born per woman if she lived to the end of herchildbearing years and bore children at each age in accordance with prevailing age-specific fertility rates.
EM28BAFebr RGua Ory ED2012MAIN DATA SOURCESNOTES
AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld
2292342152561871461941151188824156240139
1601741561967786120555450109717088
14215413717555658938353778013873
1111219814341486724232366311057
1.81.51.61.34.42.62.43.73.92.84.42.41.72.3
1.21.21.31.13.42.83.03.74.33.03.61.92.11.9
2.52.43.42.02.93.02.84.64.24.81.52.42.32.5
1.81.82.31.63.22.92.94.14.33.92.62.22.22.2
3130372747444456575440353535
2221281825262537343814212022
0.90.00.3-0.5-0.24.52.15.61.4–2.42.5-0.22.4
2.12.01.91.82.46.94.57.41.62.31.64.83.22.6
6.76.76.86.66.75.65.75.65.32.82.35.76.74.7
5.96.26.06.55.03.24.22.63.22.31.73.65.93.2
4.54.94.65.42.82.22.71.82.21.81.72.64.22.5
0.60.30.60.11.52.81.63.82.50.91.42.30.61.9
1.31.21.41.02.81.92.21.91.81.4-0.11.71.71.4
Under-five mortality rate– Inter-agency Group for Child Mortality Estimation(UNICEF, World Health Organization, United Nations Population Division and the World Bank).gDP per capita– The World Bank.Fertility– United Nations Population Division.
– Data not available.ΘA negative value indicates an increase.x Data refer to years or periods other than those specified in the column heading.Such data are not included in the calculation of regional and global averages.
Statistical tables
129
TABLE 11: ADOLESCENTSAdolescent population(aged 10–19)Adolescentsas proportionof totalpopulationTotal(%)(thousands)20102010Marital statusAdolescentsaged 15–19 whoare currentlymarried/in union(2000–2010*) (%)male femaleAge atAdolescentJustification offirst birthbirth ratewife-beatingWomenNumberAdolescents aged 15–19aged 20–24of birthswho think a husband iswho gaveper 1,000justified in hitting or beatingbirth before girls agedhis wife under certainage 18 (%)15–19circumstances (2002–2010*) (%)2000–2010* 2000–2010*malefemaleUse of mass mediaSecondary education HIV knowledgeAdolescents agedLowerUpperAdolescents aged15–19 who use at least secondary secondary 15–19 who haveone type of information grossgrosscomprehensivemedia at least once a enrolment enrolment knowledge of HIVweek (2000–2010*) (%)ratioratio(2005–2010*) (%)malefemale2007–2010*malefemale
Countries and territories
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republicof the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopia
7,7715616,571–4,553–6,7974572,9119421,4775914931,514381,0751,209722,0421492,20944643733,729647243,8801,9473,2864,4224,1881151,0122,6182,817200,6608,752155888–8364,5634991,4831541,1104,12315,877701201–1,9642,82915,9261,4621511,14413820,535
251819–24–171513111617122114111123232122122217161024232323122323231615192122–18231113141117241323–2020202422221025
–1–––––0––0–––––––2–4–––––––2––2––––––2––2–––––––––3––––––2
–82––––7––10––46–4––2215137–25––2410822–85942––14–19–1020–––––25–4–19161321–29–22
–3–––––3––4––40––––23–20––16 x––27–933–2238 x48––2017 x29––29–––––23–––25–7––25–28
151204916567652717104139131335122119111446891551771744128305214114921331935368495132476711114506121
–37–––––31––63–––––––12––––––––––––24–––––––––––––––
–2466––––22––39––41–––144170174––––68–4958–23––––––76––63–––––
–97–––––99––97–––––––83–100–––––70–8877–88–55––––75––86–––––
–99–––––99––95––63 y––––64–97–––––59–8761–88–24––––63––75–––––
6293135842512610598115102939710156–9611187–749410691107116832729565097101182910192103–––113–1049210299–481174011988858979–4610243
245351742187678316699113899231–7810652–3874776792859110112329105–817856677–––71–87879592–31119188771664646–219715
–21–––––7––2–––––––31–24–––––––41––3626–––––18––30–––––––––33–16––––32
–3612––––19––3––7–32–3917222245––––18305032–371610––21–8––18–54––713–16–39–3––––21
130
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012135627479810050681288524109––––14––––––5372–––6–50 y––70–7755–––98––––––3443–––98–97 y––85–27
Countries and territories
Adolescent population(aged 10–19)Adolescentsas proportionof totalpopulationTotal(%)(thousands)20102010
Marital statusAdolescentsaged 15–19 whoare currentlymarried/in union(2000–2010*) (%)male female
Age atAdolescentJustification offirst birthbirth ratewife-beatingWomenNumberAdolescents aged 15–19aged 20–24of birthswho think a husband iswho gaveper 1,000justified in hitting or beatingbirth before girls agedhis wife under certainage 18 (%)15–19circumstances (2002–2010*) (%)2000–2010* 2000–2010*malefemale
Use of mass mediaSecondary education HIV knowledgeAdolescents agedLowerUpperAdolescents aged15–19 who use at least secondary secondary 15–19 who haveone type of information grossgrosscomprehensivemedia at least once a enrolment enrolment knowledge of HIVweek (2000–2010*) (%)ratioratio(2005–2010*) (%)malefemale2007–2010*malefemale
FijiFinlandFranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People'sDemocratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia(Federated States of)MonacoMongoliaMontenegroMoroccoMozambique
1,5162297795318911,105–412614,9203,5835,455693,61252–77621321,66927–519846,1685,402
EM28BAFebr RGua Ory ED2012241018242217–1212242419222312–22161924–19131923–––13––––11––––––––––––––––––1619––––3433–540––25–15––421140–––1338––––3634–146––25––––3–842110151892177442091471771215190208888349051–201718185–––5437––––3328––––––––––––––79––4848––––3532–4183–––––––1766437–––6473––––6184––81––55–––––––95–––6963––––6070–10079––44––––––9088
1616347,4603444095758,2025,3271,091213,3882,2863431772,265–1,7641,09746242,99142,79712,6127,2625641,1845,74456511,8731,4082,4979,135–3811,120
191212232413102210202423232323–2311142018172313169219231623–1421
–––2–––1–––3––2––––5––––––––––0–––
–––182511–8––1836191417–20––30131719–––5–6512––8
–––35–––16––2244–2215–26––2210–––––––46x26––4x
30911144 x10444107012549215313710169–108201545523168171576053231106391230
–––––––28–––––––––––57––––––––––54–––
––––715–41–––79391929–18––5341 y–57–––6–91 y757––28
–––89–––90–––66–9488––––88––––––––––91–––
–––83–––85–––55–9683–98––7279 y–––––––97 y–81–––
94102110–6595102781041156245–122––68100997793100631077110295102951079098979253968957––104981084336941225099932696117100–951097432
62116117–48811023599774725–71––609811547667339134108998510174714371806534907527––10610187151550–2610370238162––87883810
–––––––30––2420–4534––––352y–––––––––52––––––2821––––2642––––3510–––––––31
––––4012–28––2017125331–28––196y–2–––59–12 y2242––19–––3518––––2342–22 y14–274––––3229–37
Statistical tables
131
TABLE 3: HEALTH11: ADOLESCENTSAdolescent population(aged 10–19)Adolescentsas proportionof totalpopulationTotal(%)(thousands)20102010Marital statusAdolescentsaged 15–19 whoare currentlymarried/in union(2000–2010*) (%)male femaleAge atAdolescentJustification offirst birthbirth ratewife-beatingWomenNumberAdolescents aged 15–19aged 20–24of birthswho think a husband iswho gaveper 1,000justified in hitting or beatingbirth before girls agedhis wife under certainage 18 (%)15–19circumstances (2002–2010*) (%)2000–2010* 2000–2010*malefemaleUse of mass mediaSecondary education HIV knowledgeAdolescents agedLowerUpperAdolescents aged15–19 who use at least secondary secondary 15–19 who haveone type of information grossgrosscomprehensivemedia at least once a enrolment enrolment knowledge of HIVweek (2000–2010*) (%)ratioratio(2005–2010*) (%)malefemale2007–2010*malefemale
