Sundhedsudvalget 2009-10
SUU Alm.del Bilag 517
Offentligt
World Alzheimer Report 2010The GlobAl economic impAcT of DemenTiA
Executive Summary
World Alzheimer reporT 2010
Alzheimer’s Disease InternationalWorld Alzheimer Report 2010The Global Economic Impact of Dementiaprof Anders Wimo, Karolinska institutet, stockholm, swedenprof martin prince, institute of psychiatry, King’s College london, UKpublished by Alzheimer’s disease international (Adi) 21 september 2010
Acknowledgementsprofessor Bengt Winblad (Karolinska institutet, stockholm, sweden) and dr linus Jönsson (i3 innovus and Karolinskainstitutet, stockholm, sweden) have contributed significantly to the methodological development in the cost estimates.swedish Brain power (sBp) provided unrestricted financial support for the work of Anders Wimo for this study.Alzheimer’s Association (Us) for support with reviewing and launching this report.photos: Cathy Greenblat – www.cathygreenblat.comdesign: Julian howell
ADI would like to thank those who contributed financially:Vradenburg FoundationGeoffrey Beene Foundation – www.geoffreybeene.com/alzheimers.htmlAlzheimer’s Association – www.alz.orgAlzheimer’s Australia – www.alzheimers.org.auAlzheimer’s Australia WA – www.alzheimers.asn.auAlzheimer scotland – www.alzscot.orgAlzheimer’s society – www.alzheimers.org.ukAssociation Alzheimer suisse – www.alz.chAlzheimerföreningen i sverige – www.alzheimerforeningen.sedeutsche Alzheimer Gesellschaft – www.deutsche-alzheimer.destichting Alzheimer nederland – www.alzheimer-nederland.nl
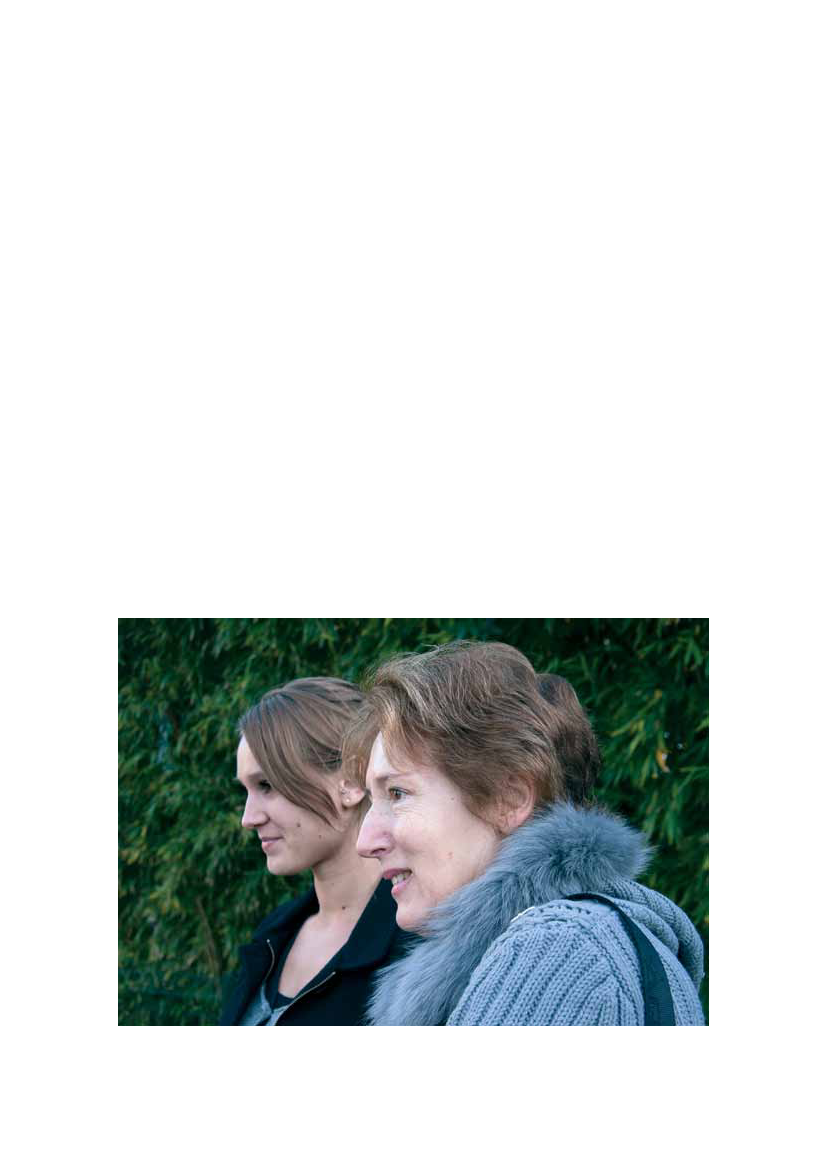
Cover imageAna de Jesus de Bido, a pastor and geriatrician, and her physicianhusband run a care facility in the Villa Francisca barrio in santo domingo,dominican republic. here she was on a home visit with 82-year-old Analuisa Candelario, who cares for her 92-year-old husband. Ana luisatakes little care of herself, often not eating, and pastor Ana consoled herand explained the importance of caregivers taking care of themselves.
