Udenrigsudvalget 2009-10
URU Alm.del Bilag 102
Offentligt
Joint Action for ResultsUNAIDS Outcome Framework2009–2011
UNAIDS/09.13E – JC1713E (English original, May 2009)Updated version July 2009� Joint United Nations Programme on HIV/AIDS (UNAIDS) 2009.All rights reserved. Publications produced by UNAIDS can be obtained from the UNAIDS Content ManagementTeam. Requests for permission to reproduce or translate UNAIDS publications—whether for sale or fornoncommercial distribution—should also be addressed to the Content Management Team at the address below,or by fax, at +41 22 791 4835, or e-mail: [email protected].The designations employed and the presentation of the material in this publication do not imply the expression ofany opinion whatsoever on the part of UNAIDS concerning the legal status of any country, territory, city or area orof its authorities, or concerning the delimitation of its frontiers or boundaries.The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed orrecommended by UNAIDS in preference to others of a similar nature that are not mentioned. Errors and omissionsexcepted, the names of proprietary products are distinguished by initial capital letters.All reasonable precautions have been taken by UNAIDS to verify the information contained in this publication.However, the published material is being distributed without warranty of any kind, either expressed or implied.The responsibility for the interpretation and use of the material lies with the reader. In no event shall UNAIDS beliable for damages arising from its use.Cover photo: UNAIDS
WHO Library Cataloguing-in-Publication DataJoint action for results: UNAIDS outcome framework, 2009–2011.“UNAIDS/09.13E / JC1713E”.1.HIV infections – prevention and control. 2.HIV infections – epidemiology. 3.Technical cooperation.4.Interinstitutional relations. I.UNAIDS.ISBN 978 92 9173 780 2(NLM classification: WC 503.6)
UNAIDS20 avenue AppiaCH-1211 Geneva 27Switzerland
T (+41) 22 791 36 66F (+41) 22 791 48 35
Joint Action for ResultsUNAIDS Outcome Framework, 2009–2011
Photo UNAIDS / P. Virot
“People forget.We are here to act.We are here to deliver results.We are agents ofchange. Our job is to change the UN – and,through it, the world.”Secretary-General Ban Ki-moonTurin, Italy
Photo UNAIDS / P. Virot
Photo UNAIDS / P. Virot
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
Photo UNAIDS / P. Virot
2Photo UNAIDS / P. Virot
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
ContextThe global response to the HIV epidemicis at a crossroads. The emergency footing ofthe response over the past 25 years and thebroad social mobilization of stakeholdershave spearheaded remarkable action andresults.Yet the hard-won gains are fragile andcall for a renewed commitment and leader-ship by the United Nations system. Ourjoint efforts have produced encouragingresults, but many challenges lie ahead.In order to achieve further progress, it isessential to take steps to address specific gapsin the response to the epidemic as well asthe social, political and structural constraintsthat limit results.Progress requires that the UNAIDSSecretariat, the Cosponsors1and otherpartners protect and build on the gainsalready made and make use of theopportunities for linking specific actionsand broader agendas for reaching theMillennium Development Goals.The challenges facing the response toAIDS are exacerbated by the current globalfinancial and economic crisis. As statedin the April 2009 communiqué from theSecretariat of the United Nations SystemChief Executives Board for Coordination,the crisis will affect all countries, with aserious and disproportionate impact on thepoorest, and could leave 80% of the world’spopulation without a social safety net.The HIV organizational landscape hasevolved and grown more complex overthe past decade. UNAIDS, donors and civilsociety, including networks of people livingwith HIV, have rightly demanded greaterclarity on the relationships between needs,financing, activities and outcomes. Alsodemanded is greater specificity about therole of UNAIDS and the Secretariat withinthe wider constellation of actors.We are responding through this OutcomeFramework to optimize our partnershipsbetween the UNAIDS Secretariat and theCosponsors. The Outcome Framework,which builds upon the UNAIDS StrategicFramework (2007–2011), will guide futureinvestment. It will also hold the Secretariatand the Cosponsors accountable for makingthe resources of the UN work for results inthe countries.
1
The ten UNAIDS cosponsoring organizations are: Office of the United Nations High Commissioner for Refugees (UNHCR), UnitedNations Children's Fund (UNICEF), World Food Programme (WFP), United Nations Development Programme (UNDP), United NationsPopulation Fund (UNFPA), United Nations Office on Drugs and Crime (UNODC), International Labour Organization (ILO), United NationsEducational, Scientific and Cultural Organization (UNESCO), World Health Organization (WHO), World Bank.