Countries and territories
MyanmarNamibiaNauruNepalNetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent andthe GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogo
2143–404,9312,9411,225–1,3327406611971192,0789,956–4,2763,173–953031,1218774,7071,68110,2672862951,393
EM28BAFebr RGua Ory ED2012
8,763526–6,9352,0136181,3263,64435,326–6461,02249539,911–6391,5211,3765,77120,2014,4871,1001366,5954952,31814,6462,314–33
1823–231214232322–13251823–1822212022121081414111022–191923–24182412–23151210222220–915–18261211232415142623
–0–10–––31–––––––3–––––––1––1–––1–1–6––1–––––2–––––0––––––0–
–5–32––245929––13–16––15111110––––10––3–––7–20–296–30––––254––9–117––106152812
–172223––285128––––10–––16 x157––––5––7––
1774841065341091991235396014162987706569531616152243930436750
–44–27––––35–––––––––––––––25–––––
–38–24––196840––––––––––15––––24––51––
–86–88–––6682–––––––––––––––99––79––
–88–80––954864–––––––––9194––––98––60––
6183––126105781734–988992449890–7898889911610299899985361011051219695691023999110––9396541096–119104–9064102110989590916051
3835––11615353426–1238091259455–567565999871958789841789839167962091178498––919719692–125––553710385365962764127
–59845–––1428––––––––––––––––––49–––5–39–21––26–––26–––––––52–––9––15–
3162829–––1220––––2––––1719–––––––45–––2–39–1843–16–––293–––––4156––61146231115
–5–25–22––40–––15–15––4––28–––––
72291110796225914352257012354–1323–6611164752743
–50–25––––57–––73–––––––59––––––72–
–58–23–665–55–––7275 y–––54 y–1954–––85 y–148154
–97–96–61––66–––––––––––94––––––61–
–97–95–89––51–––––––––––89––––––62–
–919 x
205489 x
132
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
Adolescent population(aged 10–19)Adolescentsas proportionof totalpopulationTotal(%)(thousands)20102010
Marital statusAdolescentsaged 15–19 whoare currentlymarried/in union(2000–2010*) (%)male female
Age atAdolescentJustification offirst birthbirth ratewife-beatingWomenNumberAdolescents aged 15–19aged 20–24of birthswho think a husband iswho gaveper 1,000justified in hitting or beatingbirth before girls agedhis wife under certainage 18 (%)15–19circumstances (2002–2010*) (%)2000–2010* 2000–2010*malefemale
Use of mass mediaSecondary education HIV knowledgeAdolescents agedLowerUpperAdolescents aged15–19 who use at least secondary secondary 15–19 who haveone type of information grossgrosscomprehensivemedia at least once a enrolment enrolment knowledge of HIVweek (2000–2010*) (%)ratioratio(2005–2010*) (%)malefemale2007–2010*malefemale
MEMORANDUMSudan and South Sudanδ9,804
EM28BAFebr RGua Ory ED201223–2517 x72 x––––
TongaTrinidad and TobagoTunisiaTurkeyTurkmenistanTuvaluUgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela(Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
231961,75713,0421,031–8,0634,8898777,48310,19841,4495265,941535,48215,8075,9743,0873,223
2215171820–2411121223131622221918252426
––––––23––4–––––––1–
–6–105–206––18––513165191821
–––823353––28––4––425 x3421
1633651212315930222611640602692 x1013580151101
–––––83698––39––63––––55–
–10–3037 y69703––52––63––53–6157
––––––8799––79–––––97–8068
––––96–7899––70–––––94–7160
–9111691––33961011033899108974890––––53
–867372––15918796588681204670––––28
–––––573833––41–––––––38––
–49––4313139––46––2714–452y3651–
SUMMARY INDICATORS#AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld228,066196,54092,30294,23282,264655,548332,513323,035108,36155,069114,9331,061,866190,4451,202,710
2223232320182016191412192318
2231–5 **5–––––––
222419281525 **3011 **187–22 **2922 **
25282729–19 **228 **–––20 **3220 **
108123116130383653198134225612352
–4350––56 **56–––––––
57576055–48 **5138 **–31–50 **5649 **
72726874–89 **88––––83 **67–
65616161–74 **7186 **–––72 **5972 **
524447408980718910293103774680
3127292554514264748499512456
31323827–30 **35––––30 **––
23253318517 **1622 **–––19 **2119 **
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Marital status– Percentage of boys and girls aged 15–19 who are currently married or in union. Thisindicator is meant to provide a snapshot of the current marital status of boys and girls in this age group.However, it is worth noting that those not married at the time of the survey are still exposed to the risk ofmarrying before they exit adolescence.Age at first birth– Percentage of women aged 20–24 who gave birth before age 18. This standardized indicatorfrom population-based surveys captures levels of fertility among adolescents up to the age of 18. Note that the dataare based on the answers of women aged 20–24, whose risk of giving birth before the age of 18 is behind them.Adolescent birth rate– Number of births per 1,000 adolescent girls aged 15–19.Justification of wife-beating– The percentage of boys and girls aged 15–19 who consider a husband tobe justified in hitting or beating his wife for at least one of the specified reasons: if his wife burns the food,argues with him, goes out without telling him, neglects the children or refuses sexual relations.Use of mass media– The percentage of boys and girls aged 15–19 who make use of at least one of thefollowing types of information media at least once a week: newspaper, magazine, television or radio.Lower secondary gross enrolment ratio– Number of children enrolled in lower secondary school,regardless of age, expressed as a percentage of the total number of children of official lower secondaryschool age.Upper secondary gross enrolment ratio– Number of children enrolled in upper secondary school,regardless of age, expressed as a percentage of the total number of children of official upper secondaryschool age.Comprehensive knowledge of HIV– Percentage of young men and women (aged 15–19) who correctlyidentify the two major ways of preventing the sexual transmission of HIV (using condoms and limitingsex to one faithful, uninfected partner), who reject the two most common local misconceptions about HIVtransmission and who know that a healthy-looking person can be HIV-positive.
MAIN DATA SOURCES
Adolescent population– United Nations Population Division.Marital status– Demographic and Health Surveys (DHS), Multiple Indicator Cluster Surveys (MICS)and other national surveys.Age at first birth– DHS.Adolescent birth rate– United Nations Population Division.Justification of wife-beating– DHS, MICS and other national surveys.Use of mass media– AIDS Indicator Surveys (AIS), DHS and other national surveys.gross enrolment ratio– UNESCO Institute for Statistics (UIS).Comprehensive knowledge of HIV– AIS, DHS, MICS, Reproductive Health Surveys (RHS) and othernational household surveys; HIV/AIDS Survey Indicators Database, <www.measuredhs.com/hivdata>.– Data not available.x Data refer to years or periods other than those specified in the column heading. Such data are not includedin the calculation of regional and global averages.y Data differ from the standard definition or refer to only part of a country. Such data are included in thecalculation of regional and global averages.* Data refer to the most recent year available during the period specified in the column heading.** Excludes China.