Alzheimer’s diseAse inTernATionAl
The GloBAl eConomiC impACT oF demenTiA
1
ForewordIn the World Alzheimer Report 2010, we build upon the findings detailed in the World AlzheimerReport 2009, to explore the cost of dementia to our societies. The Report contains an explanationof the methods used, detailed results for different economic and geographic regions, and we offerconclusions and recommendations in the final section.As you will see, the figures are cause for great concern and we hope that this Report will act asa call to action for governments and policy makers across the world. It is vital that they recognizethat the cost of dementia will continue to increase at an alarming rate and we must work to improvecare and support services, treatment and research into dementia in all regions of the world. Lowerincome countries face a severe lack of recognition of dementia, placing a heavy burden on familiesand carers who often have no understanding of what is happening to their loved one. High incomecountries are struggling to cope with the demand for services, leaving many people with dementiaand caregivers with little or no support. Consequently, we urge key decision makers to take noticeof this very important document and to work with Alzheimer associations and with ADI to makedementia a national and global health priority.We would like to thank a number of people for their hard work on the development of this Report.We are grateful to the Report’s authors, Prof Anders Wimo and Prof Martin Prince, for their tirelessefforts and dedication, and Niles Frantz and MaryKate Wilson from the Alzheimer’s Association inthe USA for their valuable input. Thank you also to the sponsors who made the Report possibleand to those who took the time to review the contents: the Organisation for Economic Co-operation and Development (OECD) in Paris, the Alzheimer’s Association in the USA and GlennRees at Alzheimer’s Australia. Finally, we would like to thank Cathy Greenblat for her photographs.Daisy AcostaChairmanAlzheimer’s disease international
Marc Wortmannexecutive directorAlzheimer’s disease international
As mandakini became more confused, it was clear that she could no longer live alone. Two of her sons indicated thatthey could not take care of her because they had young children. her son satish and his wife neha, who also hadyoung children, brought her to their home, where they take care of her with the assistance of a professional caregiver.eight-year old srushti has found ways to relate to her grandmother, and her two-year-old sister shows no fear. Thoughmandakini speaks very little, srushti has found that her grandmother enjoys the religious chants that have beenimportant to her throughout her life. now srushti leads and they chant together.
Alzheimer’s diseAse inTernATionAl
2
World Alzheimer reporT 2010
Executive SummaryThe total estimated worldwide costs of dementia are US$604 billion in 2010.About 70% of the costs occur in Western Europe and North America.Costs were attributed to informal care (unpaid care provided by family and others), directcosts of social care (provided by community care professionals, and in residential homesettings) and the direct costs of medical care (the costs of treating dementia and otherconditions in primary and secondary care).Costs of informal care and the direct costs of social care generally contribute similarproportions of total costs, while the direct medical costs are much lower. However, in lowand middle income countries informal care accounts for the majority of total costs anddirect social care costs are negligible.