3
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
Keeping the momentumIn 2006, the world made a historic commit-ment at the United Nations aimed at thegoal of universal access to comprehensiveprevention programmes, treatment, careand support. The achievement of universalaccess will remain the fundamental priorityfor UNAIDS. Universal access goals canbecome a reality. By achieving these goals,we can contribute to the broader develop-ment agenda.The multisectoral determinants of theepidemic demand dynamic and multifacetedresponses that must constantly evolve tomeet emerging challenges and priorities. Wehave identified areas in which our collectiveaction can make a difference. Flexibility inplanning and budgeting is critical, as is theability to monitor progress and results.We will continue to strive for increased effi-ciency and effectiveness in the response toAIDS, and to demonstrate the added valueof coherence in the UN system and itscollective impact at the country level.We will revive the unified forces of theCosponsors and the implementation ofa relevant UN response to the epidemic.Delivering results in priority areas holds theCosponsors and the UNAIDS Secretariataccountable in each area of their respectivecomparative advantage.
Photo UNAIDS / J. Wainwright
4
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
Moving forwardUnder the Outcome Framework for theperiod 2009–2011, UNAIDS will continueto advocate for comprehensive nationalresponses, including ramped-up preventionefforts to break the trajectory of the epidemic,and will refocus its efforts on achieving resultsin nine priority areas. These priority areashave been selected because their realizationwill contribute directly to the achievementUnion and the Association of Southeast AsianNations, and coalitions such as Health 8.Substantial progress on a number of theMillennium Development Goals can beachieved by taking the AIDS response outof isolation and integrating it with effortsto achieve broader human developmentand the goals of health and social justice.
This Outcome Framework affirms the UNAIDS Secretariat andCosponsors to leverage our respective organizational mandates and resourcesto work collectively to deliver results.of universal access and will simultaneouslyenable advancement towards the relatedMillennium Development Goal outcomes.Our success demands a shift in the develop-ment agenda, in which poverty reduction isaccompanied by a growth in dignity, freedomand equality. In this model of develop-ment, women and men — including thosepushed to the margins of society — will haveenhanced control over their lives.The AIDS movement has used the powerof human rights to transform society’sapproach to the epidemic. The globalmovement of people living with HIV andthe nearly four million people on treatmentare a force for change.UNAIDS will fully engage partners andstakeholders from all sectors, including civilsociety, networks of people living with HIV,the private sector, governments, regionalintergovernmental groups such as the AfricanThe response to AIDS should be aboutbuilding bridges and restoring trust inpublic institutions.Future investments in the AIDS response willbe guided by:The commitment to stand by peopleliving with and affected by HIV;Measurable impacts on preventing newinfections and on the people mostaffected;The promotion of human rights andgender equality;The best available scientific evidence andtechnical knowledge;Comprehensive responses to AIDS thatintegrate HIV prevention, treatment, careand support;The pursuit of wider results in terms ofdevelopmental outcomes; andProgramme coherence and alignment ofexternal resources to national prioritiesto effectively deliver results.5
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
Action agenda:Nine priority areas and cross-cutting strategies
Photo UNAIDS