NOTES
Statistical tables
133
TABLE 12: EQUITY – RESIDENCEBirth registration (%)2000–2010*ratio ofurbanurban rural to ruralUnder-fives withComprehensivediarrhoea receivingUnderweight% of populationknowledge of HIV (%)oral rehydration andprevalence inusing improvedSkilled attendantPrimary school netchildren under five (%) continued feeding (%)sanitation facilitiesat birth (%)attendance ratiofemales 15–242006–2010*2006–2010*2006–2010*2005–2010*2005–2010*2008ratio ofratio ofratio ofratio ofratio ofratio ofurbanurbanurbanurbanruralurbanurban rural to rural urban rural to urban urban rural to rural urban rural to rural urban rural to rural urban rural to rural
Countries and territories
AfghanistanAlbaniaAlgeriaAndorraAngolaAntigua and BarbudaArgentinaArmeniaAustraliaAustriaAzerbaijanBahamasBahrainBangladeshBarbadosBelarusBelgiumBelizeBeninBhutanBolivia (Plurinational State of)Bosnia and HerzegovinaBotswanaBrazilBrunei DarussalamBulgariaBurkina FasoBurundiCambodiaCameroonCanadaCape VerdeCentral African RepublicChadChileChinaColombiaComorosCongoCook IslandsCosta RicaCôte d'IvoireCroatiaCubaCyprusCzech RepublicDemocratic People'sRepublic of KoreaDemocratic Republicof the CongoDenmarkDjiboutiDominicaDominican RepublicEcuadorEgyptEl SalvadorEquatorial GuineaEritreaEstoniaEthiopia
1242.799981.099991.0–––34191.7––––––97951.0––––––96921.0––––––1391.5–––––––––92971.068561.2100 1001.076721.199 1001.078671.2–––––––––86581.562601.071661.186581.5––––––72362.0363 11.9––––––97951.087831.188 y 75 y 1.2 y––––––79412.0–––100 y 100 y 1.0 y––––––10024–90–8289999943––2910029–82–7092999924––51.00.8–1.1–1.21.01.01.01.8––5.9
35 x10098–71––100––97––41–100 x–998490881009998––66889586–91 x8260100 x1009979 x96 x–10084––––10093–95–9898 x909787 x65 x–45 x
7x9992–26––99––80––22–100 x–936954511009094––51586746–64 x261299 x999457 x73 x–9940––––100
5.0 x1.01.1–2.8––1.0––1.2––1.9–1.0 x–1.11.21.61.71.01.11.0––1.31.51.41.9–1.4 x3.15.11.0 x1.01.11.4 x1.3 x–1.02.1––––1.0
–53––––3––4––33–1x–2151132x–2–––16199––2222–3x3–8x––9––––13
–64––––7––12––43–2x–6211461x–2–––283022––2633–8x5–15 x––20––––27
–1.21.4––––2.6––3.1––1.3–1.7 x–2.91.41.32.30.7 x–0.8–––1.71.62.4––1.21.5–2.7 x1.6–2.0 x––2.2––––2.0
–6426––––62 x––21––70–53 x––43602842––––5227 x45 x29––5239––5548 x40 x––48––––7136–32–58–17–34 x67 x–28 x
–6323––––56 x––41––68–56 x––41623058––––4123 x51 x18––4319––4527 x38 x––43––––6338–63–51–20–37 x49 x–14 x
–1.01.1––––1.1 x––0.5––1.0–0.9 x––1.11.00.90.7––––1.31.2 x0.9 x1.6––1.22.1––1.21.8 x1.1 x––1.1––––1.10.9–0.5–1.1–0.8–0.9 x1.4 x–1.9 x
73 x9098–85–––––74––86–92–977496989889–––7991–90––66–––9141 x––9667––––
47 x9195–67–––––72––86–95–945590969885–––3870–71––42–––9129 x––9648––––9970–49–89–87–––––
1.6 x1.01.0–1.3–––––1.0––1.0–1.0–1.01.31.11.01.01.0–––2.11.3–1.3––1.6–––1.01.4 x––1.01.4––––1.01.2–1.4–1.0–1.0–––––
–5116––––26––7––––33–4922323246––––35536242––2118––26–9––19–55––1121–18–42–7––––44
–2610––––17––2––––34–291115942––––10294718––137––17–6––17–49––412–9–37–3––––14
–2.01.7––––1.5––3.3––––1.0–1.71.92.13.51.1––––3.61.81.32.4––1.62.6––1.5–1.5––1.1–1.1––2.81.7–2.0–1.2–2.3––––3.2
6098981008698919510010085100100561009110093248734997487–1003349675610065432398588150311009536999410099–
30988810018–778010010077100–5210097100864549923937–1006461835993828483525530291009611988110097–
2.01.01.11.04.8–1.21.21.01.01.11.0–1.11.00.91.01.16.01.63.81.11.92.4–1.05.51.13.71.61.01.71.55.81.21.11.51.71.11.01.03.31.01.21.01.0–
EM28BAFebr RGua Ory ED201210086–67–88–91–––––661.4––402.3––971.099 x 1.0 x721.2941.049 x 1.8 x10 x 6.2 x––3 x 17.2 x17–18–––64y–23 x–17 x27–27–––67y–40 x–35 x1.6–1.5–––1.02.0 y–1.7 x–2.0 x
23 23 1.0100 100 1.063 10 6.3–––87 74 1.296 84 1.197 92 1.189 83 1.1–––524 13.096 94 1.0298 3.6
134
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
Birth registration (%)2000–2010*ratio ofurbanurban rural to rural
Under-fives withComprehensivediarrhoea receivingUnderweight% of populationknowledge of HIV (%)oral rehydration andprevalence inusing improvedSkilled attendantPrimary school netchildren under five (%) continued feeding (%)sanitation facilitiesat birth (%)attendance ratiofemales 15–242006–2010*2006–2010*2006–2010*2005–2010*2005–2010*2008ratio ofratio ofratio ofratio ofratio ofratio ofurbanurbanurbanurbanruralurbanurban rural to rural urban rural to urban urban rural to rural urban rural to rural urban rural to rural urban rural to rural
Fiji–Finland–France–Gabon90Gambia57Georgia97Germany–Ghana82Greece–Grenada–Guatemala–Guinea78Guinea-Bissau30Guyana96Haiti87Holy See–Honduras95Hungary–Iceland–India59Indonesia71Iran (Islamic Republic of)–Iraq95Ireland–Israel–Italy–Jamaica89Japan–Jordan–Kazakhstan99Kenya76Kiribati100Kuwait–Kyrgyzstan96Lao People's84Democratic RepublicLatvia–Lebanon–Lesotho43Liberia5yLibya–Liechtenstein–Lithuania–Luxembourg–Madagascar92Malawi–Malaysia–Maldives93Mali92Malta–Marshall Islands96Mauritania75Mauritius–Mexico–Micronesia (Federated States of)–Monaco–Mongolia98Montenegro98Morocco92 yMozambique39
EM28BAFebr RGua Ory ED20121.2––1.01.9 y––––1.2––1.01.2–1.01.8––––1.01.01.1 y1.468––8879––––8278–9980–9790–98––10010085 x7811––5432––––3950–9338–6839–87––999840 x466.2––1.62.4––––2.11.6–1.12.1–1.42.3–1.1––1.01.02.2 x1.720––1217––––31 x10–1120–––––––5x2x6x1434––1320––––37 x13–2029–––––––6x1x12 x201.7––1.11.2––––1.2 x1.3–1.81.5–––––––1.2 x0.7 x2.1 x1.5–––4950––––6236––43––39––––42 x–51 x51–––4746––––4725––37––28––––49 x–41 x45–––1.01.1––––1.31.4––1.2––1.4––––0.9 x–1.2 x1.193––9346––––9388–8379––72––––9697968975––8821––––7788–8352––49––––949883781.2––1.02.2––––1.21.0–1.01.5––1.5––––1.01.01.21.1