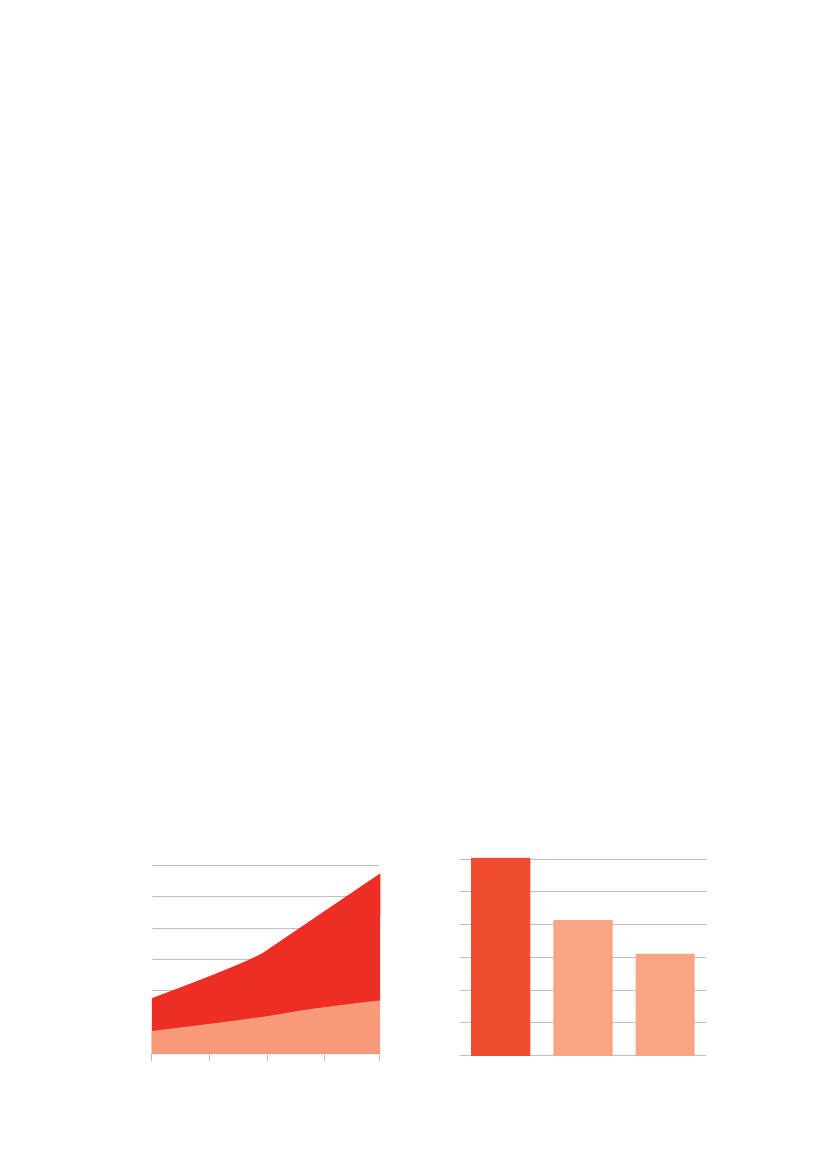
Background• Dementia is a syndrome that can be caused by a number of progressive disorders that affectmemory, thinking, behaviour and the ability to perform everyday activities. Alzheimer’s diseaseis the most common type of dementia. Other types include vascular dementia, dementia withLewy bodies and frontotemporal dementia.• Dementia mainly affects older people, although there is a growing awareness of cases that startbefore the age of 65. After age 65, the likelihood of developing dementia roughly doubles everyfive years.• In last year’s World Alzheimer Report, Alzheimer’s Disease International estimated that there are35.6 million people living with dementia worldwide in 2010, increasing to 65.7 million by 2030and 115.4 million by 2050. Nearly two-thirds live in low and middle income countries, where thesharpest increases in numbers are set to occur (figure 1).• People with dementia, their families and friends are affected on personal, emotional, financialand social levels. Lack of awareness is a global problem. A proper understanding of thesocietal costs of dementia, and how these impact upon families, health and social careservices and governments may help to address this problem.Figure 1The growth in numbers of people withdementia in high income countries and low andmiddle income countriesNumbers of people with dementia (millions)120100806040200201020202030YearAlzheimer’s diseAse inTernATionAl
Figure 2Cost of dementia compared to companyrevenue
US$ billions600500400
low and middleincome countries
3002001000
high income countries20402050
Dementia
Wal-Mart
Exxon Mobil
The GloBAl eConomiC impACT oF demenTiA
3
• The societal cost of dementia is already enormous. Dementia is already significantly affectingevery health and social care system in the world. The economic impact on families isinsufficiently appreciated.• In this World Alzheimer Report 2010, we merge the best available data and the most recentinsights regarding the worldwide economic cost of dementia. We highlight these economicimpacts by providing more detailed estimates than before, making use of recently availabledata that considerably strengthens the evidence base.– The World Alzheimer Report 2009 provides the most comprehensive, detailed and up-to-date data on the prevalence of dementia and the numbers of people affected in differentworld regions.– The 10/66 Dementia Research Group’s studies in Latin America, India and China haveprovided detailed information on informal care arrangements for people with dementia inthose regions.– For this Report, Alzheimer’s Disease International has conducted a global survey of keyinformants regarding the extent of use of care homes in different world regions.
When a caregiver in a Kyoto group home embraced this resident everyone around smiled. Although it is widely heldthat touching is not appropriate in Japanese culture, dr Yoshio miyake explained that ‘in Japan, training coursesfor professional caregivers of people with dementia take place in many and different settings, where non-verbalcommunication with them, including touch or physical contact, is emphasised very often.’