Under the Outcome Framework for theperiod 2009–2011, UNAIDS will focus itsefforts on achieving results in nine priorityareas. These priority areas have beenselected based on a series of consultationswith the Cosponsors, communities, civilsociety and a broad range of other stake-holders.The realization of these priority areaswill accelerate the achievement ofuniversal access. It will require effort andcommitment from all stakeholders, andcan bring about even greater results interms of wider developmental outcomesand contribute to the attainment of theMillennium Development Goals.In our continuous efforts to support allcountries to halt and reverse the epidemic,address its drivers and mount an effectiveresponse, major relevant strategies forcombination HIV prevention mustbe strengthened, brought to scale andextended to meet the particular needs of allthose at risk, including people on the moveand people in emergency settings.The priority areas are interlinked, andhence progress in one area will contributeto progress in others. In many cases, a single6
programmatic activity can promote actionin more than one of the priority areas.We can reduce sexual transmissionof HIV:Sexual transmission accounts formore than 80% of new HIV infectionsworldwide. Reversing the global AIDSepidemic requires a dramatic increase incommunity, national and global actionfor sexual and reproductive health andrights, and in individual commitmentto safer sex. We can reduce sexualtransmission of HIV by promoting socialnorms and individual behaviours thatresult in sexual health; by supporting theleadership of people living with HIV for‘positive health, dignity and prevention’;and by supporting universal access to keyprevention commodities and services,especially for the most vulnerable,including sex workers and men whohave sex with men.We can prevent mothers fromdying and babies from becominginfected with HIV:By scaling upaccess to and the use of quality servicesfor the prevention of mother-to-childtransmission (+) as an integral part ofsexual and reproductive health servicesand reproductive rights for women, theirpartners and young people. This includes
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
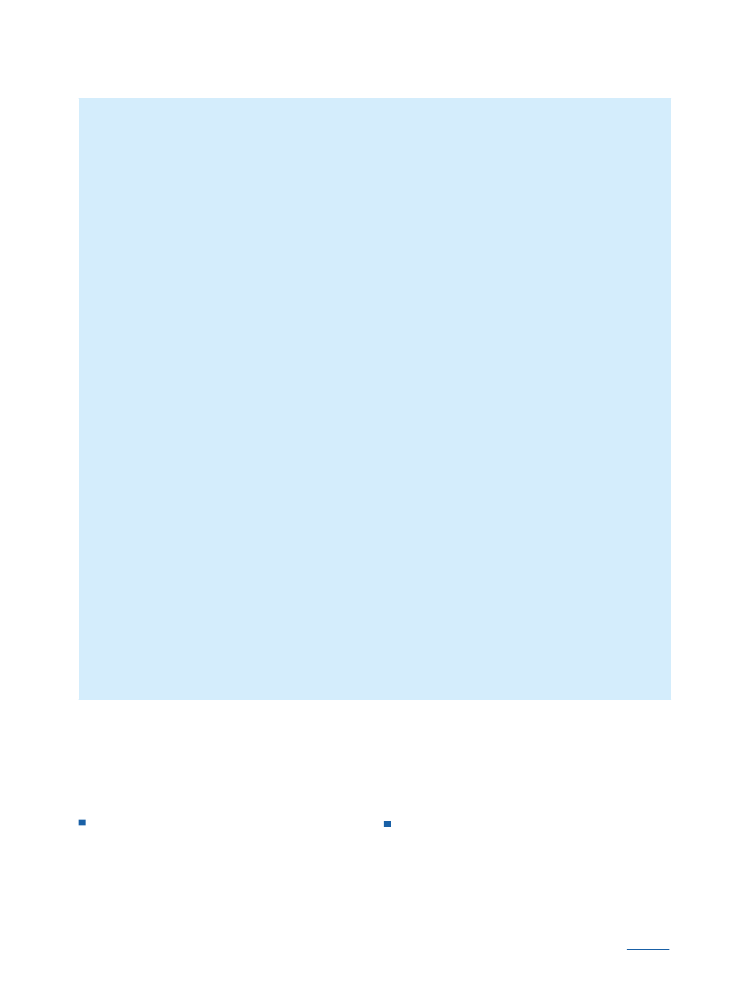
HIV prevention key to changing the trajectory of the AIDS epidemicFor every two people who start on HIV treatment, five are newly infected. UNAIDS mustmagnify its focus on HIV prevention while addressing the specific needs of each keypopulation, including youth, women and girls, sex workers and their clients, injectingdrug users, men who have sex with men, prisoners, refugees and migrants. This will helpchange the course of the epidemic.UNAIDS advocates for a combination approach to HIV prevention that is tailored tolocal epidemics. Combination prevention requires action simultaneously both on theimmediate risks and on the underlying drivers of the epidemic.Combination HIV prevention involves choosing the right mix of HIV prevention actionsand tactics to suit the unique epidemic in each country and matching the needs of thosemost at risk, just as the right combination of drugs and nutritional support is chosen forantiretroviral treatment.Combination HIV prevention means providing services and programmes for individuals,such as promoting the knowledge and skills necessary to undertake safe behaviours.These include knowledge of HIV status, knowledge of risks, reducing concurrent andserial sexual partners, using condoms consistently, scaling-up male circumcision and theprevention of mother-to-child transmission services. Combination HIV prevention needsinvestment in structural interventions, including legal reforms to outlaw discriminationagainst people living with HIV and the enforcement of laws that prohibit sexual andgender-based violence. It also requires the promotion of a desire for behaviour changewhile simultaneously acting to shift community norms and broader social environments.Only in this way can HIV prevention responses be widespread and sustainable.Combination prevention highlights the synergies that can come when these programmesare coordinated and reinforce each other.There is no single ‘magic bullet’ for HIV prevention, but by making the right choicesevery country's HIV prevention efforts can have the power, relevance and scale requiredto stop new HIV infections.