–––875487–65–––33219278–93––3541–96–––88––995780–93
–––1.01.11.1–1.3–––2.41.41.01.1–1.0––1.71.7–1.0–––1.0––1.01.31.3–1.0
––––––92 x 67 x834399 x 98 x––8441––––77378431692798904715––9050––––76448476––8671––––––99 x 94 x––9999100 1007537––––10096
–––1.4 x1.91.0 x–2.0––2.12.72.61.13.0–1.8––1.71.1–1.2–––1.0 x–1.01.02.0––1.0
––––121–11––81513712–4––33––6–––––2310––2
––––221–16––1623211220–11––46––7–––––2517––2
––––1.91.6–1.5––1.91.51.61.71.7–2.4––1.4––1.1–––––1.31.71.7––0.9
–––46 x3241 x–53–––40 x55–––51––3852–62–––––31–44––26
–––37 x4032 x–40–––37 x52–––49––3156–67–––––36–42––21
–––1.3 x0.81.3 x–1.3–––1.1 x1.0–––1.0––1.20.9–0.9–––––0.9–1.1––1.3
––––5396–82––––8393––92–––99–92–––97––9881––93
––––3593–70––––5792––86–––97–78–––98––9872––92
––––1.51.0–1.2––––1.51.0––1.1–––1.0–1.2–––1.0––1.01.1––1.0
––––4217–34––3224227238–37––3316 y–4–––61––2457––23–––4426––––4056–43 y19–338––––3831–43
––––3712–22––141384726–21––146y–1–––58––2145––18–––3615––––1939–32 y12–122––––2129–32
––––1.21.5–1.5––2.21.92.81.51.4–1.8––2.42.5 y–4.4–––1.0––1.11.3––1.3–––1.21.8––––2.11.5–1.4 y1.5–2.74.7––––1.81.1–1.4
–1001003368961001899968934498524–801001005467–76100100–82100989727–10094
–10010030659310079797731198010–621001002136–6698100–84100979832–10093
–1.01.01.11.01.01.02.61.01.01.23.15.41.12.4–1.31.01.02.61.9–1.21.01.0–1.01.01.01.00.8–1.01.02.31.2–1.66.31.0––1.01.50.91.01.01.41.01.65.61.01.3––2.01.11.69.5
68––463y––––78––9277–9642––––999980 y28
86 3882 71100–40 2525497 96––––100 10015 1051 5796 95100 9645 32100 10083 5350993 9090 68––100–64 3296 8683 52384
Statistical tables
135
TABLE 3: HEALTH – RESIDENCE12: EQUITYBirth registration (%)2000–2010*ratio ofurbanurban rural to ruralUnder-fives withComprehensivediarrhoea receivingUnderweight% of populationknowledge of HIV (%)oral rehydration andprevalence inusing improvedSkilled attendantPrimary school netchildren under five (%) continued feeding (%)sanitation facilitiesat birth (%)attendance ratiofemales 15–242006–2010*2006–2010*2006–2010*2005–2010*2005–2010*2008ratio ofratio ofratio ofratio ofratio ofratio ofurbanurbanurbanurbanruralurbanurban rural to rural urban rural to urban urban rural to rural urban rural to rural urban rural to rural urban rural to rural
Countries and territories
MyanmarNamibiaNauruNepalNetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupied Palestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent and the GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogo
9483–42––9071 y49––97 y–32–––––87––––98––79–––62–76–7599–59–––706–––97–9838––9685100955093
6459–34––7325 y22––96 y–24–––––78––––98––83–––44–74–4499–48–––812–––98–9528––959099935771
1.51.4–1.2––1.22.9 y2.2––1.0 y–1.3–––––1.1––––1.0––0.9–––1.4–1.0–1.71.0–1.2–––0.93.7–––1.0–1.01.4––1.00.91.01.00.91.3
82589473––5114––––925678256528––––9997––6030––99848847––95647848––––––––100 x 99 x100 x 98 x––8267––––––9478––8975––85 x 33 x9999––6733––––––9067651594 x 85 x––––9999––95828980––––99939586100 10098 x599398 x2040
EM28BAFebr RGua Ory ED2012
1.41.3–3.5––1.73.12.4––1.0–2.0–1.21.9–1.51.6––––1.0 x1.0 x–1.2––
–1.2–1.2–2.5 x1.0–2.0–––1.34.51.1 x––1.0–1.21.1––1.11.11.01.0 x2.92.3
1912–23––4–16––––29 x––12 x–2–––––2x3x–6–––––12–7x1x–16–––82010 x––––74––912513510
2419–41––7–27––––33 x––20 x–8–––––4x4x–12–––––14–17 x1x–23–––12389x––––86––916824720
1.31.7–1.8––1.7–1.7––––1.1 x––1.6 x–3.8–––––2.0 x1.3 x–1.9–––––1.1–2.4 x1.1 x–1.5–––1.51.90.9 x––––1.11.5––1.01.31.71.01.41.9
–52–39––51 x4734––––38––––6664––––43 x––30 x–––––64–44 x76 x–59––––9–––––2619––3328 x4261 x5923
–45–37––47 x3222––––36––––5356––––56 x––23 x–––––62–42 x64 x–56––––6–––––2923––3520 x4823 x6424
–1.1–1.1––1.1 x1.51.6––––1.0––––1.21.1––––0.8 x––1.3 x–––––1.0–1.1 x1.2 x–1.1––––1.5–––––0.90.8––0.91.4 x0.92.7 x0.90.9
9394–90–––7178––––78–––8997––––––––––––89 y–86––98–78–––72 y30–––––9687––8997 y98937994
8991–83–––3256––––62–––8794––––––––––––88 y–85––99–56–––65 y9–––––9184––8597 y98977086
1.01.0–1.1–––2.21.4––––1.3–––1.01.0––––––––––––1.0 y–1.0––1.0–1.4–––1.1 y3.3–––––1.11.0––1.01.0 y1.01.01.11.1
–65–43–––3130––––––––––23–––––––63–––5–47–2747–28–––347–––––4570––7–43331417
–65–25–––818––––––––––17–––––––48–––2–38–1237–9–––282–––––3255––7–47181213
–1.0–1.7–––3.81.7––––––––––1.4–––––––1.3–––2.4–1.3–2.41.3–3.1–––1.24.1–––––1.41.3––1.0–0.91.81.21.4
86605051100–633436100100919772967571908180961001001008588935096––100–3010069969724100100100985284–10088–9061100100969595927624
7917–27100–3742810010084–29–5141403669801001001007454705596–96100–19–3888–6–99100–665–10092–665310010095949682403
1.13.5–1.91.0–1.78.51.31.01.01.1–2.5–1.51.72.32.31.21.21.01.01.01.11.61.30.91.0––1.0–1.6–1.81.1–4.0–1.01.0–8.71.3–1.01.0–1.41.21.01.01.01.01.01.11.98.0
136
THE STATE OF THE WORLD’S CHILDREN 2012
Countries and territories
Birth registration (%)2000–2010*ratio ofurbanurban rural to rural
Under-fives withComprehensivediarrhoea receivingUnderweight% of populationknowledge of HIV (%)oral rehydration andprevalence inusing improvedSkilled attendantPrimary school netchildren under five (%) continued feeding (%)sanitation facilitiesat birth (%)attendance ratiofemales 15–242006–2010*2006–2010*2006–2010*2005–2010*2005–2010*2008ratio ofratio ofratio ofratio ofratio ofratio ofurbanurbanurbanurbanruralurbanurban rural to rural urban rural to urban urban rural to rural urban rural to rural urban rural to rural urban rural to rural
MEMORANDUMSudan and South Sudanδ5322