This document is the Executive Summary of the World Alzheimer Report 2010.The full Report, including detailed explanations of the methodology, results, conclusionsand references to sources, is available free from www.alz.co.uk/worldreport.
Alzheimer’s diseAse inTernATionAl
4
World Alzheimer reporT 2010
Methods• Different methods can be used to estimate the cost of an illness. The base approach in thisReport is a societal, prevalence-based gross cost of illness study. Annual costs per person withdementia for each country have been applied to the estimated number affected in that country,and then aggregated up to the level of World Health Organization regions, and World Bankincome groupings.• The costs considered include informal (family) care as well as direct medical and social carecosts. Direct medical costs refer to the medical care system, such as costs of hospital care,medication and visits to clinics. Direct social care costs are for formal services provided outsideof the medical care system, including community services such as home care, food supply andtransport, and residential or nursing home care.• For informal care, we estimated how much time family caregivers spend caring, includingtime spent with basic activities of daily living (such as eating, dressing, bathing, toileting andgrooming) and with instrumental activities of daily living (such as shopping, preparing food,using transport and managing personal finances).• The costs in this Report, as well as the prevalence of dementia, reflect estimates for 2010and are expressed as US dollars. To permit aggregation across countries, and comparisonsbetween countries and regions, costs were converted to US dollars from local currenciesbased on current exchange rates.• Cost of illness studies depend on a set of sources and assumptions. We have conductedcomprehensive sensitivity analyses in which we use different source data or vary assumptions tosee how this would affect the results (available in the full Report at www.alz.co.uk/worldreport).
muriel, in the foreground, has recently been diagnosed with early onset Alzheimer’s. An emergency room nurse, shenow finds herself, at 58, the recipient of a different form of care delivery. muriel participates in a research and actionprogramme run by the Centre for memory resources and research (Cmrr) in nice, France. here she is walking withnathalie, a psychologist, during an excursion to a local park.