ongoing care and treatment for women,and their partners, and children inaffected families.We can ensure that people living withHIV receive treatment:By scaling upand sustaining treatment coverage andbridging the gap between sexual andreproductive health and HIV, integratingnutritional support within treatment
programmes and increasing the numberof skilled and equipped health workers.We can prevent people living withHIV from dying of tuberculosis:Byensuring an effective integrated deliveryof services for HIV and tuberculosis aswell as nutritional support in all settings.7
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
We can protect drug users frombecoming infected with HIV:Bymaking comprehensive, evidence-informed and human-rights-basedinterventions accessible to all drugusers (i.e. harm reduction and demandreduction), including programmes toreduce hepatitis coinfection, and byensuring that legal and policy frameworksserve HIV prevention efforts.We can remove punitive laws,policies, practices, stigma anddiscrimination that block effectiveresponses to AIDS:By collaboratingwith civil society and all stakeholders touphold non-discrimination in all efforts,countering social judgement and thefear that feeds stigma, delivering on thebroader human rights agenda, includingin the areas of sex work, travel restrictions,homophobia and criminalization of HIVtransmission, ensuring access to justiceand use of the law by promoting propertyand inheritance rights, protecting accessto and the retention of employment andprotecting marginalized groups and rein-forcing the work of UN Plus.We can stop violence againstwomen and girls:By making theresponse to AIDS an opportunity toreduce intimate partner and sexualviolence and developing comprehensiveresponses to gender-based violence andHIV prevention within and beyond thehealth sector.
We can empower young people toprotect themselves from HIV:Byputting young people’s leadership at thecentre of national responses, providingrights-based sexual and reproductivehealth education and services andempowering young people to preventsexual and other transmission of HIVinfection among their peers. By ensuringaccess to HIV testing and preventionefforts with and for young people in thecontext of sexuality education. And byensuring enabling legal environments,education and employment opportunitiesto reduce vulnerability to HIV.We can enhance social protection forpeople affected by HIV:By promotingthe provision of a range of social servicesto protect vulnerable populations,including populations of humanitarianconcern, refugees, internally displacedpersons and migrants, informal-economyworkers, people experiencing hunger,poor nutrition and food insecurity andorphaned and vulnerable children. Bypromoting corporate social responsibility,workplace policies and incomegeneration for people affected by HIV. Byempowering governments, particularlyministries of labour, employers andworkers to adopt, implement andmonitor HIV-related policies. Andby countering discrimination andpromoting HIV prevention, treatment,care and support through workplaces,including through UN Cares, and theirlinks with the community.
8
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
Photo UNAIDS / P. Virot
Cross-cutting strategiesThese outcome areas call for joint action. Inorder to address these areas effectively, theSecretariat and the Cosponsors will supportcross-cutting strategies and institutional deliverymechanisms that build on what we know worksand will take steps for change where we needto work differently and work better. We will:Bring AIDS planning and action intonational development policy and broaderaccountability frameworks;Optimize UN support for applications to,and programme implementation of, theGlobal Fund to Fight AIDS, Tuberculosisand Malaria;Improve country-by-country strategicinformation generation, analysis and use,including through the mobilization ofnovel sources;Assess and realign the management oftechnical assistance programmes;Develop shared messages for sustainedpolitical commitment, leadership develop-ment and advocacy; andBroaden and strengthen engagement withcommunities, civil society and networksof people living with HIV at all levels ofthe response.
9
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
Translating priority areas into measurableoutcomesThe ultimate impacts of the renewedcommitment to universal access reflected inthe Outcome Framework will be avertingHIV infections and HIV-related deaths andimproving the quality of life of people livingwith HIV. This is in line with the sixthMillennium Development Goal, to halt andreverse the AIDS epidemic.For each of the nine priority areas, aswell as the cross-cutting strategies, specificoutcomes and targets will be established inthe UNAIDS Unified Budget and Workplan(UBW).The UBW brings together the individualand joint efforts of the ten Cosponsorsand the UNAIDS Secretariat to opera-tionalize the Outcome Framework. Thespecific results and corresponding budgetsof the Cosponsors and the Secretariat willbe defined. Clear accountability indicatorswill be developed and used to track prog-ress and to monitor the achievement of theoutcomes and the action agenda.In supporting the implementation of theOutcome Framework, UNAIDS willincreasingly concentrate its human andfinancial resources where they can makethe most difference to the epidemic. Jointprogrammes of support will be scaled upsubstantially and will become the norm andnot the exception.UNAIDS country staff will increasinglyfocus their efforts on:Brokering and unifying the managementof relevant technical support for appro-priate national AIDS responses;Producing strategic analyses of program-matic quality to improve results-basedimplementation;Enabling political agents to demandchange in governance, legislation andpolicy to support evidence-informedprogrammes;Developing oversight structures toensure mutual accountability to demandresults; andSupporting the Cosponsors, in order tomaximize their comparative advantage atthe country level in support of nationalefforts to achieve universal access.