EM28BAFebr RGua Ory ED20122.4–––21301.4––––––1.71.81.71.71.31.6 **1.61.3 **–1.0–1.6 **1.71.6 **79767875898371959698–84748543404140655840877492–5539551.81.91.91.91.41.41.81.11.31.1–1.51.91.513151215831 **33–3––17 **1917 **212217251343 **45–8––32 **2732 **1.61.51.51.71.61.4 **1.4–2.7––1.9 **1.41.9 **384149383744 **4056 **–––42 **4942 **343541313638 **3555 **–––37 **4537 **1.11.21.21.21.01.2 **1.21.0 **–––1.1 **1.11.1 **8381857992––98 **–91––84–6866765781––96 **–91––73–1.21.21.11.41.1––1.0 **–1.0––1.2–
TongaTrinidad and TobagoTunisiaTurkeyTurkmenistanTuvaluUgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republic of TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela (Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
–––95966024100––44––10039–94382857
–––92953821100––10––10023–8616930
–––1.01.01.61.11.0––4.6––1.01.7–1.12.33.21.9
––9896100–8099––83––10087–98628386
––898099–3798––40––10072–85263158
––1.11.21.0–2.21.0––2.0––1.01.2–1.22.32.71.5
–––17x–11–––11––4––––138
–––39x–17–––17––4––––1510
–––2.11.2 x–1.6–––1.5––0.9––––1.21.3
––612231–48–––55–––45––505946
––632222–39–––49–––43––475531
––1.01.01.4–1.2–––1.1–––1.1––1.11.11.5
–––94 y––8871––91––9785–95839194 y
–––91 y––8176––77––9580–96647790 y
–––1.0 y––1.10.9––1.2––1.01.1–1.01.31.21.0 y
––––7384848––55––3323–594y–––
––––4412837––45––3013–391y–––
––––2.00.91.71.3––1.2––1.11.8–1.56.7 y–––
98 9692 9296 6497 7599 9788 8138 4997 9098 95100 10032 21100 99100 99100 10066 48––94 6794 3359 4356 375518
1.01.01.51.31.01.10.81.11.01.01.51.01.01.01.4–1.42.81.41.53.1
SUMMARY INDICATORS#AfricaSub-Saharan AfricaEastern and Southern AfricaWest and Central AfricaMiddle East and North AfricaAsiaSouth AsiaEast Asia and PacificLatin America and CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld605345578660 **5082 **–97–64 **4465 **
363027346638 **3166 **–96–40 **2640 **
29334728–31 **3326 **–––29 **33–
20222914–16 **1422 **–––17 **21–
1.4551.5441.6551.935–901.9 ** 632.3571.2 ** 66–86–93–1001.7 ** 681.650–76
3224282166402655558298403145
1.71.82.01.71.41.62.21.21.61.11.01.71.61.7
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Birth registration– Percentage of children less than 5 years old who were registered at the moment ofthe survey. This includes children whose birth certificate was seen by the interviewer or whose mother orcaretaker says the birth has been registered.Skilled attendant at birth– Percentage of births attended by skilled health personnel (doctors, nurses ormidwives).Underweight– Percentage of children aged 0–59 months who are below minus two standard deviationsfrom median weight-for-age of the World Health Organization (WHO) Child Growth Standards.Under-fives with diarrhoea receiving oral rehydration and continued feeding– Percentage ofchildren (aged 0–4) with diarrhoea in the two weeks preceding the survey who received oral rehydrationtherapy (a packet of oral rehydration salts, recommended home-made fluids or increased fluids) andcontinued feeding.Primary school net attendance ratio– Number of children attending primary or secondary school who areof official primary school age, expressed as a percentage of the total number of children of official primaryschool age. Because of the inclusion of primary-school-aged children attending secondary school, thisindicator can also be referred to as a primary adjusted net attendance ratio.Comprehensive knowledge of HIV– Percentage of young women (aged 15–24) who correctly identify thetwo major ways of preventing the sexual transmission of HIV (using condoms and limiting sex to one faithful,uninfected partner), who reject the two most common local misconceptions about HIV transmission and whoknow that a healthy-looking person can be HIV-positive.% of population using improved sanitation facilities– Percentage of the population using any of thefollowing sanitation facilities, not shared with other households: flush or pour-flush latrine connected toa piped sewerage system, septic tank or pit latrine; ventilated improved pit latrine; pit latrine with a slab;covered pit; composting toilet.
MAIN DATA SOURCES
Birth registration– Demographic and Health Surveys (DHS), Multiple Indicator Cluster Surveys (MICS),other national surveys and vital registration systems.Skilled attendant at birth– DHS, MICS and other nationally representative sources.Underweight– DHS, MICS, other national household surveys, WHO and UNICEF.Diarrhoea treatment– DHS, MICS and other national household surveys.Primary school attendance– DHS, MICS and other national household surveys.Comprehensive knowledge of HIV– AIDS Indicator Surveys (AIS), DHS, MICS and other nationalhousehold surveys; HIV/AIDS Survey Indicators Database, <www.measuredhs.com/hivdata>.Use of improved sanitation facilities– UNICEF and WHO Joint Monitoring Programme for Water Supplyand Sanitation.– Data not available.x Data refer to years or periods other than those specified in the column heading. Such data are not includedin the calculation of regional and global averages.y Data differ from the standard definition and are included in the calculation of regional and global averages.* Data refer to the most recent year available during the period specified in the column heading.** Excludes China.Italicized dataare from different sources than the data presented for the same indicators in other tables of thereport: Table 2 (Nutrition – Underweight prevalence), Table 3 (Health – Diarrhoea treatment) and Table 8 (Women– Skilled attendant at birth).