Alzheimer’s diseAse inTernATionAl
The GloBAl eConomiC impACT oF demenTiA
5
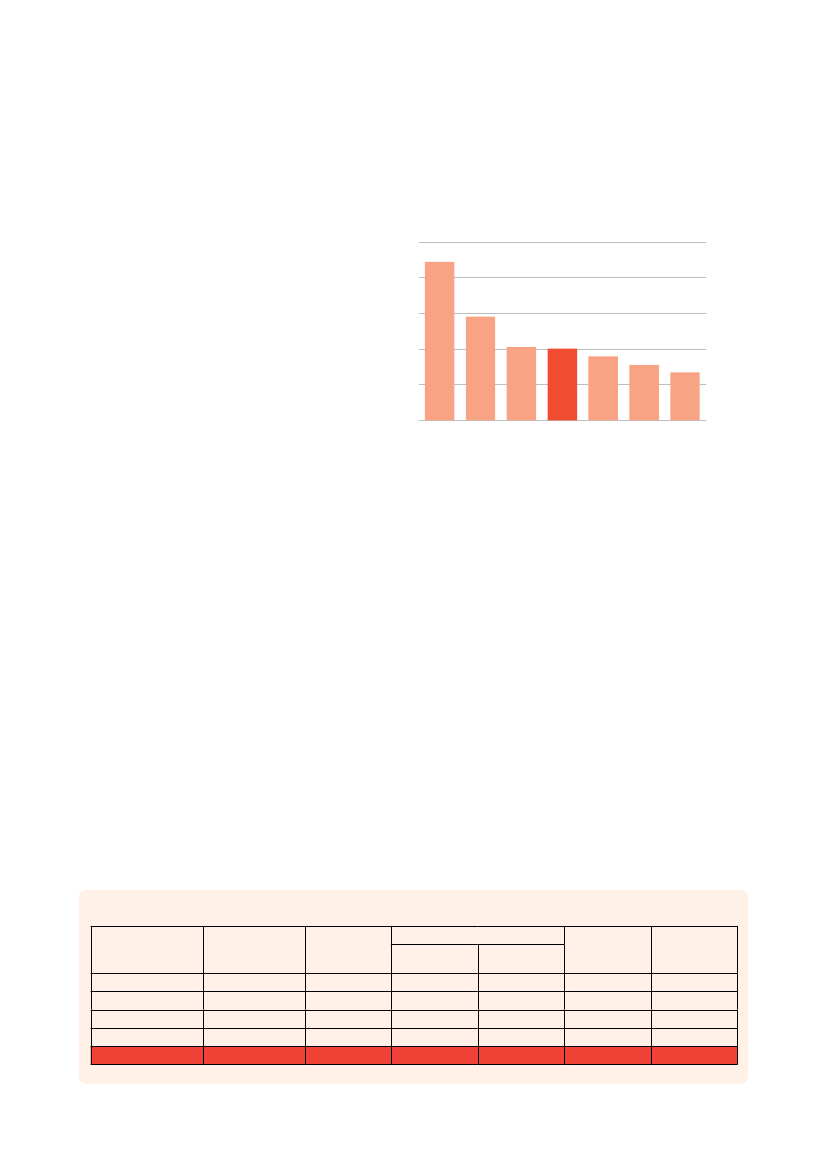
Results• The total estimated worldwide costsof dementia are US$604 billion in2010.• These costs account for around1% of the world’s gross domesticproduct, varying from 0.24% in lowincome countries, to 0.35% in lowmiddle income countries, 0.50% inhigh middle income countries, and1.24% in high income countries.• If dementia care were a country, itwould be the world’s 18th largesteconomy, ranking between Turkeyand Indonesia (figure 3). If it werea company, it would be the world’slargest by annual revenue exceedingWal-Mart (US$414 billion) and ExxonMobil (US$311 billion) (figure 2).Figure 3Cost of dementia compared to national economiesUS$ billions150012009006003000IndonesiaCanadaaBelgiumoMexicTurkeymentiSweden
Cost of dementia compared to national economies
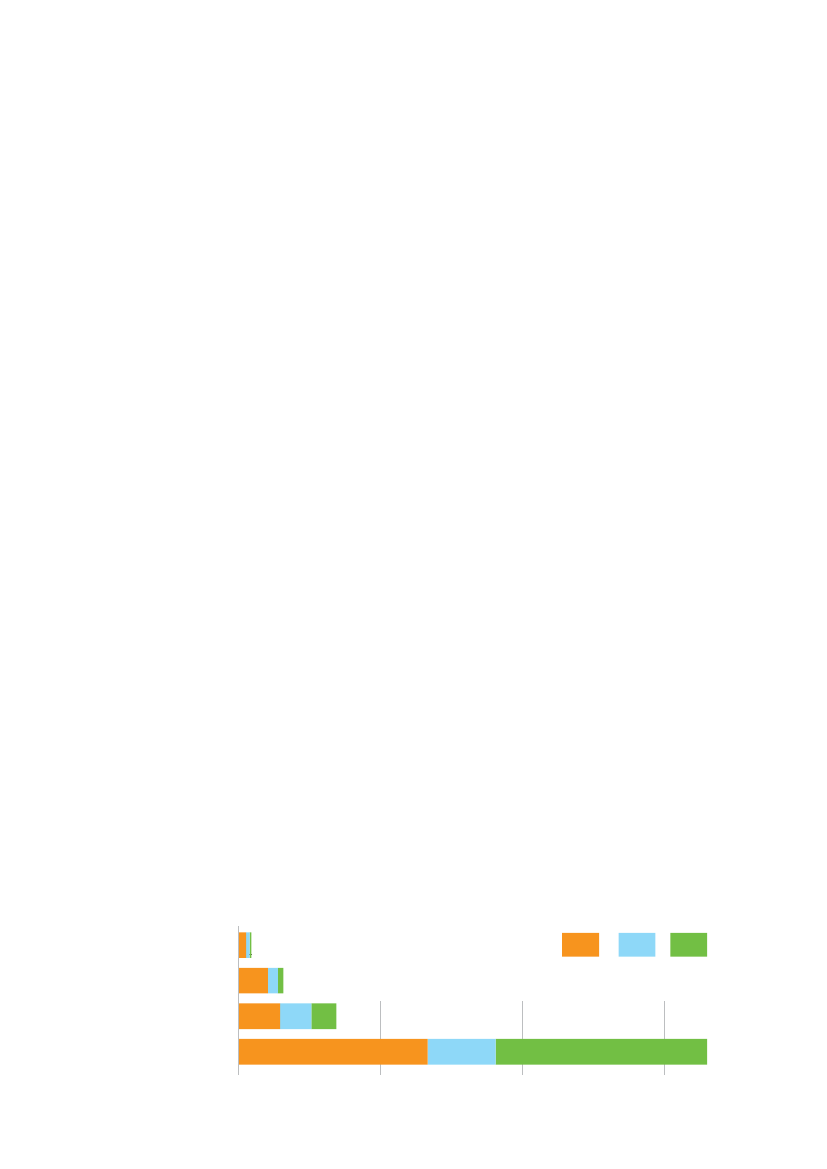
• Costs of informal care (unpaid care provided by families and others) and the direct costsof social care (provided by community care professionals and in residential home settings)contribute similar proportions (42%) of total costs worldwide, while direct medical care costsare much lower (16%).• Low income countries accounted for just under 1% of total worldwide costs (but 14% of theprevalence), middle income countries for 10% of the costs (but 40% of the prevalence) and highincome countries for 89% of the costs (but 46% of the prevalence). About 70% of the globalcosts occurred in just two regions: Western Europe and North America.• These discrepancies are accounted for by the much lower costs per person in lower incomecountries – US$868 in low income countries, US$3,109 in lower middle income, US$6,827 inupper middle income and US$32,865 in high income countries (figure 4).• In lower income countries, informal care costs predominate, accounting for 58% of all costsin low income and 65% of all costs in lower middle income countries, compared with 40% inhigh income countries. Conversely, in high income countries, the direct costs of social care(professional care in the community, and the costs of residential and nursing home care)account for the largest element of costs – nearly one half, compared with only one tenth inlower income countries.