10
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
Measuring progress,promoting accountability, achieving the visionFollowing the historic G20 summit inMarch 2009, UN Secretary-General BanKi-moon made clear the importanceof turning the economic crisis into anopportunity for a sustainable future. TheUN system will actively participate in anew vulnerability monitoring and alertmechanism to track developments andreport on the political, economic, social andenvironmental dimensions of the crisis.Each of the nine priority areas representsa distinct goal. Each priority area requiresa strategic combination of specific actionsthat should be tailored to the country’sspecific epidemic and that must identify themost effective strategies, build local capacity,increase coverage of services, ensure qualityand ensure that services are equitable.If countries were to reach their 2010 targetsfor universal access, a dramatic change in thecourse of the epidemic would follow (seebox below).In order to establish baselines, measureprogress and monitor success or failure,multiple sources of data and methodologiesmust be used. No single indicator cancapture the entire scope of progress towardsany of these outcomes. We will use a mix ofrelevant quantitative indicators, compositeindices and specific qualitative assessments.We will synthesize this information intoa meaningful understanding of whether
If countries reached their 2010 targets for universal access*, this would dramaticallychange the course of the epidemic.Expected outcomes in 132 low- and middle-income countries (in millions)200720102015
Number of new HIV infections (annual)People on antiretroviral treatmentWorkers reached in the workplacePregnant women offered comprehensiveprevention of mother-to-child transmissionservicesMen who have sex with men reachedSafe injections providedOrphans supported
2.73.0
1.36.746.274.5
1.011.696.778.7
11.820.0
3.9
20.44 2476.7
23.35 74218.9
348.31.5
* Under the country-defined universal access approach countries achieve different programmatic targets at different times and the achieve-ment of universal access by all countries by 2015.
11
J O I N T AC T I O N F O R R E S U LT S
|
UNAIDS OUTCOME FRAMEWORK, 2009–2011
We can prevent mothers from dying and babies from becoming infectedwith HIV — how to measure progressTo know if a country has achieved this priority area, we need indicators to answerquestions such as:Have the most effective multiple drug combinations for preventing HIVtransmission (according to the latest guidelines), rather than the use of just onedrug (such as nevirapine), been utilized?Were mothers evaluated for initiation of full, ongoing antiretroviral treatment?Have other sexual and reproductive health services been provided (e.g.congenital syphilis screening and treatment)?Were other members of the family provided services, with siblings and spousesbeing tested, counselled and started on therapy as needed?Has counselling taken place on infant feeding and on the future use ofcontraception?Has there been an exploration of the possible social support services that may benecessary, such as for nutrition and education?
progress is truly being made and wherebottlenecks are impeding progress.By 2010, nearly US$ 25 billion (US$ 18.9billion–US$ 30.5 billion) will be neededannually for low- and middle-incomecountries. To assess access to funds, countrieswill be mapped based on the proportionof available funds from all sources (nationaland international) compared with theestimated resource needs and the number ofcountries with successful HIV-related grantapplications to the Global Fund to FightAIDS, Tuberculosis and Malaria. Countrieswill also be monitored according to thelevel of investment in the strengthening ofthe health sector and the number of health-
care workers available compared with theestimated needs.Each of the nine priority areas will bemonitored and assessed in the samecomprehensive way — outcome byoutcome and country by country. Thecommon dimensions of capacity, coverage,quality, equity and efficiency are neededto provide the framework for assessingthe impact in each country and to enablecomparability across countries.Ultimately, we are concerned with resultsfor people, whether and why our efforts areeffective at achieving measurable impactson new infections, life expectancy andquality of life.
12
UNAIDS is an innovative joint venture of the United Nations, bringing together the efforts and resourcesof the UNAIDS Secretariat and ten UN system organizations in the AIDS response. The Secretariat head-quarters is in Geneva, Switzerland—with staff on the ground in more than 80 countries. The Cosponsorsinclude UNHCR, UNICEF, WFP, UNDP, UNFPA, UNODC, ILO, UNESCO, WHO and the World Bank.Contributing to achieving global commitments to universal access to comprehensive interventions for HIVprevention, treatment, care and support is the number one priority for UNAIDS. Visit the UNAIDS websiteat www.unaids.org
UNAIDS20 AVENUE APPIACH-1211 GENEVA 27SWITZERLANDTel.: (+41) 22 791 36 66Fax: (+41) 22 791 48 35e-mail: [email protected]
www.unaids.org
Uniting the world againstAIDS