NOTES
Statistical tables
137
TABLE 13: EQUITY – HOUSEHOLD WEALTHUnder-fives withComprehensiveComprehensivediarrhoea receivingUnderweightknowledge of HIV (%) knowledge of HIV (%)oral rehydration andprevalence inSkilled attendantPrimary school netchildren under five (%) continued feeding (%)at birth (%)attendance ratiofemales 15–24males 15–24Birth registration (%)2000–2010*2006–2010*2006–2010*2006–2010*2005–2010*2005–2010*2005–2010*ratio ofratio ofratio ofratio ofratio ofratio ofratio ofpoorest richest richest to poorest richest richest to poorest richest poorest poorest richest richest to poorest richest richest to poorest richest richest to poorest richest richest to20%20% to richest 20% 20% poorest 20% 20% poorest 20% 20% poorest 20% 20% poorest20%20% poorest20% poorestCountries and territories20%
Afghanistan–––––Albania98991.098 100Algeria–––8898Andorra–––––Angola17482.823 x 67 xAntigua and Barbuda–––––Argentina–––––Armenia93991.193 x 100 xAustralia–––––Austria–––––Azerbaijan92971.176 100Bahamas–––––Bahrain–––––Bangladesh6193.0957Barbados–––––Belarus–––100 x 100 xBelgium–––––Belize93981.1––Benin46751.65296Bhutan100 1001.03495Bolivia–––3899(Plurinational State of)Bosnia and Herzegovina 99 1001.099 100Botswana–––84 x 100 xBrazil–––––Brunei Darussalam–––––Bulgaria–––––Burkina Faso52901.75665Burundi58641.125 x 55 xCambodia59771.321 x 90 xCameroon51911.82398Canada–––––Cape Verde–––––Central African Republic 23833.72789Chad037 121.7861Chile–––––China–––––Colombia–––93 100Comoros72931.349 x 77 xCongo69 y 91 y1.3 y 40 x 95 xCook Islands–––––Costa Rica–––––Côte d'Ivoire28893.22995Croatia–––––Cuba–––––Cyprus–––––Czech Republic–––––Democratic People's–––––Republic of KoreaDemocratic Republic25271.15996of the Congo––Denmark–––Djibouti–––––Dominica–––––Dominican Republic59971.69599Ecuador–––99 x 98 xEgypt99 1001.05597El Salvador98991.09198Equatorial Guinea–––47 x 85 xEritrea–––7 x 81 xEstonia–––––Ethiopia3187.01 x 27 x
EM28BAFebr RGua Ory ED2012
–1.01.1–3.0 x––1.1 x––1.3––6.2–1.0 x––1.92.8
–85–––––––15––51–2x––2516
–42–––––––2––26–0x––107
–2.22.4–––––––7.0––1.9–6.7 x––2.42.2
––19––––53 x––27––57––––4061
––23––––78 x––28––70––––4760
––1.2––––1.5 x––1.0––1.2––––1.21.0
–8993–63–––––72––––96––3985
–9198–78–––––78––––94––6394
–1.01.1–1.2–––––1.1––––1.0––1.61.1
–205––––12––1––––31–2897546––––8262612––146––15–5––10–––––8–––31–2––––8
–6020––––29––12––––35–5526324049––––37356850––2318––32–12––24–––––24–––46–9––––39
–3.03.7––––2.5––10.3––––1.1–2.03.14.48.41.1––––4.41.32.64.0––1.62.9––2.2–2.4––2.5–––––2.8–––1.5–4.9––––4.7
–10–––––16––2–––––––17–11–––––––26–––19–––––12––15–––––––––21–9––––20
–38–––––20––14–––––––52–45–––––––64–––33–––––27––42–––––––––41–28––––50
–3.8–––––1.2––6.3–––––––3.0–4.3–––––––2.5–––1.7–––––2.3––2.8–––––––––2.0–3.1––––2.5
2.61.01.2 x–––1.22.2 x4.3 x4.4––3.37.6––1.11.6 x2.4 x––3.3–––––
82x16–––38––30––2533––6–16 x––21–––––
23x4–––18––5––1721––2–5x––6–––––
3.80.5 x4.0–––2.1––6.2––1.51.6––3.1–3.1 x––3.4–––––
2858––––3822 x56 x16––3914––4631 x36 x––44–––––
2747––––5327 x37 x45––5541––6434 x45 x––60–––––
0.90.8––––1.41.2 x0.7 x2.8––1.42.9––1.41.1 x1.3 x––1.4–––––
9599––––3359–50––31–––9025 x–––35–––––65–––82–81–––––
9798––––3969–87––48–––9339 x–––55–––––73–––91–93–––––
1.01.0––––1.21.2–1.7––1.5–––1.01.6 x–––1.6–––––1.1–––1.1–1.1–––––
1.6–––1.01.0 x1.81.11.8 x12.1 x–38.0 x
29–––––812 y–––36 x
12–––––51y–––25 x
2.3–––––1.412.9 y–––1.5 x
39–––54–21–33 x––10 x
38–––57–14–28 x––30 x
1.0–––1.0–0.7–0.9 x––3.1 x
138
THE STATE OF THE WORLD’S CHILDREN 2012
Under-fives withComprehensiveComprehensivediarrhoea receivingUnderweightknowledge of HIV (%) knowledge of HIV (%)oral rehydration andprevalence inSkilled attendantPrimary school netchildren under five (%) continued feeding (%)at birth (%)attendance ratiofemales 15–24males 15–24Birth registration (%)2000–2010*2006–2010*2006–2010*2006–2010*2005–2010*2005–2010*2005–2010*ratio ofratio ofratio ofratio ofratio ofratio ofratio ofpoorest richest richest to poorest richest richest to poorest richest poorest poorest richest richest to poorest richest richest to poorest richest richest to poorest richest richest to20%20% to richest 20% 20% poorest 20% 20% poorest 20% 20% poorest 20% 20% poorest20%20% poorest20% poorestCountries and territories20%
FijiFinlandFranceGabonGambiaGeorgiaGermanyGhanaGreeceGrenadaGuatemalaGuineaGuinea-BissauGuyanaHaitiHoly SeeHondurasHungaryIcelandIndiaIndonesiaIran (Islamic Republic of)IraqIrelandIsraelItalyJamaicaJapanJordanKazakhstanKenyaKiribatiKuwaitKyrgyzstanLao People'sDemocratic RepublicLatviaLebanonLesothoLiberiaLibyaLiechtensteinLithuaniaLuxembourgMadagascarMalawiMalaysiaMaldivesMaliMaltaMarshall IslandsMauritaniaMauritiusMexicoMicronesia(Federated States of)MonacoMongoliaMontenegroMoroccoMozambique
EM28BAFebr RGua Ory ED20123––3526––––2243–8935–6821––81––9081––––9077–9986–9995––27.1––2.63.2––––4.11.8–1.12.5–1.54.6––38––1821––––40 x––2431–––––14––913––––24 x––1117–––––2.7––1.91.6––––1.7 x––2.31.8––––––––4940––––4624––32––25–––––5256––––6534––51––37–––––1.11.4––––1.41.4––1.6––1.5––59––8315––––5971–8237––41––––9192777284––9456––––9690–8256––59––1.4––1.13.7––––1.61.3–1.01.5––1.5––––1.11.11.21.1––––98 x 100 x98 10030 x 95 x3789––1.0 x1.03.2 x2.4––7x4x15 x24––3x1x3x8––2.8 x4.1 x4.5 x3.1––47 x–37 x41––––50 x55––––1.3 x1.3––961009580
–––885289–60–––21178772–92––2423––––––––9948––9462––421y––––61––9265–9228––––9994–20
–––926498–88–––83359892–96––7284––––––––10080––9585––497y––––93––9496–9883––––9899–48
–––1.01.21.1–1.5–––4.02.01.11.3–1.0––3.13.7––––––––1.01.7––1.0
––––––––288995 x 99 x––2294––––––265719796493668––3399––––19896586––––––––––––––98 100100 1002081––––93 100
––––3.11.0 x–4.2–––2.24.01.510.5–2.9––4.61.3–––––––1.01.04.0––1.1
––––24––19––21 y24221622–16––57––––––––3525––2
––––9––9––3y191146–2––20––––––––029––2
––––2.6––2.2––6.5 y1.32.13.83.6–8.1––2.9––––––––26.02.82.8––0.8
–––37 x34––34–––32 x62–––45––2955–––––––32–49––49
–––45 x33––57–––45 x62–––52––4548–––––––35–41––20
–––1.2 x1.0––1.7–––1.4 x1.0–––1.1––1.50.9–––––––1.1–0.8––0.4
––––2890–60––––5289––80––––––––––––9958––94
––––4296–88––––6592––90––––––––––––9878––91
––––1.51.1–1.5––––1.21.0––1.1––––––––––––1.01.3––1.0
––––327–17––51063718–13––43y––––––––1829––17–––2614––––1033–23 y9–120––––1823–41
––––4519–34––4127257241–44––4523 y––––––––2861––29–––4829––––4252–48 y19–3912––––4436–43
––––1.42.8–2.1––7.82.84.32.02.2–3.4––11.77.5 y––––––––1.62.1––1.7–––1.82.1––––4.31.6–2.0 y2.0–3.329.5––––2.41.6–1.1
–––––––23–––8–2528––––152y–––––––––42––––––1417––––834––––374–––––––16
–––––––50–––28–6552––––5527 y–––––––––68––––––4537––––4945––––5827–––––––45
–––––––2.1–––3.3–2.61.9––––3.812.2 y–––––––––1.6––––––3.32.2––––6.51.3––––1.66.2–––––––2.7
1.4––1.26.1 y––––1.5––1.01.5–1.12.9––––1.01.0–2.4
Statistical tables
139