Table 1
Aggregated costs in different World Bank income groups (billions US$)Number ofpeople withdementia5036979939520447590251636750835558717
Informalcare(all ADL)2.5218.9013.70216.77251.89
Direct costsMedical1.236.7410.4478.0096.41
Non-medical0.623.578.35243.14255.69
Total costs4.3729.2132.49537.91603.99
Percent ofGDP0.24%0.35%0.50%1.24%1.01%
Low incomeLower middle incomeUpper middle incomeHigh incomeAll
De
Alzheimer’s diseAse inTernATionAl
6
World Alzheimer reporT 2010
Table 2
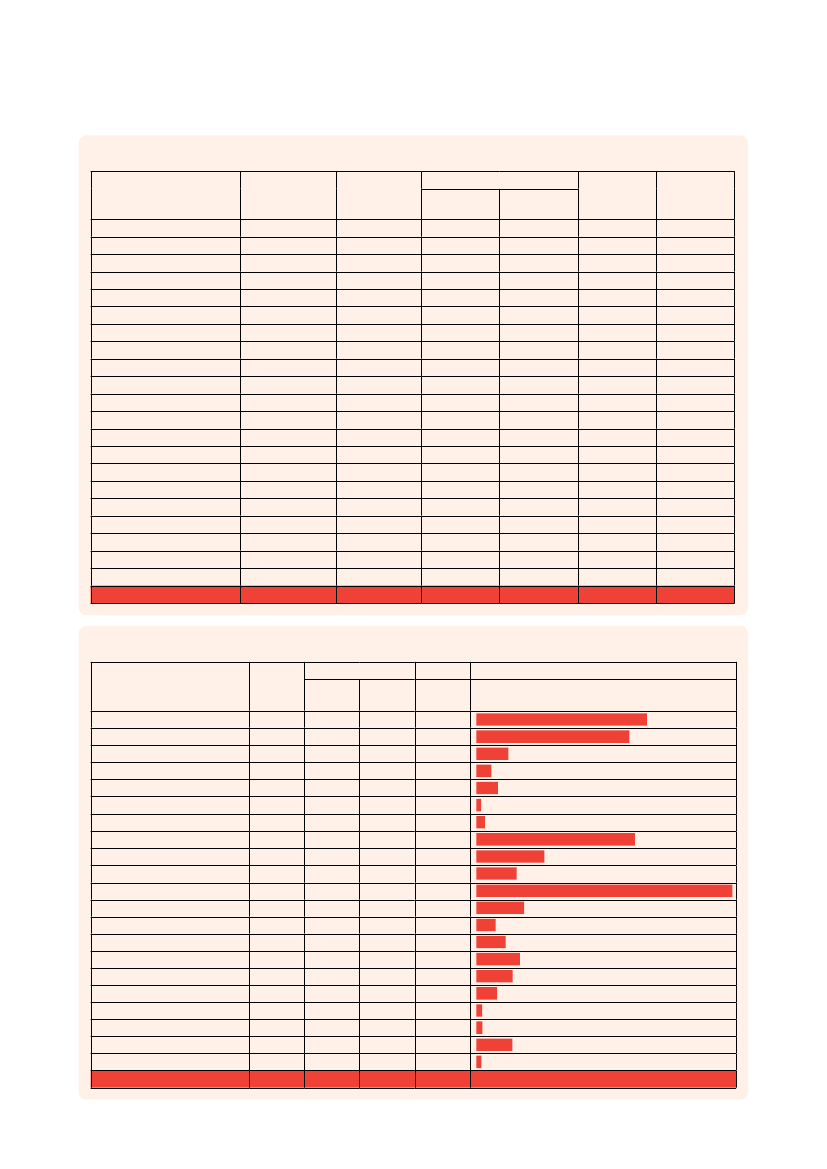
Aggregated costs in each WHO region (billions US$)Number ofpeople withdementia311,3272,826,38816,553330,1255,494,3874,475,3242,482,0766,975,5401,100,7591,869,2424,383,057327,825254,9251,185,559614,5231,054,5601,145,63367,775360,602100,733181,80335,558,717
Informal care(all ADLs)4.3034.600.070.4315.242.311.7787.058.597.9678.761.500.351.582.362.171.900.040.280.520.11251.89
Direct costsMedical0.705.230.020.284.331.161.4830.192.673.4236.830.780.312.611.422.672.050.020.080.110.0496.41
Social5.0742.290.010.242.840.570.7392.882.942.9497.450.710.282.371.292.420.540.010.040.060.02255.69
Total costs10.0882.130.100.9422.414.043.97210.1214.1914.33213.042.980.936.565.077.264.500.070.400.690.18603.99
Percentof GDP0.97%1.31%0.46%0.36%0.40%0.25%0.28%1.29%1.10%0.90%1.30%1.06%0.43%0.37%1.02%0.42%0.16%0.06%0.17%0.24%0.06%1.01%
AustralasiaAsia Pacific High IncomeOceaniaAsia CentralAsia EastAsia SouthAsia SoutheastEurope WesternEurope CentralEurope EasternNorth America High IncomeCaribbeanLatin America AndeanLatin America CentralLatin America SouthernLatin America TropicalNorth Africa / Middle EastSub-Saharan Africa CentralSub-Saharan Africa EastSub-Saharan Africa SouthernSub-Saharan Africa WestTotal
Table 3
Cost per person with dementia in each WHO region (US$)Direct costsInformalcareNon(all ADL) Medical medical13812226216296122431852149634526102650812958457232774788517515259128711595295124794328133157801242326674261183215731796884032223345702371215113751200108913352202199938382309209520572529229516601794472648289143787224111514911275586092411197084
2711
7191
Totalcosts32370290576059286240789031601301221289176674860590923663553682436881392610811122683496916986
Total costs
AustralasiaAsia Pacific High IncomeOceaniaAsia CentralAsia EastAsia SouthAsia SoutheastEurope WesternEurope CentralEurope EasternNorth America High IncomeCaribbeanLatin America AndeanLatin America CentralLatin America SouthernLatin America TropicalNorth Africa / Middle EastSub-Saharan Africa CentralSub-Saharan Africa EastSub-Saharan Africa SouthernSub-Saharan Africa WestAll
Alzheimer’s diseAse inTernATionAl
The GloBAl eConomiC impACT oF demenTiA
7
Conclusions• The scale of the global cost of dementia is explainable when one considers that around 0.5% ofthe world’s total population live with dementia.– A high proportion of people with dementia need some care, ranging from support withinstrumental activities of daily living (such as cooking or shopping), to full personal care andround the clock supervision.– In some high income countries, between one third and one half of all people with dementialive in resource- and cost-intensive residential or nursing home care facilities.– Medical care costs also tend to be relatively high for people with dementia, particularly inhigh income countries with reasonable provision of specialist care services.• Costs are lower in developing countries, both per person and societally (as a proportion ofGDP). In these regions, there is a much greater reliance on the unpaid informal care provided byfamily and others.