TABLE 3: HEALTH – HOUSEHOLD WEALTHTABLE 13: EQUITYUnder-fives withComprehensiveComprehensivediarrhoea receivingUnderweightknowledge of HIV (%) knowledge of HIV (%)oral rehydration andprevalence inSkilled attendantPrimary school netchildren under five (%) continued feeding (%)at birth (%)attendance ratiofemales 15–24males 15–24Birth registration (%)2000–2010*2006–2010*2006–2010*2006–2010*2005–2010*2005–2010*2005–2010*ratio ofratio ofratio ofratio ofratio ofratio ofratio ofpoorest richest richest to poorest richest richest to poorest richest poorest poorest richest richest to poorest richest richest to poorest richest richest to poorest richest richest to20%20% to richest 20% 20% poorest 20% 20% poorest 20% 20% poorest 20% 20% poorest20%20% poorest20% poorestCountries and territories20%
MyanmarNamibiaNauruNepalNetherlandsNew ZealandNicaraguaNigerNigeriaNiueNorwayOccupiedPalestinian TerritoryOmanPakistanPalauPanamaPapua New GuineaParaguayPeruPhilippinesPolandPortugalQatarRepublic of KoreaRepublic of MoldovaRomaniaRussian FederationRwandaSaint Kitts and NevisSaint LuciaSaint Vincent andthe GrenadinesSamoaSan MarinoSao Tome and PrincipeSaudi ArabiaSenegalSerbiaSeychellesSierra LeoneSingaporeSlovakiaSloveniaSolomon IslandsSomaliaSouth AfricaSouth SudanδSpainSri LankaSudanδSurinameSwazilandSwedenSwitzerlandSyrian Arab RepublicTajikistanThailandThe former YugoslavRepublic of MacedoniaTimor-LesteTogo
50467122––6320 y9––––18––––––––––97––82–––31–74–3198–43–––801–––97–9418––928999895063
96928847––9367 y62––––38––––––––––98––81–––63–86–8199–62–––787–––98–9850––9986100995696
1.92.01.22.2––1.53.3 y7.0––––2.1––––––––––1.0––1.0–––2.1–1.1–2.61.0–1.4–––1.06.6–––1.0–1.02.8––1.11.01.01.11.11.5
–60975––42218––
–989858––997186––
–1.61.012.0––2.43.310.3––1.0–4.8––––1.83.7––––1.0 x––1.7–––1.4–1.3–4.4 x1.0–2.5–––1.67.2–––1.0–1.21.4––1.31.01.1
3322747––9–35–––––––––9–––––5x–––––
147319––1–10–––––––––1–––––1x–––––
2.53.12.72.5––6.6–3.5–––––––––15.7–––––8.2 x––––––––2.6–4.2 x3.5 x–1.8–––1.43.0–––2.6–1.82.3––1.51.33.35.31.42.5
–32–25––44 x3117––––32––––5259––––43 x––21 x–––––66–40 x63 x–47––––5–––––2321––3720 x4320 x6619
–47–57––63 x4641––––45––––7565––––51 x––31 x–––––64–44 x––60––––11–––––3115––3826 x45–6227
–1.5–2.2––1.4 x1.52.5––––1.4––––1.51.1––––1.2 x––1.5 x–––––1.0–1.1 x––1.3––––2.2–––––1.40.7––1.01.3 x1.1–0.91.4
8188–76–––2631––––42––––92–––––––––––
9497–84–––3272––––74––––97–––––––––––
1.21.1–1.1–––1.22.4––––1.8––––1.1–––––––––––
–6113 y12–––59––––––––––14–––––––42––
–6910 y49–––3034––––––––––26–––––––59–––3–56–3248–31–––378–––––5472––10–43451617
–1.10.8 y4.3–––6.53.6––––––––––1.8–––––––1.4–––1.0–2.0–3.61.9–5.3–––2.113.5–––––2.41.5––2.9–0.95.01.81.6
–55–30–––618––––––––––––––––––50–––3–39–7––10–––35–––––––44––––––11–
–6725 y59–––3441––––––––––––––––––55–––9–55–36––42–––50–––––––64––––––35–
–1.2–2.0–––5.82.2––––––––––––––––––1.1–––2.7–1.4–5.1––4.2–––1.5–––––––1.5––––––3.0–
140
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012––6695––7493––20 x 89 x98 100––2871––––––56881177––––––9799––81966594––––7899909093 100–––18–21 x4x–22–––1442–––29–98––10171134921–––7–5x1x–12–––1014–––11–54––71330359––85 y 91 y––7595––––96 100––4483––––––58 y 61 y340––––––––––88977791––––––96 y 96 y97988660801008392–1.1 y–1.3––1.0–1.9–––1.1 y12.5–––––1.11.2–––1.0 y1.01.21.41.295 x 100 x106930971.0 x6.93.3
98 100––1677––––––––56 1002694––––––––99 x 100 x––––4371––––
–3–27–925–6–––171–––––2349––4–479911
Under-fives withComprehensiveComprehensivediarrhoea receivingUnderweightknowledge of HIV (%) knowledge of HIV (%)oral rehydration andprevalence inSkilled attendantPrimary school netchildren under five (%) continued feeding (%)at birth (%)attendance ratiofemales 15–24males 15–24Birth registration (%)2000–2010*2006–2010*2006–2010*2006–2010*2005–2010*2005–2010*2005–2010*ratio ofratio ofratio ofratio ofratio ofratio ofratio ofpoorest richest richest to poorest richest richest to poorest richest poorest poorest richest richest to poorest richest richest to poorest richest richest to poorest richest richest to20%20% to richest 20% 20% poorest 20% 20% poorest 20% 20% poorest 20% 20% poorest20%20% poorest20% poorestCountries and territories20%
MEMORANDUMSudan and South Sudanδ686
14.0
EM28BAFebr RGua Ory ED2012
TongaTrinidad and TobagoTunisiaTurkeyTurkmenistanTuvaluUgandaUkraineUnited Arab EmiratesUnited KingdomUnited Republicof TanzaniaUnited StatesUruguayUzbekistanVanuatuVenezuela(Bolivarian Republic of)Viet NamYemenZambiaZimbabwe
–94–89943917100––4––1001387725523
–98–99977126100––56––100419597503168
–1.0–1.11.01.81.51.0––12.7––1.03.11.11.39.35.82.9
–98–7399992897––31––1005595 x5317273915
–100–100100987699––90––1009092 x9974919290
–1.0–1.41.01.02.71.0––2.9––1.01.61.0 x1.94.33.42.45.8
–––48x121–––22––5––––16–
–––12x08–––9––3––––11–
–––8.43.2 x–2.5–––2.3––1.5––––1.5–
–––2027–39–––45–––38––415327
–––3336–44–––59–––53––546548
–––1.71.3–1.1–––1.3–––1.4––1.31.21.8
–95–87 y––7278––68––947486 x94447385 y19 y
–99–95 y––8275––93––967699 x96739697 y56 y
–1.0–1.1 y––1.11.0––1.4––1.01.01.2 x1.01.61.31.1 y2.9 y
–48––334 y2033––39––259–290y–––
–62––8394745––55––3323–614y–––
–1.3––2.81.2 y2.31.4––1.4––1.32.7–2.1––––
––––––2828––34––––––––––
–––––67 y4742––56––––––––––
––––––1.61.5––1.7––––––––––
31
17
1.9
53
59
1.1
SUMMARY INDICATORS#AfricaSub-Saharan AfricaEastern andSouthern AfricaWest and Central AfricaMiddle East andNorth AfricaAsiaSouth AsiaEast Asia and PacificLatin Americaand CaribbeanCEE/CISIndustrialized countriesDeveloping countriesLeast developed countriesWorld2823212561584764
2.22.52.22.5
30272926
87858486
2.93.22.83.3
2628–31
1011–11
2.52.6–2.7
32334127
44474944
1.41.41.21.6
54506542
77748469
1.41.51.31.7
14152310
34374730
2.52.42.03.2
20222816
44475340
2.22.11.92.4–3.9 **3.7––––3.2 **––
––27 ** 68 **226346 ** 89 **–94–31 **2232 **–98–67 **4967 **
–2.5 **2.81.9 **
4726 **1954 **
9286 **8492 **
1.9––3.3 ** 53 ** 20 **4.555201.7 ** ––
–33352.7 ** 36 ** 48 **2.7324754 ** 53 **
1.1611.3 ** –1.5–1.0 ** –
81–––
1.3–––
–––––7 ** 42 ** 5.6 ** 13 ** 51 **44511.1155516 ** 34 ** 2.2 ** ––––––––10 ** 38 **153610 ** 38 **–––––––––3.9 ** 15 ** 49 **2.4––3.8 ** ––
–1.0–2.2 **2.32.1 **
–88–31 **2932 **
–99–87 **7987 **
–––1.1–––––2.8 ** 39 ** 14 **2.732152.7 ** 39 ** 14 **
–––––––––2.7 ** 35 ** 47 **2.142532.7 ** 35 ** 47 **
–––88––1.3 ** –1.3571.3 ** –
–93––75–
–1.1––1.3–
# For a complete list of countries and territories in the regions, subregions and country categories, see page 124.δBecause of the cession in July 2011 of the Republic of South Sudan by the Republic of the Sudan, and its subsequent admission to the United Nations on 14 July 2011, disaggregated data for the Sudan and South Sudan as separate States arenot yet available for most indicators. Aggregated data presented are for the Sudan pre-cession (see Memorandum item).