– While wage levels are low, these are increasing rapidly, and hence the opportunity cost orreplacement cost of these informal inputs is set to rise.– In our key informant survey, we estimated that in low and middle income countries only6% of people with dementia live in care homes. However, this sector is expanding rapidly,particularly in urban settings in middle income countries, boosted by demographic andsocial changes that reduce the availability of family members to provide care.– Medical help-seeking is relatively unusual in low and middle income countries, wheredementia is often viewed as a normal part of ageing. Demand for medical care is likelyto increase in the future, with improved awareness, better coverage of evidence-basedinterventions, and, possibly, more effective treatments.• Worldwide, the costs of dementia are set to soar. We have tentatively estimated an 85%increase in costs to 2030, based only on predicted increases in the numbers of people withdementia. Costs in low and middle income countries are likely to rise faster than in high incomecountries, because, with economic development, per person costs will tend to increasetowards levels seen in high income countries, and because increases in numbers of peoplewith dementia will be much sharper in those regions.• There is an urgent need to develop cost-effective packages of medical and social care thatmeet the needs of people with dementia and their caregivers across the course of the illness,and evidence-based prevention strategies. Only by investing now in research and cost-effectiveapproaches to care can future societal costs be anticipated and managed. Governments andhealth and social care systems need to be adequately prepared for the future, and must seekways now to improve the lives of people with dementia and their caregivers.Figure 4Care costs per person with dementia in different World Bank income groups (US$)Low incomeLower middle incomeUpper middle incomeHigh income010,00020,00030,000InformalMedicalSocial
Alzheimer’s diseAse inTernATionAl
8
World Alzheimer reporT 2010
Recommendations123Alzheimer’s Disease International calls on governments to make dementia a healthpriority and develop national plans to deal with the disease.Alzheimer’s Disease International reminds governments of their obligations underthe UN Convention on the Rights of People with Disabilities, and the MadridInternational Plan for Action on Ageing to ensure access to healthcare. It callson governments to fund and expand the implementation of the World HealthOrganization (WHO) Mental Health Gap Action Plan, including the packages of carefor dementia, as one of the seven core disorders identified in the plan.Alzheimer’s Disease International requests that new investment in chronic diseasecare should always include attention to dementia. For example, the WHO GlobalReport on ‘Innovative Care for Chronic Conditions’ alerts policymakers, particularlythose in low and middle income countries, to the implications of the decreases incommunicable diseases and the rapid ageing of populations. Healthcare is currentlyorganized around an acute, episodic model of care that no longer meets the needsof patients with chronic conditions. The WHO Innovative Care for Chronic Conditionsframework provides a basis on which to redesign health systems that are fit for theirpurpose.Alzheimer’s Disease International calls on governments and other major researchfunders to act now to increase dementia research funding, including research intoprevention, to a level more proportionate to the economic burden of the condition.Recently published data from the UK suggests that a 15-fold increase is