DEFINITIONS OF THE INDICATORS
Birth registration– Percentage of children less than 5 years old who were registered at the moment of thesurvey. The numerator of this indicator includes children whose birth certificate was seen by the intervieweror whose mother or caretaker says the birth has been registered.Skilled attendant at birth– Percentage of births attended by skilled health personnel (doctors, nursesormidwives).Underweight– Percentage of children aged 0–59 months who are below minus two standard deviationsfrom median weight-for-age of the World Health Organization (WHO) Child Growth Standards.Under-fives with diarrhoea receiving oral rehydration and continued feeding– Percentage ofchildren (aged 0–4) with diarrhoea in the two weeks preceding the survey who received oral rehydrationtherapy (a packet of oral rehydration salts, recommended home-made fluids or increased fluids) andcontinuedfeeding.Primary school net attendance ratio– Number of children attending primary or secondary school whoare of official primary school age, expressed as a percentage of the total number of children of officialprimary school age. Because of the inclusion of primary-school-aged children attending secondary school,thisindicator can also be referred to as a primary adjusted net attendance ratio.Comprehensive knowledge of HIV– Percentage of young men and women (aged 15–24) who correctlyidentify the two major ways of preventing the sexual transmission of HIV (using condoms and limitingsex to one faithful, uninfected partner), who reject the two most common local misconceptions about HIVtransmission and who know that a healthy-looking person can be HIV-positive.
MAIN DATA SOURCES
Birth registration– Demographic and Health Surveys (DHS), Multiple Indicator Cluster Surveys (MICS),other national surveys and vital registration systems.Skilled attendant at birth– DHS, MICS and other nationally representative sources.Underweight– DHS, MICS, other national household surveys, WHO and UNICEF.Diarrhoea treatment– DHS, MICS and other national household surveys.Primary school attendance– DHS, MICS and other national household surveys.Comprehensive knowledge of HIV– AIDS Indicator Surveys (AIS), DHS, MICS and other nationalhousehold surveys; HIV/AIDS Survey Indicators Database, <www.measuredhs.com/hivdata>.– Data not available.x Data refer to years or periods other than those specified in the column heading. Such data are not includedin the calculation of regional and global averages.y Data differ from the standard definition and are included in the calculation of regional and global averages.* Data refer to the most recent year available during the period specified in the column heading.** Excludes China.Italicized dataare from different sources than the data presented for the same indicators in other tables of thereport: Table 2 (Nutrition – Underweight prevalence), Table 3 (Health – Diarrhoea treatment) and Table8 (Women– Skilled attendant at birth).
NOTES
Statistical tables
141
ABBREVIATIONSAIDSAPHRCBCGCBOCEDAWCFCCFCICSODHSDPTGDPGISGNIHIVICDDR,BICTIGMEIIEDILOJMPMDGMICSNFHSNGOOECDPAHOPPPSDIU5MRUNAIDSUNDESAUNDPUNESCOUNFPAUN-HabitatUNHCRUNICEFUNW-DPACUN-WomenUrban HEARTWHOacquired immune deficiency syndromeAfrican Population and Health Research Centeranti-tuberculosis vaccine (bacilli Calmette-Guérin)community-based organizationConvention on the Elimination of All Forms of Discrimination Against WomenChild-Friendly CitiesChild-Friendly Cities Initiativecivil society organizationDemographic and Health Surveysdiphtheria, pertussis and tetanus vaccinegross domestic productgeographic information systemgross national incomeInternational Centre for Diarrhoeal Disease Research, Bangladeshinformation and communications technologyInter-agency Group for Child Mortality EstimationInternational Labour OrganizationMillennium Development GoalNational Family Health Surveyhuman immunodeficiency virus
International Institute for Environment and Development
WHO-UNICEF Joint Monitoring Programme for Water Supply and SanitationMultiple Indicator Cluster Surveysnon-governmental organization
Organisation for Economic Co-operation and DevelopmentPan American Health Organizationpurchasing power parityunder-five mortality rate
Shack/Slum Dwellers International
Joint United Nations Programme on HIV/AIDSUnited Nations Development Programme
United Nations, Department of Economic and Social Affairs
United Nations Educational, Scientific and Cultural OrganizationUnited Nations Population FundUnited Nations Human Settlements ProgrammeUnited Nations High Commissioner for RefugeesUnited Nations Children’s FundUN-Water Decade Programme on Advocacy and CommunicationUnited Nations Entity for Gender Equality and the Empowerment of WomenUrban Health Equity Assessment and Response ToolWorld Health Organization
142
THE STATE OF THE WORLD’S CHILDREN 2012
EM28BAFebr RGua Ory ED2012
UNICEF HeadquartersUNICEF House3 United Nations PlazaNew York, NY 10017, USA
UNICEF Regional Office for EuropePalais des NationsCH-1211 Geneva 10, Switzerland
UNICEF Central and Eastern Europe/Commonwealth of IndependentStates Regional OfficePalais des NationsCH-1211 Geneva 10, SwitzerlandUNICEF Eastern and Southern AfricaRegional OfficeP Box 44145.O.Nairobi 00100, KenyaUNICEF West and Central AfricaRegional OfficeP Box 29720 Yoff.O.Dakar, Senegal
EM28BAFebr RGua Ory ED2012
UNICEF The Americas and CaribbeanRegional OfficeClayton Edificio 102Avenida MorseCiudad del SaberApartado Postal 0843-03045Panama City, PanamaUNICEF East Asia and the PacificRegional OfficeP Box 2-154.O.19 Phra Atit RoadBangkok 10200, ThailandUNICEF Middle East and North AfricaRegional OfficeP Box 1551.O.Amman 11821, JordanUNICEF South Asia Regional OfficeP Box 5815.O.Lekhnath MargKathmandu, Nepal
United Nations Children’s Fund3 United Nations PlazaNew York, NY 10017, USA[email protected]www.unicef.org
US$25.00ISBN: 978-92-806-4597-2eISBN: 978-92-806-4603-0United Nations publication sales no.: E.12.XX.1
� United Nations Children’s Fund (UNICEF)February 2012
EM28BAFebr RGua Ory ED2012� Jonas Bendiksen/Magnum Photos
For the online edition,scan this QR code or go towww.unicef.org/sowc2012