required toreach parity with research into heart disease, and a 30-fold increase to achieve paritywith cancer research. International coordination of research is needed to make thebest use of resources.Alzheimer’s Disease International calls on governments worldwide to developpolicies and plans for long-term care that anticipate and address social anddemographic trends and have an explicit focus on supporting family caregivers andensuring social protection of vulnerable people with dementia.Alzheimer’s Disease International supports HelpAge International’s call forgovernments to introduce universal non-contributory social pension schemes(www.helpage.org/Researchandpolicy/Socialprotection).Alzheimer’s Disease International calls on governments to ensure that people withdementia are eligible to receive and do receive disability benefits, where suchschemes are in operation.Jody ross, a laughter yogateacher in minneapolis, UsA,visited lakeview ranch tolead a session with residents,staff, and a few visitors. elsieagreed to participate, but atfirst all her grimaces indicatedthat she knew she wouldnot have a good time. soon,however, she changed intoan active and enthusiasticparticipant. The sessionended with this hug. everyonewas delighted and elsie andthe other residents asked tohave more such sessions.
4567
Alzheimer’s diseAse inTernATionAl
The GloBAl eConomiC impACT oF demenTiA
9
Alzheimer’s Disease InternationalAlzheimer’s Disease International (ADI) is the international federation of Alzheimer associationsthroughout the world. Each of our 73 members is a non-profit Alzheimer association supportingpeople with dementia and their families.ADI’s vision is an improved quality of life for people with dementia and their families throughoutthe world. ADI aims to build and strengthen Alzheimer associations and raise awareness aboutdementia worldwide. Stronger Alzheimer associations are better able to meet the needs of peoplewith dementia and their carers.
What we do• Support the development and activities of our member associations around the world.• Encourage the creation of new Alzheimer associations in countries where there is noorganization.• Bring Alzheimer organizations together to share and learn from each other.• Raise public and political awareness of dementia.• Stimulate research into the prevalence and impact of Alzheimer’s disease and dementia aroundthe world.
Key activities• Raising global awareness through World Alzheimer’s Day™ (21 September every year).• Providing Alzheimer associations with training in running a non-profit organization through ourAlzheimer University programme.• Hosting an international conference where staff and volunteers from Alzheimer associationsmeet each other as well as medical and care professionals, researchers, people with dementiaand their carers.• Disseminating reliable and accurate information through our website and publications.• Supporting the 10/66 Dementia Research Group’s work on the prevalence and impact ofdementia in developing countries.ADI is based in London and is registered as a non-profit organization in the USA. ADI was foundedin 1984 and has been in official relations with the World Health Organization since 1996. You canfind out more about ADI at www.alz.co.uk.
Alzheimer’s diseAse inTernATionAl
Alzheimer’s Disease International:The International Federationof Alzheimer’s Disease andRelated Disorders Societies, Inc.is incorporated in Illinois, USA,and is a 501(c)(3) not-for-profitorganization
Alzheimer’s Disease International64 Great Suffolk StreetLondon SE1 0BLUKTel: +44 20 79810880Fax: +44 20 79282357www.alz.co.uk